
Abstract
Introduction
Exenatide is a new antidiabetic glucagon-like peptide-1 receptor agonist. In addition to its hypoglycemic effect, exenatide may have a potential protective benefit on vascular endothelial function. This study attempted to compare the effects of exenatide and traditional antidiabetic drug metformin treatment on endothelial function in overweight patients with type 2 diabetes.
Methods
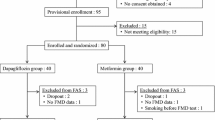
Ninety overweight patients with newly diagnosed type 2 diabetes were recruited; 45 patients received exenatide (Exe) treatment and 45 patients received metformin (Met) treatment for 12 weeks. The control groups included 37 overweight and 24 non-overweight individuals. The parameters of glucose and lipid metabolism and endothelial function were measured before and after treatment. Vascular endothelial dysfunction was measured by reactive hyperemia index.
Results
Newly diagnosed patients with type 2 diabetes had more serious vascular endothelial dysfunction than both overweight and normal-weight control groups. The levels of body mass index, glucose, HbA1c, homeostasis model assessment insulin resistance, and homeostasis model assessment β-cell function were improved significantly by both exenatide and metformin treatment. Both exenatide and metformin treatment can improve vascular endothelial function (Exe group: 1.67 ± 0.52 vs 1.98 ± 0.67, P < 0.05; Met group: 1.68 ± 0.29 vs 1.82 ± 0.24, P < 0.05). Exenatide treatment was no less effective than metformin in improving endothelial function (0.31 ± 0.70 vs 0.13 ± 0.24, P > 0.05).
Conclusions
Newly diagnosed patients with type 2 diabetes may have vascular endothelial dysfunction. Both exenatide and metformin treatment can improve vascular endothelial dysfunction, and exenatide was no less effective than metformin treatment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The number of patients with type 2 diabetes mellitus (T2DM) has increased significantly in the world with changes of lifestyle [1]. The acute and chronic complications of T2DM seriously threaten the health of patients. T2DM is also an important risk factor of cardiovascular and cerebrovascular diseases [2]. Therefore, the cardiovascular protective effects of antidiabetic drugs need to be evaluated along with the hypoglycemic activity. Among a wide variety of antidiabetic drugs, metformin is one of the most important because of its cardiovascular protective effects independent of glucose control [3]. Glucagon-like peptide-1 receptor agonist exenatide is a new kind of antidiabetic drug. In previous studies, exenatide decreased the risk of atherosclerosis by reducing weight and inflammatory factors and increasing the expression of adiponectin [4,5,6].
Endothelial dysfunction is a key step in patients with T2DM with atherosclerosis. Studies have shown that endothelial dysfunction occurs even in patients with impaired glucose tolerance or early-stage T2DM [7, 8]. The main mechanism is decreasing activity of endothelial nitric oxide synthase (eNOS) and the reduction of nitric oxide (NO) generation. NO is the major endothelium-derived vasodilator factor and an important anti-atherosclerosis agent. T2DM, dyslipidemia, smoking, and hypertension can induce oxidative stress and decrease eNOS activity and NO production [9]. The result is chronic endothelial dysfunction. In basic research, exenatide improved endothelial dysfunction by inhibiting the expression of monocyte chemotactic protein-1 (MCP-1) and vascular cell adhesion molecule-1 (VCAM-1) and promoting the phosphorylation of eNOS [5, 10]. Metformin also promoted the activity of eNOS by activating the AMPK signal pathway [11]. So we hypothesized that exenatide and metformin treatment would improve endothelial dysfunction in newly diagnosed patients with T2DM.
This study tried to compare the effects of exenatide and metformin treatment on endothelial function in overweight patients with type 2 diabetes and analyze the correlations between endothelial function and other metabolic parameters.
Methods
Subjects
A total of 90 newly diagnosed overweight patients with T2DM and 61 age- and sex-matched healthy controls were recruited from the Beijing Chao-yang Hospital between June 2013 and June 2017. Diagnostic criteria for T2DM were based on the World Health Organization criteria of 1999. Overweight was defined as body mass index (BMI) ≥ 24 kg/m2. Patients were excluded if they had a history of type 1 diabetes mellitus, diabetic ketoacidosis, diabetic hyperosmolar coma, nephropathy, acute or chronic hepatic and renal diseases, severe anemia, acute myocardial infarction, or stoke. No participants were under the treatment of antidiabetic, antihypertensive, or antidyslipidemic drugs.
