
Abstract
Objectives
The COVID-19 pandemic has caused high mortality rates worldwide, as well as consequent psychological and physical stress. The present study aimed to review the main existing scientific research studies conducted since the onset of the COVID-19 that have used mindfulness-based interventions (MBIs) as tools for emotional regulation, aiming to improve individuals’ ability to cope with general stress caused by pandemic periods and their consequences (e.g., contagion, confinement, loss of loved ones or job stability) especially related with anxiety, stress, depression, or emotional dysregulation.
Method
To this aim, six databases (i.e., PubMed, Medline, Embase, Scopus, Web of Science, and Science Direct) were consulted and analyzed following PRISMA-Sc guidelines.
Results
Of the 16 studies selected, 7 are clinical trials that used MBIs, and 9 are online surveys in which mindfulness and emotional regulation variables were assessed to explore their interrelations. Generally, the analysis suggested that the cultivation of MBI strategies for treating anxiety and depression during COVID-19 confinement periods resulted in improved psychological well-being.
Conclusions
MBI techniques can be considered useful intervention tools in current and future worldwide changing situations, in which personal development and resilience should be considered an urgent issue for both educational and preventive health practices. Conversely, there are also some limitations that arose from the field of MBI research that hopefully might be addressed in future research (such as the diversity of intervention techniques used across studies).
Pre registration
This study is not preregistered.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Avoid common mistakes on your manuscript.
The current COVID-19 (SARS-CoV-2) pandemic has caused high mortality rates worldwide and considerable concomitant psychological and physical stress (Ceban et al., 2022; Jungmann & Witthöft, 2020; Liu et al., 2020; Rosenbaum, 2020; Sohrabi et al., 2020; Tanne et al., 2020; Wang et al., 2021). In this context of increasing anxiety and situations requiring constant adaptation to unpredictable circumstances, the available emotional regulation tools that people have for coping with changing situations may be a key response to deal with adversity both in general populations and in at-risk groups (Liu et al., 2020; Yang et al., 2020). In this sense, a clear association has been reported between psychological well-being increases and the concomitant reduction in mental illness symptoms when specific therapeutic mindfulness tools can be mastered by participants (e.g., Chennapragada et al., 2022; Pappa et al., 2020).
The relationships between anxiety, depression, and other emotional symptoms have already been extensively documented in recently published scientific studies (e.g., Cao et al., 2020; Ceban et al., 2022; Huang & Zhao, 2020; Lai et al., 2020; Pappa et al., 2020; Qiu et al., 2020; Rosenbaum, 2020; Sohrabi et al., 2020; Xiao et al., 2020; Zhang & Ma, 2020). In this sense, comprehensive reviews emerged during the COVID-19 pandemic (e.g., such as the one by Nicola et al., 2020) that showed that the use of mindfulness-based interventions (MBIs), which can also serve as emotional self-management tools, might help people improve their coping abilities in situations such as contagion, confinement, loss of loved ones, and loss of job stability.
Mindfulness training results in a state of mind that can be characterized as intentional and non-judgmental or awareness of experience in the present moment (Baer et al., 2008; Kabat-Zinn, 2003, 2012). In general, it refers to a mental state at the present moment, including a constant observant monitoring of sensations, perceptions, and cognitions (Anālayo, 2020). The state of mind that emerges during any mindfulness-based practice can be contrasted with mental states in which the attentional focus is dissociated from the experience of the present moment, such as the constant mental shifting and jumping that occurs throughout fantasies and self-projections into the past or future, which often occur automatically and without full awareness of the actions or thoughts we are experiencing at any given time (Brown & Ryan, 2003).
A mindful state of mind can be cultivated through formal meditation and informal practice in everyday life. Mindfulness and the ability to enhance them through meditation seem to reflect the innate human capacity to deliberately pay mindful attention to the present moment and to learn from it (Hick & Bien, 2010). In recent years, structured mindfulness-based programs have emerged as possible approaches to address a range of clinical and subclinical difficulties, such as stress, chronic pain, anxiety, or recurrent depression (e.g., Brenton-Peters et al., 2021; Piet & Hougaard, 2011; Taylor et al., 2021). In addition, several neuroscientific studies have reported adaptive changes in brain function and structure (i.e., functional and neural plasticity) related to mindfulness training (e.g., Chen et al., 2022; Hölzel et al., 2011; Tang et al., 2012). With regard to the cultivation of mindfulness competence, it should be noted that attentional training skills play a central role in achieving mastery in meditation practices (e.g., Malinowski, 2013). As a consequence, a specific set of cognitive competencies has been identified as playing a crucial role in mindfulness-based practices (see Lutz et al., 2008): (a) skills of concentration and attention maintenance, (b) attention regulation skills for distraction inhibition and attentional control, (c) ability to detect distraction and consequently return to the previous point where the source of distraction intervened, and (d) re-engage with the meditation object. In fact, several behavioral and neural studies have shown how attentional processes improve after participants are exposed to meditation and mindfulness training and how this is also evidenced by their neural correlates (for reviews, see Cahn & Polich, 2006, 2009; Raffone & Srinivaran, 2010; Wong et al., 2022). It is worth noting that MBIs enhance focusing attention skills and awareness, which consequently contributes to strengthening self-regulation skills and helping individuals effectively cope with life challenges (e.g., González-García et al., 2016; Tang et al., 2015; Van Gordon et al., 2015; Zhao & Zhou, 2020). Additionally, recent scientific literature (e.g., Kuehner et al., 2023) strongly states that cognitive processing (i.e., mostly related to attention focusing; e.g., Mao et al., 2023) can be enhanced as a result of MBI training, and accordingly, it might help in health improvement (e.g., Dunn & Dimolareva, 2022) and emotional regulation (e.g., Ch et al., 2023).
During the COVID-19 global pandemic period, while citizens were confined to their homes and had little or no possibility of attending regular psychological or medical services, there was an urgent need to develop psychological treatments, and mental health measures were taken all over the globe (Luykx et al., 2020; Otu et al., 2020; Shigemura et al., 2020). For example, as reported in Wang et al. (2020), during the initial phase of the COVID-19 outbreak, respondents showed, in general terms, a psychological impact (i.e., higher levels of stress, anxiety, and depression). Pre-pandemic research (e.g., Tang et al., 2015) has shown how MBIs can be effective in reducing psychological symptoms of depression (Ma et al., 2019), anxiety (de Abreu Costa et al., 2019), or chronic disease (e.g., González-García et al., 2016). Given the emerging research on the significant impact of COVID-19 on mental health, there has been a substantial increase in the number of scientific publications that have been able to support MBIs for treating symptomatology derived from stress (e.g., Villalón et al., 2023), and mindfulness has been shown to be effective using self-reported and online treatments (e.g., González-García et al., 2021). Mindfulness implies attention training for gaining greater awareness (i.e., thoughts, emotions, bodily sensations, and behavior) and research carried out during the COVID-19 pandemic period (e.g., Dai et al., 2022) has shown the role of MBIs in physical symptoms caused by COVID-19 recovery, possibly as a consequence of mediating psychological variable improvement (i.e., related to anxiety reduction, stress, and possible symptoms of sadness and depression reduction) (Bhattacharya & Hofmann, 2023; Hao et al., 2020).
To this end, the present study aimed to review some existing research studies conducted since the onset of the COVID-19 pandemic. We reviewed scientific literature that have used mindfulness surveys or MBIs in relation to positive emotional regulation, and for coping with stress caused by pandemic periods and their consequences (e.g., contagion, confinement, hospitalization recovery, loss of loved ones, loss of job stability). Other interesting reviews have been released on similar matters (e.g., Brenton-Peters et al., 2021; Ceban et al., 2022; Chennapragada et al., 2022; Renaud-Charest et al., 2021; Taylor et al., 2021) but were not aimed at the same scope as the present study. This review specifically aimed to examine whether mindfulness can serve as a simple and powerful coping tool for anxiety, posttraumatic stress, or depression symptoms in health emergency periods. It is worth noting that our goal is coherent with a scoping review approach because we present a set of knowledge syntheses, based on a systematic approach, with the ultimate goal of identifying and synthesizing an emerging body of research on a specific topic that has not been summarized before. We believed that a detailed review of the research conducted since COVID-19 onset could give us a unique and relevant opportunity for analyzing the use of MBIs and mindfulness surveys for improving an individual’s mental health and well-being in social emergency conditions or any other infectious diseases.
Method
The methods and results were performed guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2009; Page et al., 2021; Tricco et al, 2018) for search and screening methods.
