
Abstract
Carrier screening for autosomal recessive variants has become a cornerstone of community and public health genetics. While the first carrier screening programs were confined to conditions with relatively high prevalence, and hence well-known carrier frequency, the number of candidate genes has increased greatly since the advent of high-throughput DNA sequencing technologies. The epidemiological database of the ensuing gene panels is mostly sparse, and judgement of their performance is, therefore, anything but straightforward. We therefore derived estimates of the carrier detection probabilities among non-consanguineous and consanguineous couples as expected using the ‘Tier 3’ carrier screening gene panel recently recommended by the American College of Medical Genetics (ACMG). For non-Finnish Europeans, the respective estimate for unrelated couples equals 0.63%, implying that the ACMG Tier 3 panel accounts for over 90% of the genetic load for autosomal recessive diseases in this population. Among the offspring of first cousins, the corresponding incidence is expected to be tenfold higher, an increase still consistent with previous estimates of the overall risk of birth defects for this type of mating. Our considerations are intended to aid the implementation of carrier screening programs and to provide additional support to reproductive counselling and to obtaining informed consent.
Similar content being viewed by others

Carrier screening for autosomal recessive variants has become a cornerstone of community and public health genetics (Antonarakis 2019; Cornel et al. 2021). Its primary and often overlapping goals are disease prevention (Christianson and Modell 2004) and facilitation of reproductive decision-making (Henneman et al. 2016). The first carrier screening programs, which started in the 1970s, were confined to a few clinically severe conditions of high prevalence in particular ethnic groups or geographic regions such as Tay-Sachs disease in Ashkenazi Jews (Kaback et al. 1993) and beta-thalassemia in the Mediterranean (Cao et al. 1997). Even when cystic fibrosis carrier screening was introduced as the first pan-ethnic such endeavour in the 1990s (Castellani et al. 2010), the existing programs still targeted highly selected conditions so that their performance, measured in terms of carrier detection probabilities, could be inferred reliably from available epidemiological data. With the advent of high-throughput DNA sequencing technologies, however, the number of candidate genes for screening has increased greatly, and the coverage of current carrier screening programs ranges from a handful of genes (Gregg et al. 2021) via several hundred genes (Bell et al. 2011) to whole exomes (Kirk et al. 2019). The epidemiological database of these panels, however, is mostly sparse, and the judgement of their performance is anything but straightforward.
A recently published American College of Medical Genetics (ACMG) practice resource (Gregg et al. 2021) reported carrier frequencies for recessive pathogenic variants in 86 key autosomal genes (‘Tier 3 genes’), as derived from gnomAD v2.0.2 (https://gnomad.broadinstitute.org/). We evaluated this list in terms of its potential to identify at-risk couples (Schmidtke and Krawczak 2022) and concluded that the ACMG Tier 3 genes cover more than 50% of the autosomal recessive ‘genetic load’ of pairs of unrelated individuals.
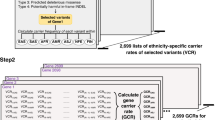
Notably, the ACMG practice resource (Gregg et al. 2021) was based upon an earlier report by Guo and Gregg (2019) that contained the specific gnomAD-derived carrier frequencies for autosomal recessive variants in six different human ancestries, namely Africans (AFR), Hispanics (AMR), East Asians (EAS), South Asians (SAS), Non-Finnish Europeans (NFE) and Ashkenazi Jews (ASJ). Similar to our own analysis (Schmidtke and Krawczak 2022), Guo and Gregg (2019) also clarified that, under the assumption of stochastic independence between genes, the probability of both in an unrelated couple being simultaneous carriers of variants in at least one of n genes (henceforth referred to as the ‘couple carrier detection probability’) can be calculated from known gene-specific carrier frequencies, fi, as
Briefly, \(1-{f}_{i}^{2}\) equals the probability that at least one in an unrelated couple is not a mutation carrier for the ith gene. Owing to stochastic independence, multiplication of these terms (symbolized by capital Greek letter Π) yields the overall probability of a lack of simultaneous carriership for all genes combined i.e. the complement of the sought-for quantity. Subtracting the product from 1 hence yields the carrier detection probability for the mating type in question. It is worthy of note that, by design, formula 1 explicitly accounts for the possibility of more than one recessive disease affecting a single mating.