Study Design
Patients with T2DM were divided into two groups according to the treatment. The exenatide (Exe) group included 45 patients with T2DM undergoing 12 weeks of exenatide (Byetta, Eli Lilly Company, USA) treatment as 5 µg bid for 4 weeks (subcutaneous injection), followed by 10 µg bid for 8 weeks. The metformin (Met) group included the other 45 patients who received 12 weeks of metformin (Glucophage, Bristol-Myers Squibb Company, USA) as 500 mg bid or tid (oral administration). Healthy control subjects were divided into two groups according to whether their BMI was greater than 24 kg/m2 (overweight control group, n = 37, non-overweight control group, n = 24).
Compliance with Ethics Guidelines
Written consent was obtained from all subjects. All procedures were conducted in accordance with the Declaration of Helsinki and the study was approved by the ethics committee of the Beijing Chao-yang Hospital.
Laboratory Measurements and Determination for Endothelial Function
All subjects underwent a screening assessment at baseline, including measurements of weight, height, total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), triglycerides (TG), fasting plasma glucose (FPG), and fasting serum insulin (FINS). BMI was calculated as weight (kg)/height2 (m2). The homeostasis model assessment for insulin resistance (HOMA-IR) and homeostasis model assessment for beta cell function (HOMA-B) were used to estimate insulin resistance and beta cell function. HOMA-IR and HOMA-B were calculated using the following equations: HOMA-IR = FPG (mmol/L) × FINS (mU/L) /22.5; HOMA-B = 20 × FINS (mU/L)/[FPG (mmol/L) − 3.5] [12]. FPG, TC, HDL-C, LDL-C, and TG were measured on a Dade-Behring Dimension RXL Autoanalyzer (Dade Behring Diagnostics, Marburg, Germany). FINS and C-peptide were measured on a Beckman Access 2 (Fullerton, CA). HbA1c was estimated by high-performance liquid chromatography using an HLC-723G7 analyzer (Tosoh Corp., Japan).
Endothelial function assessment was measured by digital reactive hyperemia index (RHI; EndoPAT 2000, Itamar Medical, Caesarea, Israel). After patients rested for 30 min in the supine position, PAT probes were placed on the index finger of each hand and tested the baseline pulse amplitude for 5 min. After 5 min, the blood pressure cuff was inflated to 60 mmHg above the systolic pressure or 200–300 mmHg for 5 min. Following cuff release, the change in pulse amplitude during reactive hyperemia was measured for 5–10 min. RHI is the ratio of the hyperemic and baseline pulse amplitude after the control arm correction. Endothelial function test was tested in a fasting state.
After the assessment, patients with T2DM underwent 12 weeks of antidiabetic treatment. Laboratory and endothelial function measurements were repeated after 12 weeks of exenatide or metformin treatment. Changes in every parameter before and after treatment were expressed as delta parameter: Δ parameter = parameter (after treatment) − parameter (baseline).
Statistical Analysis
Data were analyzed using SPSS 21.0 (SPSS, Inc., Chicago, IL). Continuous data such as age, BMI, TC, LDL-C, HDL-C, FPG, FINS, RHI, and HbA1c were expressed as mean ± SD. Independent-sample t test was used in the baseline comparisons between type 2 diabetes mellitus patients and healthy controls. Paired-sample t test was used in the comparison between before and after the treatment of metformin or exenatide. Non-normally distributed variables such as TG, HOMA-IR, and HOMA-B were expressed as median (interquartile range). They were analyzed by the Mann-Whitney U test between type 2 diabetes mellitus patients and healthy controls. Wilcoxon test was used in the comparison between before and after the treatment of metformin or exenatide. Spearman’s rank correlation was used to assess the relationship of data. All tests were two-tailed, and P < 0.05 was considered statistically significant.