Search Strategy
A systematic search was performed in PubMed, Medline, Embase, Scopus, Web of Science, and Science Direct. In addition, a manual search was performed in Google Scholar to identify additional significant studies, and an alert was created to keep the search updated until the time of acceptance of the paper for publication (Table 1).
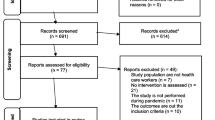
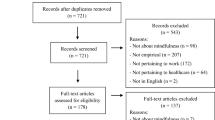
The following terms were used to perform the search procedure: (COVID-19 OR SARS-CoV-2 OR Severe Acute Respiratory Syndrome coronavirus); -AND- Mindfulness OR Self Compassion OR Mindfulness based OR Meditation OR MBIs; (2)-AND Emotional Regulation OR Depression OR Anxiety. Only research studies published from 2020 onwards on psychology and psychiatry research were selected. In Fig. 1, we showed the study assortment flowchart of the reporting documents chosen for the systematic reviews and meta-analyses we conducted.

Chosen reporting papers for Systematic Reviews and Meta-Analyses (PRISMA) study assortment flow diagram (we followed Xiao et al. (2020) flow chart structure)
We also used the PICO method (i.e., Population Intervention Comparison Outcome; Fineout-Overholt & Johnston, 2005) to perform additional, more detailed searches. PICO is a mnemonic method used to describe the key concepts of a research clinical question to be formulated prior to starting research for building a well-structured question. In the present study, we considered research articles with participants from adolescence onwards (i.e., adolescents, young adults, and adults), (P) those that participated in a mindfulness research study during the COVID-19 pandemic (i.e., not only MBIs but also mindfulness surveys), (I) studies that compared either MBIs (i.e., pre/post, using surveys to compare the effects of the intervention on emotional psychological variables such as emotional regulation, depression, and anxiety) or mindfulness surveys (i.e., when relating mindfulness questionnaires with affective variables such as emotional regulation, depression, and anxiety), and (C) studies with the aim of analyzing either the effectiveness of MBIs on an affective psychological variable improvement or their relations (i.e., mostly correlations or predictions) between mindfulness surveys (e.g., trait mindfulness) and affective psychological variables (O).
The database search following the PICO strategy was as follows: (a) search 1 (P): children OR adolescents OR young adults OR adults; (b) search 2 (I): Mindfulness Based Interventions -MBIs- OR Mindfulness Based Stress Reduction -MBSR- OR Compassion OR mindfulness surveys OR MINDFULNESS questionnaires, (c) search 3 (C) intervention OR pre/post OR control group OR significant differences OR statistical correlations OR statistical predictions; and (d) search 4 (O): effectiveness of an MBIs OR improvement of emotional regulation.
Study Selection and Eligibility Criteria
As shown in Fig. 1, in Step 4, the titles and abstracts of each publication were screened for relevance, and in Step 6, the full-text articles were accessed for eligibility after initial screening. As a result, studies were eligible for inclusion if they (1) followed a cross-sectional study design and (2) assessed the mental health status of the general population during the COVID-19 pandemic period related to emotional regulation (i.e., studies that focused on emotional regulation or stress, depression, anxiety, and other aspects that may be related to emotional regulation).
We excluded studies that (1) focused on particular subgroups of the population (e.g., specific clinical samples not related to depression or stress, health care workers, or school teachers); (2) were not peer-reviewed; (3) did not have full-text availability; or (4) were scientific work performed before the beginning of the COVID-19 worldwide pandemic.
Data Extraction
The data extraction table summarized the relevant data: (1) primary author and year of publication; (2) country/region of the population studied; (3) study design; (4) sample size; (5) mindfulness-based intervention used; (6) mindfulness assessment tools (if used); (7) other assessment questionnaires used; and (8) main results and conclusions. In Table 1, we show the results of the data extraction from the articles reviewed.
Results
In the present section, we described the characteristics and main results of the selected studies (i.e., synopsized in Table 1), and we presented them in two main subsections. In the first section, we appraised the studies that proposed MBIs online. In the second subsection, we summarized some of the selected studies in which participants were assessed on mindfulness variables by self-administered questionnaires (i.e., participants do not participate in MBIs), and the mindfulness measures were analyzed in relation to other variables of emotional dysregulation (e.g., anxiety in general, COVID-19 anxiety, stress, posttraumatic stress, depression, emotional intelligence, positive thoughts). The reviewed articles focused on observing the positive emotional regulation aspects that might be related to the cultivation of MBIs (i.e., subsection, effects of mindfulness interventions during the time of confinement) or with the variables or personality traits more often related to mindfulness (i.e., Subsection 2, descriptive studies that focused on the relations between mindfulness self-report measures and other emotional dysregulation measures) that were performed during confinement or post-COVID-19 hospitalization recovery. We additionally included a summary of the results at the end of this section.
Effects of Mindfulness Interventions During the Time of Confinement
Bäuerle et al. (2020a, 2020b) designed an online intervention that was self-administered and was able to be played by smartphone. The four intervention modules consisted of four 30 min modules conducted every other day for 2 weeks. Bäuerle et al. (2020c) carried out a clinical trial by assessing several questionnaires (Table 1) and applying learning mindfulness techniques (i.e., CoPE It Program CBT and Mindfulness). This study was limited by the lack of a control group. However, the results (i.e., difference between pre- and posttest) revealed clear benefits on stress and anxiety reduction.
Wei et al. (2020) also examined the efficacy of a mindfulness intervention but focused on adults with mild to moderate depression. Specifically, 26 adults were divided into two groups (i.e., intervention and support), and they showed an increased level of psychological stress caused by the COVID-19 pandemic. The MBIs were 2 weeks long and were focused on relaxation, self-care, and sense of safety. The results showed anxiety and depression reduction in the intervention group.
Zhang and Ma (2020) published two parallel studies that are worth mentioning. The first was conducted in Wuhan City (China) in February 2020. Recruitment was done through social networks, soliciting the participation of working adults who were experiencing confinement. A group of 110 participants (i.e., 60 participants in the mindfulness group and 50 in the mind-wandering condition-control group) received a daily short survey and instructions including audio for mindfulness practice. The second study was conducted on a sample of 140 UK adult workers who were recruited in two groups. In general terms, the results from both studies showed that mindfulness practice reduces the stressful effects of COVID-19, improving the quality and duration of sleeping in employees during confinement in the group that received MBIs in comparison to the control group.
Sturgill et al. (2021) evaluated the effectiveness of an MBI on 99 students (i.e., aged 19–29) who used the artificial intelligence conversational platform Ajivar (Sturgill et al., 2021) with a minimum frequency of twice a week. After using this platform, the participants in both the intervention and control groups were asked to complete a set of questionnaires (Table 1). The results indicated that the intervention group reported fewer symptoms of anxiety, stress, and depression than the control group, as well as a significant improvement in emotional intelligence skills. Additionally, O’Donnell et al. (2020) performed a randomized controlled trial comparing pre- and post-MBIs (i.e., after 30 days) in 150 adults (over 18 years old) who were asked to use a mindfulness app (i.e., Insight Timer Meditation App) and found reduced anxiety and well-being improvement.
Yuan (2021) evaluated adolescent students (i.e., aged from 12 to 14) who were asked to listen to 15-min MBI recordings (i.e., with a daily frequency for a 24-week period) with the aim of increasing their resilience and thereby decreasing their anxiety and stress symptoms. The mindfulness training effects were measured using resilience and emotional intelligence measures (Table 1) and were compared with the results in a control group. Participants from the intervention group showed a significant improvement in their emotional intelligence skills, an increase in positive thoughts, and a decrease in their associated stress symptoms.
In summary, the studies reviewed in this subsection (i.e., Bäuerle et al., 2020c; Sturgill et al., 2021; Wei et al., 2020; Yuan, 2021; Zhang & Ma, 2020) delivered online treatments during the confinement period and obtained benefits in terms of stress, depression, and anxiety reduction and improvements in the sleep quality and emotional intelligence skills of the participants.
Descriptive Studies That Focused on the Relations Between Mindfulness Self-report Measures and Other Emotional Dysregulation Measures
In this subsection, we summarized some of the selected studies in which participants did not participate in MBIs but were assessed on mindfulness variables by self-administered questionnaires.
Two descriptive studies, addressed in adolescent populations, analyzed relations between mindfulness measures and anxiety, stress, or depression measures. First, in Yu et al. (2020), emotional dysregulation was assessed in 332 students using the Depression, Anxiety, Meaningfulness of Life and Stress Scales (Table 1). They found significant correlations between resilience measures and the variables of self-esteem, life satisfaction, and personality trait factors. Hong et al. (2020) assessed the stress generated by media exposure during quarantine and emotional dysregulation in 439 adolescents who were studying in Wuhan, China. These students were asked to complete the Adolescent Mindfulness Measure, a rumination inventory, a psychological stress scale, and a social media questionnaire (Table 1). The results indicated that the higher the person’s mindfulness skills are, the greater the acceptance of the situation and the lower the manifestation of symptoms linked to emotional dysregulation. They also found that stress and anxiety increased as a consequence of media exposure, and it was also related to an increase in negative thoughts and ruminations.