When formula 1 is applied to the 86 ACMG Tier 3 genes, the resulting couple carrier detection probabilities are 1.84% (AFR), 1.61% (ASJ), 0.63% (NFE), 0.32% (AMR), 0.28% (SAS) and 0.19% (EAS), respectively (see rightmost column of Table 1). Empirical estimates of the yield of an expanded carrier screening in diverse ethnic groups were derived before in a study by Haque et al. (2016) of nearly 350,000 reproductive-aged individuals, primarily from the USA. The respective samples were tested with the Family Prep Screen (Counsyl™ Inc., San Francisco) covering a large number of autosomal and X-linked recessive conditions. The resulting disease risks (see right-most column of Table 5 of the original publication) correspond well to approximately 1/4 of the couple carrier detection probabilities projected in the present study. This underpins the validity of our calculations and reflects the notable overlap between the 94 genes considered by Haque et al. (2016) and the 86 ACMG Tier 3 genes.
In his 2019 review on carrier screening, Antonarakis (2019) recalled that a 30-year-old Canadian survey (Baird et al. 1988) of > 1 million neonates still represents the most comprehensive assessment of the burden of autosomal recessive diseases in a population of European descent. The incidence there was estimated to equal 1.7 in 1000 newborns, which correspond to an underlying joint carrier probability of 4∙0.17 = 0.68%. Therefore, we may surmise that the ACMG Tier 3 gene account, not only for over 50%, but for over 90% (0.63/0.68 = 0.926) of the autosomal recessive genetic load of non-Finnish Europeans.
Carrier detection probabilities calculated for unrelated couples are not valid for cases of consanguineous mating, who represent an important target group of screening programs. However, formula 1 can be extended easily to consanguineous couples by including their coefficient of relatedness, r, so as to read
Applying formula 2 to the 86 ACMG Tier 3 genes yields couple carrier detection probabilities that range from between 0.87 (EAS) and 3.71% (ASJ), for 2nd-degree cousins, to between 5.53 (EAS) and 10.67% (ASJ), for uncle-aunt or niece-nephew matings (Table 1). Carrier detection probabilities are the highest for consanguineous couples of ASJ ethnicity because the choice of the ACMG Tier 3 genes was influenced by several particularly high carrier frequencies in Ashkenazi Jews. For example, for 11 of the 19 genes with a maximum carrier frequency > 1/50 (Table 1 in Gregg et al. 2021), the respective ASJ frequency was the highest of all ancestries (NFE: 3, AFR:2, EAS: 2, SAS: 1, AMR: 0).
Assuming that the proportion of the genetic load attributable to the ACMG Tier 3 genes is the same for first cousins as for unrelated couples in non-Finnish Europeans (92.6%, see above), the incidence of autosomal recessive diseases among the offspring of first cousins should equal 6.37/4/0.926 = 17.2 in 1000 newborns. At first glance, this tenfold increase, compared to non-consanguineous couples, appears to contradict the widely held view that the relative risk of birth defects among the offspring of first cousins equals two (Stoltenberg et al. 1997). However, the incidence of (life) birth defects in the EU is currently estimated as 20.4 in 1000 newborns (https://eu-rd-platform.jrc.ec.europa.eu/eurocat/eurocat-data/prevalence_en), implying that the vast majority of cases, namely 2.04–0.17 = 1.87%, must be due to causes other than homozygosity or compound heterozygosity for recessive genetic variants. Since this surplus can be assumed to be unaffected by consanguinity, it should complement the incidence of autosomal recessive diseases for any mating type, including first cousins. This implies that the relative risk of births defects for the latter type should amount to (1.87% + 1.72%)/2.04% = 1.76 in non-Finnish Europeans, a figure not too far away from the reference value of two.
Additional evidence for the authenticity of the carrier detection probabilities listed in Table 1 for consanguineous matings comes from a population-based study by Abouelhoda et al. (2016). Based upon whole exome and targeted panel DNA sequencing of > 7000 individuals, these authors concluded that at least 0.7% of children born to first-cousin parents in Saudi Arabia are affected by an autosomal recessive disease. Whilst gnomAD does not provide carrier frequencies specifically for Saudi Arabia, these may nevertheless be surmised to be not too different from gnomAD estimates for SAS. Under this assumption, the projected risk for an autosomal recessive disease of first cousin offspring in Saudi Arabia equals 3.73%/4 = 0.93%, a figure that fits well with the authors’ notion that their empirical estimate of 0.7% is likely to represent a lower limit to the true disease risk.
We hope that the above considerations will aid in the process of implementation of carrier screening programs and provide additional support to reproductive counselling and to obtaining informed consent.