Results
Baseline Characteristics of T2DM Patients and Control Subjects
Baseline characteristics of patients with T2DM and control subjects are summarized in Table 1. Patients with T2DM had significantly higher FPG, HbA1c, and TG levels and lower HOMA-B than overweight and non-overweight control groups. The difference in HOMA-IR occurred only in the comparison between patients with T2DM and non-overweight control group. The baseline endothelial function—RHI—is shown in Fig. 1. Patients with T2DM had significantly lower RHI than control groups (T2DM: 1.67 ± 0.42 vs O-Con: 1.95 ± 0.46; N-Con: 2.04 ± 0.59, P < 0.05).

RHI between T2DM, overweight and non-overweight controls before treatment. T2DM type 2 diabetes mellitus, O-Con overweight control group, N-Con non-overweight control group, RHI reactive hyperemia index
Correlations Between RHI and Other Parameters Before Antidiabetic Treatment
Before antidiabetic treatment, fasting RHI was negatively correlated with HbA1c (r = − 0.202, P < 0.05, Fig. 2a), FPG (r = − 0.155, P < 0.05, Fig. 2b), HOMA-IR (r = − 0.172, P < 0.05, Fig. 2c), and LDL-C (r = − 0.200, P < 0.05, Fig. 2d).

Correlations between RHI and a HbA1c, b FPG, c LDL-C, and d HOMA-IR. RHI reactive hyperemia index, BMI body mass index, HOMA-IR homoeostasis model assessment for insulin resistance, LDL-C low density lipoprotein cholesterol
Comparisons of the Effect of Exenatide and Metformin Antidiabetic Treatment on Endothelial Function and Metabolism of Glucose and Lipids
Changes in metabolic characteristics and endothelial function are summarized in Tables 2 and 3 and Fig. 3. Patients with T2DM were divided into two groups according to the treatment (Exe group and Met group). Age, height, weight, BMI, TC, TG, LDL-C, HDL-C, HbA1c, FINS, HOMA-IR, HOMA-B, and RHI were similar in two groups (Table 1). Both exenatide and metformin can significantly reduce FPG, HbA1c, and HOMA-IR and increase HOMA-B. In addition to their glucose-reducing effect, both exenatide and metformin can significantly improve the RHI of patients with T2DM (Exe group: 1.67 ± 0.52 vs 1.98 ± 0.67, P < 0.05, Fig. 3a; Met group: 1.68 ± 0.29 vs 1.82 ± 0.24, P < 0.05, Fig. 3b). In a comparison of the effect of the two drugs, exenatide was more effective in reducing BMI and weight (Table 3). There was no significant difference between exenatide and metformin in improving RHI levels (0.31 ± 0.70 vs 0.13 ± 0.24, P > 0.05, Table 3).

Changes in reactive hyperemia index in the a exenatide group and b metformin group
Discussion
From our research, we found that endothelial dysfunction is associated with insulin resistance and β-cell dysfunction in newly diagnosed patients with T2DM. In addition to the hypoglycemic effect, exenatide and metformin can improve insulin resistance and partly restore β-cell function. Regarding vascular endothelial function, there was no significant difference between exenatide and metformin treatment.
In the analysis of endothelial function, we used RHI (EndoPAT2000, Israel). RHI is an operator-independent method to quantify endothelial function. It is NO-dependent and associated with coronary artery blood flow and multiple cardiovascular risk factors. RHI is also useful for the assessment of cardiac events [13]. In our study, patients with T2DM had lower RHI than overweight and non-overweight controls. It is suggested that vascular endothelial dysfunction might occur even in the early period of T2DM without clear cardiovascular disease. This was consistent with previous research [8, 14]. Besides the effect of hyperglycemia, patients with T2DM always have multiple risk factors of endothelial dysfunction such as hyperlipidemia, smoking, obesity, and insulin resistance. These long-term chronic lesions may lead to the endothelial dysfunction that occurred even in newly diagnosed patients with T2DM.