Another study by Michel et al. (2020) focused on aspects that could affect people’s emotional dysregulation in times of social uncertainty and analyzed the role of mindfulness variables in reducing negative feelings related to self-perceived loneliness and sadness in 302 adults. Participants completed several online questionnaires (Table 1). The results showed that people with previous mindfulness training evidenced better adaptation skills to loneliness and therefore had less negative depression-related feelings.
In another recent study, Waterschoot et al. (2021) analyzed the negative effects of boredom resulting from this time of social isolation. Online interviews were collected from 1455 individuals over 18 years of age. These participants were asked to complete several questionnaires (Table 1). The results showed that people with a high level of mindfulness had less boredom and a higher degree of satisfaction with their lives, as well as being more mindful and exhibiting autonomy-oriented strategies.
Dubey et al. (2020) aimed to analyze the relationship between users’ levels of mindfulness and anxiety and assessed the degree of psychological flexibility shown during quarantine in India. For this purpose, 402 participants (i.e., aged between 18 and 64) completed a group of online questionnaires (i.e., depression, anxiety, stress, mindfulness facets; emotional regulation, acceptance, and COVID-19 knowledge; see Table 1). The results showed that increased emotional adjustment problems appeared more in participants with less psychological flexibility, but participants with greater COVID-19 awareness were more adaptive and showed less stress. In this sense, Difonte et al. (2020) performed a similar descriptive online study (i.e., 309 adults) and mentioned the benefits of mindfulness practice in reducing emotional regulation problems, particularly anxiety- and stress-related symptoms.
In a different recent study, Dai et al. (2022) aimed to identify the prevalence of common mental health problems among patients who recovered from COVID-19 and explore the potential mechanism through which MBIs could be valid tools for relieving depression and posttraumatic stress. They used several surveys and questionnaire assessments (Table 1) and found that mindfulness was negatively associated with depressive symptoms through the mediating effect of resilience and that anxiety-related symptoms were negatively associated with posttraumatic stress through the mediating effect of anxiety symptoms. They concluded that people who had recovered from COVID-19 showed symptoms related to psychological distress and that the cultivation of mindfulness practices implied relief from depressive symptoms and posttraumatic stress directly or indirectly, suggesting that mindfulness-based interventions could also improve mental participants’ well-being. Similarly, Belen (2021) explored the relationship between COVID-19 fear and aspects of mental health and analyzed whether mindfulness can act as a mediational variable. They found that mindfulness mediated the relationship between fear of COVID-19 and depression and anxiety.
In the same line of argumentation, Dillard and Meier (2021) used several surveys (i.e., assessed trait mindfulness scale, stress, anxiety, trait anxiety, and depression; see Table 1). The findings indicated that individuals who rated higher in trait mindfulness also reported less stress and anxiety while staying at home. Additionally, higher mastery of MBIs was associated with less worry about the virus. Additionally, trait mindfulness was negatively related to depression, and numerous associations between mindfulness and coping emerged (e.g., higher trait mindfulness was associated with healthier strategies in coping with coronavirus).
Additionally, Jiménez et al. (2020) compared the results of surveys completed by 412 participants from various provinces in Spain and analyzed the relationships between some emotional regulation variables and self-compassion (SC). They used several assessment measures (i.e., depression, anxiety, stress, and self-compassion; see Table 1). The results showed that the cultivation of SC improved participants’ quality of life and can also be considered a determinant factor for predicting lower levels of anxiety, depression, and stress. Regarding posttraumatic stress symptoms, the youth factor (i.e., found to be associated with mindfulness therapy practice) was linked to better insight and coping strategies.
Results Summary
In the first subsection, we observed that the studies reviewed (e.g., Bäuerleet al., 2020c; Zhang & Ma, 2020) delivered several online treatments during the confinement period. In this group of interventions, we detected that mindfulness scientists quickly tried to respond to the emergency situation (i.e., confinement and general difficulty in accessing health services) and provided citizens with MBI tools but adapted them to the unique needs of the pandemic and confinement, thus obtaining very promising results in psychological aspects that are key in the prevention of mental and physical diseases (i.e., benefits on stress, depression, and anxiety reduction; improving sleep quality and emotional intelligence skills). In the second results subsection, we summarized the selected studies in which mindfulness variables were assessed by self-administered questionnaires and related to emotional variables. In this sense, we observed that mindfulness mediated the relationship between fear of COVID-19 and depression and anxiety (e.g., Belen, 2021), improving mental health (i.e., stress, anxiety and depression, resilience; e.g., Hong et al., 2020; Difonte et al., 2020; Dubey et al., 2020; Dillard & Meier, 2021; O’Donnell et al., 2020; Zhang & Ma, 2020). They also found associations between trait mindfulness and mental health factors related to COVID-19 (e.g., O’Donnell et al., 2020); a high level of mindfulness traits was related to less boredom, a higher degree of life satisfaction, and more autonomy-oriented strategies (O’Donnell et al., 2020). They also obtained results that revealed increasing emotional adjustment difficulties in participants with a low level of psychological flexibility and found that participants with greater COVID-19 awareness were more adaptive and showed lower levels of stress and emotional dysregulation (Dubey et al., 2020; Hong et al., 2020; O’Donnell et al., 2020). Additionally, stress, anxiety, and negative thoughts increased as a consequence of COVID-19 media exposure (Hong et al., 2020). Additionally, self-compassion was related to better coexistence during confinement (Jiménez et al., 2020); previous mindfulness training was found to reduce emotional dysregulation caused by forced loneliness (Michel et al., 2020). Finally, participants who had recovered from COVID-19 showed that MBIs were important tools for coping with depressive symptoms and posttraumatic stress (Dai et al., 2022; Dillard & Meier, 2021), and mindfulness and life meaning might operate as important protective factors of mental health (Yu et al., 2020). Seen together, the studies that have focused on analyzing the existing relationships between variables of mindfulness (i.e., registered from self-administered questionnaires) in relation to variables of emotional regulation showed improvements in emotional regulation, the avoidance of consequent symptoms of anxiety, depression and stress, and posttraumatic stress, better resilience and adaptive capacity, greater ability to find autonomous and creative solutions to forced loneliness and isolation, and an improvement of participants’ well-being and life quality.
Discussion
In situations of great emotional stress, such as COVID-19 confinement, the use of MBIs (i.e., proprioceptive awareness of bodily sensations and observation of mental flow) can be a practical tool to help individuals cope with fear, anxiety, and depression (e.g., Roy et al., 2020; Spijkerman et al., 2016). The MBIs were useful and pertinent to the COVID crisis because of the potential benefits of meditative breathing for lung function and meditation for alleviating pain during illness. Additionally, MBIs can be general tools of self-management to address stress. Even before the COVID-19 pandemic, the benefits of MBIs on respiratory health had already been tested (e.g., Paudyal et al., 2018; Wu et al., 2018) based primarily on the fact that meditative movement of breathing may have the potential to improve lung function and physical activity in any patient with lung disease. In this sense, the inner nature of MBIs was very pertinent for this crisis. Another outstanding aspect of MBIs that were coherent with the COVID-19 global crisis is the fact that MBIs are self-management tools that can be useful for coping with concerns and constant ruminations that worry people affected by respiratory problems and those who fear being infected (e.g., Blanck et al., 2018). In this sense, mindfulness practice might be a useful emotional regulation instrument that can be self-administered and can intervene before the onset of fear or anxiety (e.g., mindfulness focused on breathing as part of whole body awareness; Anālayo, 2020). Additionally, benefits of MBIs for alleviating pain during illness in different populations were found (e.g., Hilton et al., 2017). For instance, Khoo et al. (2019) found that MBSR training can enhance physical functioning and reduce pain intensity and distress in patients with chronic pain.
It should be noted that due to the COVID-19 situation, most mindfulness studies used online tools, either for data collection or for the application MBIs. In this sense, the benefits on well-being derived from the use of online mindfulness applications have already been demonstrated in previous studies (e.g., Champion et al., 2018; Howells et al., 2014; Ly et al., 2014). The existence of mindfulness-based interventions, yoga, or other emotional regulation MBI programs distributed online has, in many cases, facilitated access to them in situations of confinement as a result of the isolation measures proposed by many governments around the world. Authors such as Liu et al. (2020) also noted an increase in the number of online psychological therapies due to the easy usage of new technologies and their consistency with pandemic limitations. In this vein, the meta-analysis performed by Andersson et al. (2014) showed that the effectiveness of online therapies was similar to that of face-to-face therapies.