References
Abouelhoda M, Sobahy T, El-Kalioby M, Patel N, Shamseldin H, Monies D, Al-Tassan N, Ramzan K, Imtiaz F, Shaheen R, Alkuraya FS (2016) Clinical genomics can facilitate countrywide estimation of autosomal recessive disease burden. Genet Med 18:1244–1249
Antonarakis SE (2019) Carrier screening for recessive Disorders. Nat Rev Genet 20:549–561
Baird PA, Anderson TW, Newcombe HB, Lowry RB (1988) Genetic-disorders in children and young-adults: a population study. Am J Hum Genet 42:677–693
Bell CJ, Dinwiddie DL, Miller NA, Hateley SL, Ganusova EE, Mudge J, Langley RJ, Zhang L, Lee CC, Schilkey FD, Sheth V, Woodward JE, Peckham HE, Schroth GP, Kim RW, Kingsmore SF (2011) Carrier testing for severe childhood recessive diseases by next-generation sequencing. Sci Transl Med 3: 65ra4.
Cao A, Sba L, Galanello R, Rosatelli MC (1997) Molecular diagnosis and carrier screening for beta thalassemia. JAMA 278:1272–1277
Castellani C, Macek M Jr, Cassiman JJ, Duff A, Massie J, ten Kate LP, Barton D, Cutting G, Dallapiccola B, Dequeker E, Girodon E, Grody W, Highsmith EW, Kääriäinen H, Kruip S, Morris M, Pignatti PF, Pypops U, Schwarz M, Soller M, Stuhrman M, Cuppens H (2010) Benchmarks for cystic fibrosis carrier screening: a European consensus document. J Cyst Fibros 9:165–178
Christianson A, Modell B (2004) Medical genetics in developing countries. Ann Rev Genomics Hum Genet 5:219–265
Cornel MC, Rigter T, Jansen ME, Henneman L (2021) Neonatal and carrier screening for rare diseases: how innovation challenges screening criteria worldwide. J Community Genet 12:257–265
Gregg AR, Aarabi M, Klugman S, Leach NT, Bashford MT, Goldwaser T, Chen E, Sparks TN, Reddi HV, Rajkovic A, Dungan JS (2021) ACMG Professional Practice and Guidelines Committee. Screening for autosomal recessive and X-linked conditions during pregnancy and preconception: a practice resource of the American College of Medical Genetics and Genomics (ACMG). Genet Med 23:1793–1806
Guo MH, Gregg AR (2019) Estimating yields of prenatal carrier screening and implications for design of expanded carrier screening panels. Genet Med 21:1940–1947
Haque IS, Lazarin GA, Kang HP, Evans EA, Goldberg JD, Wapner RJ (2016) Modeled fetal risk of genetic diseases identified by expanded carrier screening. JAMA 316:734–742
Henneman L, Borry P, Chokoshvili D, Cornel MC, van El CG, Forzano F, Hall A, Howard HC, Janssens S, Kayserili H, Lakeman P, Lucassen A, Metcalfe SA, Vidmar L, de Wert G, Dondorp WJ, Peterlin B (2016) Responsible implementation of expanded carrier screening. Eur J Hum Genet 24:e1–e12
Kaback M, Lim-Steele J, Dabholkar D, Brown D, Levy N, Zeiger K (1993) Tay-Sachs disease – carrier screening, prenatal diagnosis, and the molecular era. An international perspective, 1970 to 1993. Int TSD Data Collect Netw JAMA 270:2307–2315
Kirk EP, Barlow-Stewart K, Selvanathan A, Josephi-Taylor S, Rajagopalan S, Cowley MJ, Gayevskiy V, Bittles A, Burnett L, Elakis G, Lo W, Buckley M, Colley A, Roscioli T (2019) Beyond the panel: preconception screening in consanguineous couples using the TruSight One “clinical exome.” Genet Med 21:608–612
J Schmidtke M Krawczak Correspondence on “Screening for autosomal recessive and X-linked linked conditions during pregnancy and preconception: a practice resource of the American College of Medical Genetics and Genomics (ACMG)” by Gregg et al 2022 Genet Med 27 S1098
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
Both authors contributed to the conception and design of the study as well as to the material collection. Michael Krawczak performed the mathematical analyses. A first draft of the manuscript was written by Joerg Schmidtke. Both authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
Joerg Schmidtke is an employee of amedes MVZ wagnerstibbe. Michael Krawczak declares no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Schmidtke, J., Krawczak, M. Carrier detection probabilities for autosomal recessive variants in unrelated and consanguineous couples — an evaluation of the 86 genes of the ACMG ‘Tier 3’ panel. J Community Genet 13, 399–401 (2022). https://doi.org/10.1007/s12687-022-00593-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12687-022-00593-0