In the correlation analysis, RHI was negatively correlated with the LDL-C, FPG, HbA1c, and HOMA-IR. LDL-C is the one of the most important risk factors for cardiovascular disease. Diabetic dyslipidemia is characterized by elevated LDL-C and TG. In our previous studies, we found that LDL-C was negatively correlated with endothelial function in both T2DM and healthy controls. Basic medical research has shown that LDL-C increased oxidative stress and impaired the activity of the eNOS system [15]. Insulin resistance was reported as a risk factor of endothelial dysfunction. In the insulin-resistance condition, the balance between NO-dependent vasodilator and endothelin-1-dependent vasoconstrictor of insulin is impaired. The imbalance of NO and endothelin-1 secretion may cause the endothelial dysfunction [16, 17].
During the antidiabetic treatment, both exenatide and metformin could improve the metabolism of glucose and lipid. They decreased insulin resistance and recovered β-cell function in patients with T2DM.Exenatide had better efficacy in reducing weight and BMI than metformin. These findings are common in antidiabetic treatment [18, 19]. Our results suggested that exenatide improved the endothelial dysfunction in newly diagnosed patients with T2DM, and the effect was not inferior to single metformin. In the United Kingdom Prospective Diabetes Study, metformin treatment showed a greater effect for any diabetes-related endpoint, all-cause mortality, and stroke than insulin or sulfonylureas [3]. Previous studies had proved that long-term metformin treatment improved the endothelial function and decreased inflammatory factors such as sICAM-1, sVCAM-1, C reactive protein, and von Willebrand factor [20]. In patients with T2DM, metformin also significantly improved the risk factors of endothelial dysfunction such as hyperglycemia, LDL-C, obesity, and insulin resistance [21]. On the other hand, our research on human umbilical vein endothelial cells (HUVECs) found that metformin protected glucose-induced endothelial dysfunction through the eNOS recoupling via the AMPK-dependent pathway [11]. Moreover, another study suggested that metformin protects endothelial function by inhibiting endoplasmic reticulum stress in obese mice through the PPAR-δ pathway [22]. These results showed that the effects of metformin on endothelial function may not completely rely on the improvement of glucose and lipid metabolism.
Exenatide is an antidiabetic glucagon-like peptide-1 receptor agonist. It promotes glucose-dependent insulin secretion. Exenatide also improves insulin resistance and obesity by delaying gastric emptying and reducing weight gain. No conclusive evidence proves the protective effect for cardiovascular disease of exenatide. However, some studies have suggested that exenatide protects endothelial cell function in patients with T2DM. In Gurkan et al.’s study, exenatide improved endothelial dysfunction and inhibited the inflammatory factors such as hsCRP and MCP-1 [23]. In the patients with impaired glucose tolerance, a single injection of exenatide also improved the endothelial function after eating a meal [14]. But another GLP-1 receptor agonist liraglutide did not affect endothelial function in a randomized controlled trial [24]. The reason may be due to the difference in the evaluation of endothelial function. Another class of antidiabetes drug dipeptidyl peptidase-4 inhibitors, which prevent the degradation of GLP-1, had a similar effect on endothelial on the amelioration of endothelial dysfunction in type 2 diabetes patients [25]. In addition to relieving the damage to the endothelial cell from hyperglycemia and hyperlipidemia, researchers have found that exenatide could upregulate eNOS bioactivity via the AMPK/PI3 K-Akt/eNOS pathway in HUVEC cells independent of hypoglycemic effects [5]. In our study, 12-week single exenatide treatment had similar effects on the endothelial function as with metformin, which was consistent with previous studies [23, 26].
Our research found that the non-overweight control group had higher RHI than overweight controls, but not significantly. Overweight controls had more serious insulin resistance and obesity than non-overweight patients. Obesity is associated with endothelial dysfunction through several mechanisms, including enhanced oxidative stress. Adipose tissue is an active metabolic organ that produces reactive oxygen species, and the macrophages around it release chemoattractant protein and inflammatory cytokines [27, 28]. Moreover, obesity leads to the decrease of adiponectin which exerts anti-inflammatory and anti-atherosclerosis effects [29]. In our research, the small sample size may reduce the difference of RHI between the overweight and non-overweight groups.