In the present review, we described a group of online MBIs that were performed during confinement. In this sense, it is worth noting that there are some studies that reported the effects of direct interventions (i.e., those that have applied targeted therapy in a programmed way) and those that have used indirect interventions (i.e., using computer applications or listening to recordings). In particular, in the present study, a summary analysis of the results of the first subsection suggested that training in mindfulness techniques can clearly be a useful and accessible tool to mitigate the stressful effects of the pandemic situation (e.g., fear of contagion, economic uncertainty, or social isolation) both in the general population and in at-risk populations (e.g., Bäuerle et al., 2020c; Sturgill et al., 2021; Wei et al., 2020; Yuan, 2021; Zhang & Ma, 2020). We observed that the studies that used MBIs (i.e., Bäuerle et al., 2020c; Sturgill et al., 2021; Wei et al., 2020; Yuan, 2021; Zhang & Ma, 2020) delivered online treatments during the confinement period and obtained benefits in stress and anxiety reduction (i.e., Bäuerle et al., 2020c; Sturgill et al., 2021; Wei et al., 2020; Yuan, 2021), depression reduction (i.e., Sturgill et al., 2021; Wei et al., 2020), stress reduction specifically identified as COVID-19 consequences (i.e., Zhang & Ma, 2020), improvement in sleep quality (i.e., Zhang & Ma, 2020), improvement in emotional intelligence skills (i.e., Sturgill et al., 2021; Yuan, 2021), and positive thoughts (i.e., Yuan, 2021).
Due to quarantine periods, social interaction has been limited, and in many cases, the population has had to face a new isolation and loneliness situation, and a series of descriptive studies that are of interest emerged. They focused on analyzing possible relationships between mindfulness self-report measures and other emotional regulation measures, that is, measuring mindfulness traits and their mutual relationships. For it, in the present study, a group of studies were revised in the second subsection of the results. As a general conclusion, the authors found that those who think and act more mindfully and show more self-compassion are less stressed and anxious and can be less likely to develop depression symptoms. Specifically, more mindful participants showed (a) more acceptance of the COVID-19 situation and lower manifestation of symptoms linked to emotional dysregulation (e.g., Dai et al., 2022; Difonte et al., 2020; Dillard & Meier, 2021; Dubey et al., 2020; Hong et al., 2020; Michel et al., 2020); (b) fewer depressive and anxiety symptoms (through the mediating effect of resilience, Dai et al., 2022); (c) less boredom (Waterschoot et al., 2021); (d) more satisfaction with their lives (e.g., Waterschoot et al., 2021); (e) more autonomy-oriented strategies (e.g., Waterschoot et al., 2021); (f) more psychological flexibility (i.e., less rumination, self-punishment, or catastrophic thinking; e.g., Difonte et al., 2020; Dubey et al., 2020); and (g) less worry about the virus and anticipating less negative effects if one gets the virus (Dillard & Meier, 2021). In general, the revised studies showed that the pre-existence of mindful and self-compassion auto-administered strategies or related mindful personality traits might be truly positive during uncertain and changing situations and that people can overcome stressful periods with fewer negative psychological consequences and with more positive thoughts and resilience.
Some studies found that stress, fear, and anxiety tend to diminish resistance to infectious diseases (e.g., Jones & Drummond, 2022; McEwen, 2016). Therefore, the cultivation of MBI tools (i.e., based on the development of attentional capacities) can be a key instrument to strengthen the immune system in a self-managed way, including periods of isolation and confinement or post-hospitalization recovery (e.g., Conklin et al., 2019; Dillard & Meier, 2021; Kaliman, et al., 2014). The cultivation of MBI attentional techniques of any kind may strengthen participants’ set of tools to cope with any other changing, stressful, or baffling situation that requires great amounts of resilience and emotional self-regulation abilities, such as wars, economic falls, illnesses, or dealing with the loss of a loved one.
Limitations and Future Directions
Inferences regarding the multiple applications of MBIs in many aspects related to well-being improvement in actual societies (i.e., characterized by rapid and constant changes on multiple levels) are incredibly wide and can be anticipated to be productive (e.g., Chennapragada et al., 2022). However, there are also many limitations that arose from the mindfulness research field that hopefully might be fixed and addressed in future lines of research.
First, a limitation of the mindfulness research field is the wide scope of techniques that are available, not only regarding mindfulness relaxation and self-compassion intervention research lines but also the existence of a wide range or variations that includes yoga, tai-chi, or cognitive therapies at different degrees. In the area of self-administered mindfulness questionnaires, there is a similar situation, ranging from tools that assessed mindfulness traits to others that are more focused on phenomenological feelings of the present moments and could also be more centered on awareness as a state of mind, attention as a way of focusing cognitive resources, or self-esteem reassurance (i.e., more related to self-compassion cultivation). As observed in the results described (i.e., in the subsection on online MBIs and in the subsection on self-administered questionnaires), it is worth noting the role of appraisal instruments and the limitations also observed in the studies that were analyzed in the present work, which were used for measuring MBI effectiveness in relation to well-being improvement and psychological variables. The main challenge facing today’s mindfulness therapy research area is not only the great MBI approach diversity that makes it difficult to address one unique mindfulness construct operationalization (e.g., commented extensively in Goldberg et al., 2022) but also the existence of different ways to build the appraisal instruments used to measure it. It is worth noting that all the ranges covered by MBIs and self-assessment surveys are incredibly valid and useful for human integrative growth. It is also worth pointing out that mindfulness, being a young research discipline with incredible growth in recent decades, will ultimately lead to more accurate delimitation of its subareas of research. For instance, the two most commonly used MBIs are mindfulness-based stress reduction (MBSR) and mindfulness-based cognitive therapy (MBCT) (Alsubaie et al., 2017). Both promote mindfulness skills by generating awareness of bodily sensations as a way to regulate emotional reactivity, but there are many more that integrate interventions that are diametrically opposed, and all are called “mindfulness” but are focused on promoting other skills (e.g., such as self-compassion techniques or yoga). In this sense, a recent consensus of specialized researchers in this area highlighted important conceptual problems related to how the construction of the “full attention concept” has been defined and multiple methodological problems in its empirical appraisal (Van Dam et al., 2018). Additionally, in terms of validity, the situation is similar, and there are numerous limitations. Zhang et al. (2021) reviewed in detail the validity of the MBIs and concluded that the most frequent limitations found were (a) low quality in the study design, (b) small sample size, (c) poor provision of monitoring, and (d) inconsistent terminology and measurement tools. In this sense, the articles reviewed in this paper reflect the same difficulties and challenges that mainly come from the mindfulness research area. In this sense, we think that part of the limitations in the present research moment of the mindfulness area is the diversity of intervention techniques and questionnaires, which in a way are difficult sometimes to make comparable because they are like dissecting the psychological mindfulness phenomenon in different facets and sharp or rounded edges; all of them shining with different lights of importance to the exploration of human mind and body potential.
As has been explained extensively in the present work, much has been published about how COVID affected our perception and ways of coping with stress, depression, and anxiety in periods of uncertainty and confinement and how the MBIs proved to be a possible set of valid tools to face unknown and adverse situations such as those experienced globally during the COVID-19 pandemic (e.g., Boekhorst & Duijndam, 2023; Mueller et al., 2022). Recent literature has shown post-COVID-19 medical consequences, mainly related to other acquired infectious diseases (Kuodi et al., 2023); cardiac sequelae (Marimuthu et al., 2023); post-COVID cognitive dysfunction (Quan et al., 2023); and postacute COVID-19 syndrome, “long COVID,” and post-COVID-19 vaccination syndrome (Scholkmann & May, 2023). In contrast, little has been said about the consequences of post-COVID conditions (e.g., people who continued to be affected by COVID-19 and other viral infections) and how MBIs could also be used to address the postpandemic stage. In other words, although this group of post-COVID pathologies has been clearly defined by the literature (e.g., Rufai et al., 2023), little has yet been published about the possible transfer of findings and interventions performed during the COVID-19 period to the treatment or post-COVID pathologies (i.e., those that have been created as a result of the pandemic and are currently a new global health problem). Therefore, we believe that future lines of research should focus more on the improvement of psychological variables (i.e., depression, anxiety, and emotional regulation, which could be affected as a consequence of post-COVID pathologies) by transferring all the findings obtained in relation to all emerging MBI therapies during the COVID pandemic period. In this sense, all the MBI treatments that have proven effective during the COVID-19 period can be applied to these new groups of pathologies, but new research has to be done mostly because of the long-term duration that these new illnesses have, in contrast to COVID-19. For instance, a recent review publication (e.g., Liu et al., 2022) analyzed the effectiveness of online mindfulness-based interventions for improving mental health in patients with physical health conditions. In these publications, the authors interestingly analyzed articles on MBIs for illnesses such as human immunodeficiency virus and acquired immunodeficiency syndrome, and some of its findings around MBIs can be successfully transferred to post-COVID pathologies. Long-term pathologies present new challenges to patients mostly because of the frustration that emerges from the fact that recovery is not always that immediate, and in some cases, even the MBIs have to be more focused on the acceptance of an illness that can stay permanent and may not show any recovery in the future. For all these new challenges that post-COVID illnesses present, it is necessary to adjust what we already have known during the pandemic period to these new needs. For this reason, and above all the already mentioned limitations, we think that the incorporation of MBIs (i.e., addressing mindfulness-based coping strategies) has already shown its usefulness for overcoming uncertain and changeable situations such as those that occurred during the pandemic (i.e., those that provoked stress, anxiety, depression, and all types of emotional dysregulation symptoms). In the actual and future world, it is possible that these life-changing situations will continue to occur, and because of that, the development of resilience should be incorporated both in educational curricula and in preventive practices developed in workplaces and in all day life.
