
Abstract
Purpose of study
Advanced uterovaginal prolapse can significantly affect the quality of life in women and usually requires surgical management. McCall’s culdoplasty (M) or sacrospinous fixation (SSF) are done at the time of vaginal hysterectomy with pelvic floor repair (VHPFR) to reduce recurrence, but recurrence rates of 15% and 33% have been reported with these procedures respectively. We hypothesize that combining VH-PFR with both McCall’s culdoplasty and sacrospinous fixation (VH-PFR-M-SSF) may decrease recurrence rates compared to VH-PFR-M without significantly affecting other perioperative outcomes.
Methods
All patients with advanced uterovaginal prolapse and willing for VH-PFR at our institute from January 2015 to March 2018 were included after informed consent, except for medically unfit women and those preferring alternative management. We conducted a case control study comparing VH-PFR-M and VH-PFR-M-SSF with a follow-up period of 24 months. Qualitative and quantitative data were statistically analysed and Odds ratio and 95% Confidence interval was calculated. Kaplan Meier Curve was drawn and Log Rank test was used to compare recurrence.
Results
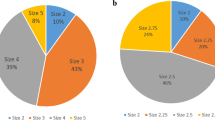
Out of 174 patients who underwent surgery in the study period, 131 patients (75.28%) underwent VH-PFR-M and 43 patients (24.71%) underwent VH-PFR-M-SSF. Both groups were comparable for age, body mass index, parity, postmenopausal status, comorbidities and aggravating factors. Patients with higher stage of prolapse were more in group 2 (p < 0.001). There were no intraoperative complications or postoperative surgical interventions in either group. The duration of surgery was not significantly different. Change in haematocrit was more in group 2 but no patient required blood transfusion. There was no statistically significant difference in recurrence rates between the 2 groups.
Conclusion
The procedure (VH PFR M-SSF) is safe and affordable with good results in Stage 3 with advanced bulge and stage 4 prolapse.


Similar content being viewed by others


References
Tseng L-H, Chen I, Chang S-D, et al. Modern role of sacrospinous ligament fixation for pelvic organ prolapse surgery—A systemic review. Taiwan J Obstet Gynecol. 2013;52(3):311–7.
Wan OY, Chan SS, Cheung RY, et al. Mesh-related complications from reconstructive surgery for pelvic organ prolapse in Chinese patients in Hong Kong. Hong Kong Med J Xianggang Yi Xue Za Zhi. 2018;24(4):369–77.
Zhang H, Zhu L, Xu T, et al. Utilize the simplified POP-Q system in the clinical practice of staging for pelvic organ prolapse: comparative analysis with standard POP-Q system. Zhonghua Fu Chan Ke Za Zhi. 2016;51(7):510–4.
Pax C-M. Vaginale Prolapshysterektomie mit Scheidengrundfixation und Zystozelenkorrektur. 2016 [cited 2019 Feb 3]; Available from: https://refubium.fu-berlin.de/handle/fub188/2991
Heft JS, Adam RA. Apical Prolapse: Is There a Best Approach? Curr Bladder Dysfunct Rep. 2018;13(3):101–10.
Ağaçayak E, Yaman Tunç S, İçen MS, et al. Should we add unilateral sacrospinous ligament fixation to vaginal hysterectomy in management of stage 3 and stage 4 pelvic organ prolapse? Turk J Obstet Gynecol. 2015;12(3):144–50.
Alas A, Chandrasekaran N, Devakumar H, et al. Advanced uterovaginal prolapse: is vaginal hysterectomy with McCall culdoplasty as effective as in lesser degrees of prolapse? Int Urogynecology J. 2018;29(1):139–44.
Lee D, Chang J, Zimmern PE. Iatrogenic Pelvic Pain: Surgical and Mesh Complications. Phys Med Rehabil Clin N Am. 2017;28(3):603–19.
Vitale SG, Laganà AS, Noventa M, et al. Transvaginal Bilateral Sacrospinous Fixation after Second Recurrence of Vaginal Vault Prolapse: Efficacy and Impact on Quality of Life and Sexuality. BioMed Res Int [Internet]. 2018 Feb 28 [cited 2019 Feb 3];2018. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5851336/
Al-Badr A, Perveen K, Al-Shaikh G. Evaluation of Sacrospinous Hysteropexy vs. Uterosacral Suspension for the Treatment of Uterine Prolapse: A Retrospective Assessment: SSHP vs. USS for Uterine Prolapse. LUTS Low Urin Tract Symptoms. 2017;9(1):33–7.
Fairchild PS, Kamdar NS, Berger MB, et al. Rates of colpopexy and colporrhaphy at the time of hysterectomy for prolapse. Am J Obstet Gynecol. 2016;214(2):262.
Funding
This article was internally funded by hospital resources.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Ethical Approval
This research involved human participants. The study has been conducted after approval from Ethical and Research committee of Believers Church Medical College, Thiruvalla, Kerala, India. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Informed consent
Written Informed Valid consent was obtained from all patients prior to the procedure.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Dr. Deepa Rajan is a Consultant Gynaecologic Oncologist, Laparoscopic Gynaecologist, and Assistant Professor in Department of Obstetrics and Gynaecology at Believers Church Medical College Hospital, Thiruvalla, Kerala.
Rights and permissions
About this article

Cite this article
Rajan, D., Varghese, P., Roy, M. et al. Is performing sacrospinous fixation with vaginal hysterectomy and McCall’s culdoplasty for advanced uterovaginal prolapse preferable over McCall’s culdoplasty alone?. J Obstet Gynecol India 70, 57–63 (2020). https://doi.org/10.1007/s13224-019-01265-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13224-019-01265-9