This research has many limitations. First, we used the HOMA-IR to estimate insulin resistance. HOMA-IR is not a precise index compared with the euglycemic clamp. However, the euglycemic clamp test is not suitable for clinical service. Second, we did not consider patients’ smoking history. Smoking is a risk factor of vascular endothelial dysfunction. Thirdly, because of the discomfort in the gastrointestinal tract, some patients of metformin group accepted lower dose of metformin (500 mg bid). Different doses might affect the effect of metformin on plasma glucose and endothelial function. Finally, this research was not a strict randomized controlled trial. These limitations will be solved in the next step of our research in the future.
Conclusions
Endothelial dysfunction might occur even in the early period of T2DM without clear cardiovascular disease. RHI was negatively correlated with LDL-C, HbA1c, FPG, and HOMA-IR. In addition to the antidiabetic effect, both exenatide and metformin therapy had positive effects on endothelial dysfunction in newly diagnosed patients with T2DM. There was no significant difference between exenatide and metformin in the improvement of endothelial function.
References
Xu Y, Wang L, He J, et al. Prevalence and control of diabetes in Chinese adults. JAMA. 2013;310:948–59.
Gu K, Cowie CC, Harris MI. Mortality in adults with and without diabetes in a national cohort of the U.S. population, 1971–1993. Diabetes Care. 1998;21:1138–45.
UK Prospective Diabetes Study (UKPDS) Group. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet. 1998;352:854–865.
Koska J, Sands M, Burciu C, et al. Exenatide protects against glucose- and lipid-induced endothelial dysfunction: evidence for direct vasodilation effect of GLP-1 receptor agonists in humans. Diabetes. 2015;64:2624–35.
Wei R, Ma S, Wang C, et al. Exenatide exerts direct protective effects on endothelial cells through the AMPK/Akt/eNOS pathway in a GLP-1 receptor-dependent manner. Am J Physiol Endocrinol Metab. 2016;310:E947–57.
Kim CLT, Hosaka T, Yoshida M, et al. Exendin-4, a GLP-1 receptor agonist, directly induces adiponectin expression through protein kinase A pathway and prevents inflammatory adipokine expression. Biochem Biophys Res Commun. 2009;390:613–8.
Shin JY, Lee HR, Lee DC. Increased arterial stiffness in healthy subjects with high-normal glucose levels and in subjects with pre-diabetes. Cardiovasc Diabetol. 2011;10:30.
Su Y, Liu XM, Sun YM, et al. Endothelial dysfunction in impaired fasting glycemia, impaired glucose tolerance, and type 2 diabetes mellitus. Am J Cardiol. 2008;102:497–8.
Montezano AC, Touyz RM. Reactive oxygen species and endothelial function–role of nitric oxide synthase uncoupling and Nox family nicotinamide adenine dinucleotide phosphate oxidases. Basic Clin Pharmacol Toxicol. 2012;110:87–94.
Ishibashi Y, Matsui T, Takeuchi M, Yamagishi S. Glucagon-like peptide-1 (GLP-1) inhibits advanced glycation end product (AGE)-induced up-regulation of VCAM-1 mRNA levels in endothelial cells by suppressing AGE receptor (RAGE) expression. BiochemBiophys Res Commun. 2010;391:1405–8.
An H, Wei R, Ke J, et al. Metformin attenuates fluctuating glucose-induced endothelial dysfunction through enhancing GTPCH1-mediated eNOS recoupling and inhibiting NADPH oxidase. J Diabetes Complic. 2016;30:1017–24.
Matthews DR, Hosker JP, Rudenski AS, et al. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28:412–9.
Hamburg NM, Keyes MJ, Larson MG, et al. Cross-sectional relations of digital vascular function to cardiovascular risk factors in the Framingham Heart Study. Circulation. 2008;117:2467–74.
Koska J, Schwartz EA, Mullin MP, Schwenke DC, Reaven PD. Improvement of postprandial endothelial function after a single dose of exenatide in individuals with impaired glucose tolerance and recent-onset type 2 diabetes. Diabetes Care. 2010;33:1028–30.
Yu J, Han JL, He LY, et al. Low density lipoprotein cholesterol level inversely correlated with coronary flow velocity reserve in patients with type 2 diabetes. J Geriatr Cardiol. 2013;10:159–64.
Del TS, Gaggini M, Daniele G, et al. Insulin resistance and endothelial dysfunction: a mutual relationship in cardiometabolic risk. Curr Pharm Des. 2013;19:2420–31.