Data Availability
The manuscript does not contain clinical studies or patient data.
References
Alonso, J., Prieto, L., & Antó, J. M. (1995). La versión española del SF-36 Health Survey (Cuestionario de Salud SF-36): Un instrumento para la medida de los resultados clínicos [The Spanish version of the SF-36 Health Survey (the SF-36 health questionnaire): An instrument for measuring clinical results]. Medicina Clinica, 104(20), 771–776.
Alsubaie, M., Abbott, R., Dunn, B., Dickens, C., Keil, T. F., Henley, W., & Kuyken, W. (2017). Mechanisms of action in mindfulness-based cognitive therapy (MBCT) and mindfulness-based stress reduction (MBSR) in people with physical and/or psychological conditions: A systematic review. Clinical Psychology Review, 55, 74–91. https://doi.org/10.1016/j.cpr.2017.04.008
Anālayo, B. (2020). Somatics of early Buddhist mindfulness and how to face anxiety. Mindfulness, 11(6), 1520–1526. https://doi.org/10.1007/s12671-020-01382-x
Andersson, G., Cuijpers, P., Carlbring, P., Riper, H., & Hedman, E. (2014). Guided Internet-based vs. face-to-face cognitive behavior therapy for psychiatric and somatic disorders: A systematic review and meta-analysis. World Psychiatry, 13(3), 288–295. https://doi.org/10.1002/wps.20151
Andrews, G., & Slade, T. (2001). Interpreting scores on the Kessler Psychological Distress Scale (K10). Australian and New Zealand Journal of Public Health, 25(6), 494–497. https://doi.org/10.1111/j.1467-842x.2001.tb00310.x
Baer, R. A., Smith, G. T., Lykins, E., Button, D., Krietemeyer, J., Sauer, S., Walsh, E., Duggan, D., & Williams, J. M. (2008). Construct validity of the five facet mindfulness questionnaire in meditating and nonmeditating samples. Assessment, 15(3), 329–342. https://doi.org/10.1177/1073191107313003
Bäuerle, A., Graf, J., Jansen, C., Dörrie, N., Junne, F., Teufel, M., & Skoda, E. M. (2020a). An e-mental health intervention to support burdened people in times of the COVID-19 pandemic: CoPE It. Journal of Public Health, 42(3), 647–648. https://doi.org/10.1093/pubmed/fdaa058
Bäuerle, A., Graf, J., Jansen, C., Musche, V., Schweda, A., Hetkamp, M., Weismüller, B., Dörrie, N., Junne, F., Teufel, M., & Skoda, E. M. (2020b). E-mental health mindfulness-based and skills-based ‘CoPE It’ intervention to reduce psychological distress in times of COVID-19: Study protocol for a bicenter longitudinal study. British Medical Journal Open, 10(8), e039646. https://doi.org/10.1136/bmjopen-2020-039646
Bäuerle, A., Skoda, E., Dörrie, N., Böttcher, J., & Teufel, M. (2020c). Psychological support in times of COVID-19: The Essen community-based CoPE concept. Journal of Public Health, 42(3), 649–650. https://doi.org/10.1093/pubmed/fdaa053
Belen, H. (2021). Fear of COVID-19 and mental health: The role of mindfulness in during times of crisis. International Journal of Mental Health and Addiction, 20(1), 607–618. https://doi.org/10.1007/s11469-020-00470-2
Bhattacharya, S., & Hofmann, S. G. (2023). Mindfulness-based interventions for anxiety and depression. Clinics in Integrated Care, 16, 100138. https://doi.org/10.1016/j.intcar.2023.100138
Blanck, P., Perleth, S., Heidenreich, T., Kröger, P., Ditzen, B., Bents, H., & Mander, J. (2018). Effects of mindfulness exercises as stand-alone intervention on symptoms of anxiety and depression: Systematic review and meta-analysis. Behavior Research and Therapy, 102, 25–35. https://doi.org/10.1016/j.brat.2017.12.002
Boekhorst, M. G. B. M., & Duijndam, S. (2023). The association between facets of mindfulness and COVID-19 related distress: A cross-sectional study. Acta Psychologica, 233, 103826. https://doi.org/10.1016/j.actpsy.2023.103826
Bond, F. W., Hayes, S. C., Baer, R. A., Carpenter, K. M., Guenole, N., Orcutt, H. K., Waltz, T., & Zettle, R. D. (2011). Preliminary psychometric properties of the Acceptance and Action Questionnaire-II: A revised measure of psychological inflexibility and experiential avoidance. Behavior Therapy, 42(4), 676–688. https://doi.org/10.1016/j.beth.2011.03.007
Brenton-Peters, J., Consedine, N. S., Boggiss, A., Wallace-Boyd, K., Roy, R., & Serlachius, A. (2021). Self-compassion in weight management: A systematic review. Journal of Psychosomatic Research, 150, 110617. https://doi.org/10.1016/j.jpsychores.2021.110617
Brown, K., & Ryan, R. (2003). The benefits of being present: Mindfulness and its role in psychological well-being. Journal of Personality and Social Psychology, 84(4), 822–848. https://doi.org/10.1037/0022-3514.84.4.822
Cahn, B., & Polich, J. (2006). Meditation states and traits: EEG, ERP, and neuroimaging studies. Psychological Bulletin, 132(2), 180–211. https://doi.org/10.1037/0033-2909.132.2.180
Cahn, B., & Polich, J. (2009). Meditation (Vipassana) and the P3a event-related brain potential. International Journal of Psychophysiology, 72(1), 51–60. https://doi.org/10.1016/j.ijpsycho.2008.03.013
Cao, W., Fang, Z., Hou, G., Han, M., Xu, X., Dong, J., & Zheng, J. (2020). The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Research, 287, 112934. https://doi.org/10.1016/j.psychres.2020.112934
Ceban, F., Ling, S., Lui, L. M. W., Lee, Y., Gill, H., Teopiz, K. M., Rodrigues, N. B., Subramaniapillai, M., Di Vincenzo, J. D., Cao, B., Lin, K., Mansur, R. B., Ho, R. C., Rosenblat, J. D., Miskowiak, K. W., Vinberg, M., Maletic, V., & McIntyre, R. S. (2022). Fatigue and cognitive impairment in Post-COVID-19 Syndrome: A systematic review and meta-analysis. Brain, Behavior, and Immunity, 101, 93–135. https://doi.org/10.1016/j.bbi.2021.12.020
Ch, N. A. N., Ansah, A. A., Katrahmani, A., Burmeister, J., Kun, A. L., Mills, C., Shaer, O., & Lee, J. D. (2023). Virtual nature experiences and mindfulness practices while working from home during COVID-19: Effects on stress, focus, and creativity. International Journal of Human-Computer Studies, 171, 102982. https://doi.org/10.1016/j.ijhcs.2022.102982
Champion, L., Economides, M., & Chandler, C. (2018). The efficacy of a brief app-based mindfulness intervention on psychosocial outcomes in healthy adults: A pilot randomized controlled trial. PLoS ONE, 13(12), e0209482. https://doi.org/10.1371/journal.pone.0209482
Chan, H., Lo, L., Lin, M., & Thompson, N. (2016). Revalidation of the cognitive and affective mindfulness scale - revised (CAMS-R) with its newly developed chinese version (Ch-CAMS-R). Journal of Pacific Rim Psychology, 10, e1. https://doi.org/10.1017/prp.2015.4
Chen, P., Kirk, U., & Dikker, S. (2022). Trait mindful awareness predicts interbrain coupling but not individual brain responses during naturalistic face-to-face interactions. Frontiers in Psychology, 13, 915345. https://doi.org/10.3389/fpsyg.2022.915345
Chennapragada, L., Sullivan, S. R., Hamerling-Potts, K. K., Tran, H., Szeszko, J., Wrobleski, J., Mitchell, E. L., Walsh, S., & Goodman, M. (2022). International PRISMA scoping review to understand mental health interventions for depression in COVID-19 patients. Psychiatry Research, 316, 114748. https://doi.org/10.1016/j.psychres.2022.114748
Cohen, S., Kamarck, T., & Mermelstein, R. (1994). Perceived stress scale. Measuring Stress: A Guide for Health and Social Scientists, 10(2), 1–2. https://doi.org/10.2307/2136404
Conklin, Q., Crosswell, A., Saron, C., & Epel, E. (2019). Meditation, stress processes, and telomere biology. Current Opinion in Psychology, 28, 92–101. https://doi.org/10.1016/j.copsyc.2018.11.009
Dai, Z., Wang, H., Xiao, W., Huang, Y., Si, M., Fu, J., Chen, X., Jia, M., Leng, Z., Cui, D., Dong, L., Mak, W. W. S., & Su, X. (2022). The association of mindfulness and psychological well-being among individuals who have recovered from COVID-19 in Jianghan district, Wuhan, China: A cross-sectional study. Journal of Affective Disorders, 319, 437–445. https://doi.org/10.1016/j.jad.2022.09.062
Daza, P., Novy, D., Stanley, M., & Averill, P. (2002). The Depression Anxiety Stress Scale-21: Spanish translation and validation with a Hispanic sample. Journal of Psychopathology and Behavioral Assessment, 24, 195–205. https://doi.org/10.1023/A:1016014818163
de Abreu Costa, M., D’Alò de Oliveira, G. S., Tatton-Ramos, T., Gus Manfro, G., & Abrahão Salum, G. (2019). Anxiety and stress-related disorders and mindfulness-based interventions: A systematic review and multilevel meta-analysis and meta-regression of multiple outcomes. Mindfulness, 10(6), 996–1005. https://doi.org/10.1007/s12671-018-1058-1
De Jong Gierveld, J., & Van Tilburg, T. (2006). A 6-item scale for overall, emotional, and social loneliness: Confirmatory tests on survey data. Research on Aging, 28(5), 582–598. https://doi.org/10.1177/0164027506289723
Difonte, M., James, C., Michel, R., & Flannery-Schroeder, E. (2020). COVID-19 impact on anxiety and depression among emerging adults: The role of mindfulness. Journal of the American Academy of Child & Adolescent Psychiatry, 59(10), S252. https://doi.org/10.1016/j.jaac.2020.08.415
Dillard, A. J., & Meier, B. P. (2021). Trait mindfulness is negatively associated with distress related to COVID-19. Personality and Individual Differences, 179, 110955. https://doi.org/10.1016/j.paid.2021.110955
Dubey, N., Podder, P., & Pandey, D. (2020). Knowledge of COVID-19 and its influence on mindfulness, cognitive emotion regulation and psychological flexibility in the Indian community. Frontiers in Psychology, 11, 589365. https://doi.org/10.3389/fpsyg.2020.589365
Dunn, T. J., & Dimolareva, M. (2022). The effect of mindfulness-based interventions on immunity-related biomarkers: A comprehensive meta-analysis of randomized controlled trials. Clinical Psychology Review, 92, 102124. https://doi.org/10.1016/j.cpr.2022.102124
Fahlman, S. A., Mercer-Lynn, K. B., Flora, D. B., & Eastwood, J. D. (2013). Development and validation of the multidimensional state boredom scale. Assessment, 20(1), 68–85. https://doi.org/10.1177/1073191111421303
Fineout-Overholt, E., & Johnston, L. (2005). Teaching EBP: Asking searchable, answerable clinical questions. Worldviews on Evidence-Based Nursing, 2(3), 157–160. https://doi.org/10.1111/j.1741-6787.2005.00032.x
Fresco, D., Moore, M., Van Dulmen, M., Segal, Z., Ma, S., Teasdale, J., & Williams, J. (2007). Initial psychometric properties of the experience’s questionnaire: Validation of a self-report measure of decentering. Behavior Therapy, 38(3), 234–246. https://doi.org/10.1016/j.beth.2006.08.003
Gao, J., Zheng, P., Jia, Y., Chen, H., Mao, Y., Chen, S., Wang, Y., Fu, H., & Dai, J. (2020). Mental problems and social media exposure during COVID-19 outbreak. PLoS ONE, 15(4), e0231924. https://doi.org/10.1371/journal.pone.0231924
García-Campayo, J., Navarro-Gil, M., Andrés, E., Montero-Marin, J., López-Artal, L., & DeMarzo, M. (2014). Validation of the Spanish versions of the long (26 items) and short (12 items) forms of the Self-Compassion Scale (SCS). Health and Quality of Life Outcomes, 12, 4. https://doi.org/10.1186/1477-7525-12-4
Garnefski, N., & Kraaij, V. (2006). Relationships between cognitive emotion regulation strategies and depressive symptoms: A comparative study of five specific samples. Personality and Individual Differences, 40(8), 1659–1669. https://doi.org/10.1016/j.paid.2005.12.009
Goldberg, S. B., Riordan, K. M., Sun, S., & Davidson, R. J. (2022). The empirical status of mindfulness-based interventions: A systematic review of 44 meta-analyses of randomized controlled trials. Perspectives on Psychological Science, 17(1), 108–130. https://doi.org/10.1177/1745691620968771
González-García, M., Álvarez, J. C., Pérez, E. Z., Fernández-Carriba, S., & González, J. (2021). Feasibility of a brief online mindfulness and compassion-based intervention to promote mental health among university students during the COVID-19 pandemic. Mindfulness, 12(7), 1685–1695. https://doi.org/10.1007/s12671-021-01632-6
González-García, M., Borràs, X., López, J. G., & McNeil, K. G. (2016). Mindfulness-based cognitive therapy application for people living with chronic disease: The case of HIV. In S. Eisendrath (Ed.), Mindfulness-based cognitive therapy: Innovative applications (pp. 95–100). Springer. https://doi.org/10.1007/978-3-319-29866-5.
Hao, F., Tan, W., Jiang, L., Zhang, L., Zhao, X., Zou, Y., Hu, Y., Luo, X., Jiang, X., McIntyre, R. S., Tran, B., Sun, J., Zhang, Z., Ho, R., Ho, C., & Tam, W. (2020). Do psychiatric patients experience more psychiatric symptoms during COVID-19 pandemic and lockdown?. A case-control study with service and research implications for immunopsychiatry. Brain, Behavior, and Immunity, 87, 100–106. https://doi.org/10.1016/j.bbi.2020.04.069
Hilton, L., Hempel, S., Ewing, B. A., Apaydin, E., Xenakis, L., Newberry, S., Colaiaco, B., Maher, A. R., Shanman, R. M., Sorbero, M. E., & Maglione, M. A. (2017). Mindfulness meditation for chronic pain: Systematic review and meta-analysis. annals of behavioral medicine. A publication of the Society of Behavioral Medicine, 51(2), 199–213. https://doi.org/10.1007/s12160-016-9844-2
Hick, S., & Bien, T. (2010). Mindfulness and the therapeutic relationship. Guilford Press.