Muniyappa R, Sowers JR. Role of insulin resistance in endothelial dysfunction. Rev Endocr Metab Disord. 2013;14:5–12.
Hu Y, Liu J, Zhang H, et al. Exenatide treatment decreases fasting fibroblast growth factor 21 levels in patients with newly diagnosed type 2 diabetes mellitus. Diabetes Metab. 2016;42:358–63.
Yuan GH, Song WL, Huang YY, Guo XH, Gao Y. Efficacy and tolerability of exenatide monotherapy in obese patients with newly diagnosed type 2 diabetes: a randomized, 26 weeks metformin-controlled, parallel-group study. Chin Med J (Engl). 2012;125:2677–81.
Ghosh S, Lakshmanan AP, Hwang MJ, et al. Metformin improves endothelial function in aortic tissue and microvascular endothelial cells subjected to diabetic hyperglycaemic conditions. Biochem Pharmacol. 2015;98:412–21.
Fan H, Sun X, Zhang H, et al. Effect of metformin on fibroblast growth factor-21 levels in patients with newly diagnosed type 2 diabetes. Diabetes Technol Ther. 2016;18:120–6.
Cheang WS, Tian XY, Wong WT, et al. Metformin protects endothelial function in diet-induced obese mice by inhibition of endoplasmic reticulum stress through 5’ adenosine monophosphate-activated protein kinase-peroxisome proliferator-activated receptor delta pathway. Arterioscler Thromb Vasc Biol. 2014;34:830–6.
Gurkan E, Tarkun I, Sahin T, Cetinarslan B, Canturk Z. Evaluation of exenatide versus insulin glargine for the impact on endothelial functions and cardiovascular risk markers. Diabetes Res Clin Pract. 2014;106:567–75.
Nomoto H, Miyoshi H, Furumoto T, et al. A comparison of the effects of the GLP-1 analogue liraglutide and insulin glargine on endothelial function and metabolic parameters: a randomized, controlled trial sapporo athero-incretin study 2 (SAIS2). PLoS One. 2015;10:e0135854.
Torimoto K, Okada Y, Tanaka Y. Type 2 diabetes and vascular endothelial dysfunction. J UOEH. 2018;40:65–75.
Kelly AS, Bergenstal RM, Gonzalez-Campoy JM, Katz H, Bank AJ. Effects of exenatide vs. metformin on endothelial function in obese patients with pre-diabetes: a randomized trial. Cardiovasc Diabetol. 2012;11:64.
Esposito K, Nicoletti G, Giugliano D. Obesity, cytokines and endothelial dysfunction: a link for the raised cardiovascular risk associated with visceral obesity. J Endocrinol Invest. 2002;25:646–9.
Virdis A. Endothelial dysfunction in obesity: role of inflammation. High Blood Press Cardiovasc Prev. 2016;23:83–5.
El HM, Mamdouh M, Shaban S, et al. Adipokines: potential therapeutic targets for vascular dysfunction in type II diabetes mellitus and obesity. J Diabetes Res. 2017;2017:8095926.
Acknowledgements
We thank all of the residents who participated in the study.
Funding
This work was supported by grants from the Capital Clinical Research Foundation of Beijing Municipal Commission of Science and Technology (Z131107002213024) to Yuan Xu. The article processing charges were funded by the authors.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval for the version to be published.
Disclosures
Yanjin Hu, Jia Liu, Guang Wang, and Yuan Xu have nothing to disclose.
Compliance with Ethics Guidelines
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the 1964 Declaration of Helsinki, as revised in 2013. This research protocol was approved by the ethics committee of Beijing Chao-yang hospital. Informed consent was obtained from all patients for being included in the study.
Data Availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced digital features
To view enhanced digital features for this article go to https://doi.org/10.6084/m9.figshare.6205244.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Hu, Y., Liu, J., Wang, G. et al. The Effects of Exenatide and Metformin on Endothelial Function in Newly Diagnosed Type 2 Diabetes Mellitus Patients: A Case–Control Study. Diabetes Ther 9, 1295–1305 (2018). https://doi.org/10.1007/s13300-018-0435-z
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13300-018-0435-z