Hölzel, B., Lazar, S., Gard, T., Schuman-Olivier, Z., Vago, D., & Ott, U. (2011). How does mindfulness meditation work? Proposing mechanisms of action from a conceptual and neural perspective. Perspectives on Psychological Science, 6(6), 537–559. https://doi.org/10.1177/1745691611419671
Hong, W., Liu, R., Ding, Y., Fu, X., Zhen, R., & Sheng, X. (2020). Social media exposure and college students’ mental health during the outbreak of COVID-19: The mediating role of rumination and the moderating role of mindfulness. Cyberpsychology, Behavior, and Social Networking, 24(4), 282–287. https://doi.org/10.1089/cyber.2020.0387
Howells, A., Ivtzan, I., & Eiroa-Orosa, F. J. (2014). Putting the ‘app’ in happiness: A randomized controlled trial of a smartphone-based mindfulness intervention to enhance well-being. Journal of Happiness Studies, 17, 163–185. https://doi.org/10.1007/s10902-014-9589-1doi:10.1007/s10902-014-9589-1
Huang, Y., & Zhao, N. (2020). Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Research, 288, 112954. https://doi.org/10.1016/j.psychres.2020.112954
Jiménez, O., Sánchez-Sánchez, L., & Garciar-Montes, J. (2020). Psychological impact of COVID-19 confinement and its relationship with meditation. International Journal of Environment Research and Public Health, 17(8), 6642. https://doi.org/10.3390/ijerph17186642
Jones, P., & Drummond, P. (2022). Construction and evaluation of a mindfulness-based quality of life and well-being program (MQW) in a randomized trial. Current Psychology, 42(17), 14782–14803. https://doi.org/10.1007/s12144-021-02672-w
Jungmann, S., & Witthöft, M. (2020). Health anxiety, cyberchondria, and coping in the current COVID-19 pandemic: Which factors are related to coronavirus anxiety? Journal of Anxiety Disorders, 73, 102239. https://doi.org/10.1016/j.janxdis.2020.102239
Kabat-Zinn, J. (2003). Mindfulness-based interventions in context: Past, present, and future. Clinical Psychology: Science and Practice, 10(2), 144–156. https://doi.org/10.1093/clipsy.bpg016
Kabat-Zinn, J. (2012). Mindfulness for beginners: Reclaiming the present moment and your life. Boulder, CO, Sounds True.
Kaliman, P., Álvarez-López, M., Cosín-Tomás, M., Rosenkranz, M. A., Lutz, A., & Davidson, R. J. (2014). Rapid changes in histone deacetylases and inflammatory gene expression in expert meditators. Psychoneuroendocrinology, 40, 96–107. https://doi.org/10.1016/j.psyneuen.2013.11.004
Khoo, E. L., Small, R., Cheng, W., Hatchard, T., Glynn, B., Rice, D. B., Skidmore, B., Kenny, S., Hutton, B., & Poulin, P. A. (2019). Comparative evaluation of group-based mindfulness-based stress reduction and cognitive behavioural therapy for the treatment and management of chronic pain: A systematic review and network meta-analysis. Evidence-Based Mental Health, 22(1), 26–35. https://doi.org/10.1136/ebmental-2018-300062
Kroenke, K., Spitzer, R. L., & Williams, J. B. (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16, 606–613. https://doi.org/10.1046/j.1525-1497.2001.016009606.x
Kroenke, K., Strine, T., Spitzer, R., Williams, J., Berry, J., & Mokdad, A. (2009). The PHQ-8 as a measure of current depression in the general population. Journal of Affective Disorders, 114(1–3), 163–173. https://doi.org/10.1016/j.jad.2008.06.026
Kuehner, C., Schricker, I. F., Nayman, S., Reinhard, I., Zamoscik, V., Kirsch, P., & Huffziger, S. (2023). Effects of rumination and mindful self-focus inductions during daily life in patients with remitted depression: An experimental ambulatory assessment study. Behavior Therapy. https://doi.org/10.1016/j.beth.2023.04.002
Kuodi, P., Gorelik, Y., Gausi, B., Bernstine, T., & Edelstein, M. (2023). Characterization of post-COVID syndromes by symptom cluster and time period up to 12 months’ post-infection: A systematic review and meta-analysis. International Journal of Infectious Diseases, 134, 1–7. https://doi.org/10.1016/j.ijid.2023.05.003
Lai, J., Ma, S., Wang, Y., Cai, Z., Hu, J., Wei, N., Wu, J., Du, H., Chen, T., Li, R., Tan, H., Kang, L., Yao, L., Huang, M., Wang, H., Wang, G., Liu, Z., & Hu, S. (2020). Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Network Open, 3(3), e203976. https://doi.org/10.1001/jamanetworkopen.2020.3976
Levenstein, S., Prantera, C., Varvo, V., Scribano, M., Berto, E., Luzi, C., & Andreoli, A. (1993). Development of the Perceived Stress Questionnaire: A new tool for psychosomatic research. Journal of Psychosomatic Research, 37(1), 19–32. https://doi.org/10.1016/0022-3999(93)90120-5
Liu, J., Bao, Y., Huang, X., Shi, J., & Lu, L. (2020). Mental health considerations for children quarantined because of COVID-19. The Lancet Child & Adolescent Health, 4(5), 347–349. https://doi.org/10.1016/S2352-4642(20)30096-1
Liu, Z., Jia, Y., Li, M., Meng, X., Shang, B., Wang, C., & Chen, L. (2022). Effectiveness of online mindfulness-based interventions for improving mental health in patients with physical health conditions: Systematic review and meta-analysis. Archives of Psychiatric Nursing, 37, 52–60. https://doi.org/10.1016/j.apnu.2021.10.001
Liu, X. C., Liu, X., Chi, X., Zhang, J., Duan, W., & Wen, T. (2019). Validation of Child and Adolescent Mindfulness Measure (CAMM) in Chinese adolescents. Psychological Exploration, 3, 250–256. https://caod.oriprobe.com/articles/56719800/Validation_of_Child_and_Adolescent_Mindfulness_Mea.htm
Lovibond, S. H., & Lovibond, P. F. (1995a). Depression anxiety stress scales (DASS--21, DASS--42). https://doi.org/10.1037/t01004-000
Lovibond S. H. Lovibond P. F. & Psychology Foundation of Australia. (1995b). Manual for the depression anxiety stress scales (2nd ed.). Psychology Foundation of Australia.
Lutz, A., Slagter, H. A., Dunne, J. D., & Davidson, R. J. (2008). Attention regulation and monitoring in meditation. Review Cognitive Emotional Interactions, 12(4), 163–169. https://doi.org/10.1016/j.tics.2008.01.005
Luykx, J. J., Vinkers, C. H., & Tijdink, J. K. (2020). Psychiatry in times of the coronavirus disease 2019 (COVID-19) pandemic: An imperative for psychiatrists to act now. JAMA Psychiatry, 77(11), 1097–1098. https://doi.org/10.1001/jamapsychiatry.2020.1225
Ly, K. H., Trüschel, A., Jarl, L., Magnusson, S., Windahl, T., Johansson, R., Carlbring, P., & Andersson, G. (2014). Behavioral activation versus mindfulness-based guided self-help treatment administered through a smartphone application: A randomized controlled trial. British Medical Journal Open, 4, e003440. https://doi.org/10.1136/bmjopen-2013-003440
Ma, L., Zhang, Y., & Cui, Z. (2019). Mindfulness-Based interventions for prevention of depressive symptoms in university students: A meta-analytic review. Mindfulness, 10(11), 2209–2224. https://doi.org/10.1007/s12671-019-01192-w
Mak, W. W. S., Ng, I. S. W., Wong, C. C. Y., & Law, R. W. (2019). Resilience style questionnaire: Development and validation among college students and cardiac patients in Hong Kong. Assessment, 26(4), 706–725. https://doi.org/10.1177/1073191116683798
Malinowski, P. (2013). Neural mechanisms of attentional control in mindfulness meditation. Frontiers in Neuroscience, 7, 8. https://doi.org/10.3389/fnins.2013.00008
Mao, L., Wu, Y., Hong, X., Li, P., Yuan, X., & Hu, M. (2023). The influence of childhood maltreatment on trait depression in patients with major depressive disorder: A moderated mediation model of rumination and mindful attention awareness. Journal of Affective Disorders, 331, 130–138. https://doi.org/10.1016/j.jad.2023.03.052
Marimuthu, Y., Nair, G. C., Nagesh, U., Anand, A., Chopra, K. K., Nagappa, B., Sharma, N., Sivashankar, G., & Nagaraj, N. (2023). Prevalence of probable post-COVID cardiac sequelae and its health seeking behavior among health care workers: A cross-sectional analytical study. Indian Journal of Tuberculosis. https://doi.org/10.1016/j.ijtb.2023.06.008
McEwen, B. S. (2016). In pursuit of resilience: Stress, epigenetics, and brain plasticity. Annals of the New York Academy of Sciences, 1373(1), 56–64. https://doi.org/10.1111/nyas.13020
Michel, R., DiFonte, M., Ruiz, E., James, C., & Flannery-Schroeder, E. (2020). Mindfulness as a mediator in the relationship between social loneliness and depression in young adults during the COVID-19 pandemic. Journal of the American Academy of Child & Adolescent Psychiatry, 59(10), S253. https://doi.org/10.1016/j.jaac.2020.08.419
Moher, D., Liberati, A., Tetzlaff, J., & Altman, D. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Medicine, 6(7), e1000097. https://doi.org/10.1371/journal.pmed.1000097
Mueller, E. A., Suvanbenjakule, P., Lim, C. X., O’Brien, W. H., Chavanovanich, J., Jarukasemthawee, S., Pisitsungkagarn, K., & Suavansri, P. (2022). Coping with COVID-19: Survey data assessing psychological distress to COVID-19 and vaccine hesitancy with measures of theory of planned behavior, mindfulness, compassion, cultural orientation, and pandemic fatigue. Data in Brief, 43, 108390. https://doi.org/10.1016/j.dib.2022.108390
Nicola, M., Alsafi, Z., Sohrabi, C., Kerwan, A., Al-Jabir, A., Iosifidis, C., Agha, M., & Agha, R. (2020). The socioeconomic implications of the coronavirus pandemic (COVID-19): A review. International Journal of Surgery, 78, 185–193. https://doi.org/10.1016/j.ijsu.2020.04.018
O’Donnell, K. T., Dunbar, M., & Speelman, D. L. (2020). Effectiveness of using a meditation app in reducing anxiety and improving well-being during the COVID-19 pandemic: A structured summary of a study protocol for a randomized controlled trial. Trials, 21, 1006. https://doi.org/10.1186/s13063-020-04935-6
Otu, A., Charles, C. H., & Yaya, S. (2020). Mental health and psychosocial well-being during the COVID-19 pandemic: The invisible elephant in the room. International Journal of Mental Health Systems, 14(1), 1–5. https://doi.org/10.1186/s13033-020-00371-w
Owen, T. R. (1999). The reliability and validity of a wellness inventory. American Journal of Health Promotion, 13(3), 180–182. https://doi.org/10.4278/0890-1171-13.3.180
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., McDonald, S., McGuinness, L. A., … Alonso-Fernández, S. (2021). Declaración PRISMA 2020: una guía actualizada para la publicación de revisiones sistemáticas. 74(9), 790–799. https://doi.org/10.1016/j.recesp.2021.06.016
Panteleeva, Y., Ceschi, G., Glowinski, D., Courvoisier, D. (2017). Music for anxiety? Meta-analysis of anxiety reduction in nonclinical samples. Psychology of Music, 46(4), 473–487. https://doi.org/10.1177/0305735617712424
Pappa, S., Ntella, V., Giannakas, T., Giannakoulis, V. G., Papoutsi, E., & Katsaounou, P. (2020). Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain, Behavior and Immunity, 88, 901–907. https://doi.org/10.1016/j.bbi.2020.05.026
Paudyal, P., Jones, C., Grindey, C., Dawood, R., & Smith, H. (2018). Meditation for asthma: Systematic review and meta-analysis. Journal of Asthma, 55(7), 771–778. https://doi.org/10.1080/02770903.2017.1365887
Piet, J., & Hougaard, E. (2011). The effect of mindfulness-based cognitive therapy for prevention of relapse in recurrent major depressive disorder: A systematic review and meta-analysis. Clinical Psychology Review, 31(6), 1032–1040. https://doi.org/10.1016/j.cpr.2011.05.002
Qiu, J., Shen, B., Zhao, M., Wang, Z., Xie, B., & Xu, Y. (2020). A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. BMJ General Psychiatry, 33(2), e100213. https://doi.org/10.1136/gpsych-2020-100213
Quan, M., Wang, X., Gong, M., Wang, Q., Li, Y., & Jia, J. (2023). Post-COVID cognitive dysfunction: Current status and research recommendations for high risk population. The Lancet Regional Health - Western Pacific, 38, 100836. https://doi.org/10.1016/j.lanwpc.2023.100836
Raffone, A., & Srinivaran, N. (2010). The exploration of meditation in the neuroscience of attention and consciousness. Cognitive Processing, 11(1), 1–7. https://doi.org/10.1007/s10339-009-0354-z
Renaud-Charest, O., Lui, L. M. W., Eskander, S., Ceban, F., Ho, R., Di Vincenzo, J. D., Rosenblat, J. D., Lee, Y., Subramaniapillai, M., & McIntyre, R. S. (2021). Onset and frequency of depression in post-COVID-19 syndrome: A systematic review. Journal of Psychiatric Research, 144, 129–137. https://doi.org/10.1016/j.jpsychires.2021.09.054
Rosenbaum, L. (2020). Facing COVID-19 in Italy - Ethics, logistics, and therapeutics on the epidemic’s front line. The New England Journal of Medicine, 382(20), 1873–1875. https://doi.org/10.1056/NEJMp2005492
Roy, D., Tripathy, S., Kar, S., Sharma, N., Verma, S. K., & Kaushai, V. (2020). Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian Journal of Psychiatry, 51, 102083. https://doi.org/10.1016/j.ajp.2020.102083
Rufai, O. H., Chu, J., Sayibu, M., Shahani, R., Amosun, T. S., Lugu, B. K., Gonlepa, M. K., & Cherisol, M. P. (2023). Why should I vaccinate? The role of mindfulness and health-protective behaviors during the COVID-19 pandemic. Health Policy and Technology, 12(2), 100749. https://doi.org/10.1016/j.hlpt.2023.100749
Scholkmann, F., & May, C. A. (2023). COVID-19, post-acute COVID-19 syndrome (PACS, “long COVID”) and post-COVID-19 vaccination syndrome (PCVS, “post-COVID vac-syndrome”): Similarities and differences. Pathology - Research and Practice, 246, 154497. https://doi.org/10.1016/j.prp.2023.154497
Schwarzer, R., & Jerusalem, M. (1995). Generalized Self-Efficacy Scale (GSE). In J. Weinman, S. Wright, & M. Johnston, Measures in health psychology: A user’s portfolio. Causal and control beliefs (pp. 35–37). NFER-Nelson. https://doi.org/10.1037/t00393-000
Sharif, N., Kaur, H., Fomani, F. K., Rahmatpour, P., Kaveh, O., Pahlevan Sharif, S., Venugopal, A. V., & Hosseini, L. (2021). Psychometric properties of the impact of events scale-revised (IES-R) among the general Iranian population during the COVID-19 pandemic. Frontiers in Psychiatry, 12, 692498. https://doi.org/10.3389/fpsyt.2021.692498
Shi, J., & Wang, L. (2007). Validation of emotional intelligence scale in Chinese university students. Personality and Individual Differences, 43(2), 377–387. https://doi.org/10.1016/j.paid.2006.12.012
Shigemura, J., Ursano, R. J., Morganstein, J. C., Kurosawa, M., & Benedek, D. M. (2020). Public responses to the novel 2019 coronavirus (2019-nCoV) in Japan: Mental health consequences and target populations. Psychiatry and Clinical Neurosciences, 74(4), 281–282. https://doi.org/10.1111/pcn.12988
Sohrabi, C., Alsafi, Z., O’Neil, N., Khan, M., Kerwan, A., Al-Jabir, A., Iosifidis, C., & Agha, R. (2020). World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). International Journal of Surgery, 76, 71–76. https://doi.org/10.1016/j.ijsu.2020.02.034
Spijkerman, M. P., Pots, W. T., & Bohlmeijer, E. T. (2016). Effectiveness of online mindfulness-based interventions in improving mental health: A review and meta-analysis of randomized controlled trials. Clinical Psychology Review, 45, 102–114. https://doi.org/10.1016/j.cpr.2016.03.009
Spitzer, R. L., Kroenke, K., Williams, J. B., & Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: The GAD-7. JAMA Archives of Internal Medicine, 166(10), 1092–1097. https://doi.org/10.1001/archinte.166.10.1092
Sturgill, R., Martinasek, M., Schmidt, T., & Goyal, R. (2021). A novel artificial intelligence-powered emotional intelligence and mindfulness app (Ajivar) for the college student population during the COVID-19 pandemic: Quantitative questionnaire study. JMIR Formative Research, 5(1), e25372. https://doi.org/10.2196/25372
Tang, Y. Y., Lu, Q., Fan, M., Yang, Y., & Posner, M. (2012). Mechanisms of white matter changes induced by meditation. Proceedings of the National Academy of Sciences of the United States of America, 109(26), 10570–10574. https://doi.org/10.1073/pnas.1207817109
Tang, Y. Y., Hölzel, B. K., & Posner, M. I. (2015). The neuroscience of mindfulness meditation. Nature Reviews. Neuroscience, 16(4), 213–225. https://doi.org/10.1038/nrn3916
Tanne, J., Hayasaki, E., Zastrow, M., Pulla, P., Smith, P., & Garcia-Rada, A. (2020). Covid-19: How doctors and healthcare systems are tackling coronavirus worldwide. The British Medical Journal, 368, m1090. https://doi.org/10.1136/bmj.m1090
Taylor, H., Strauss, C., & Cavanagh, K. (2021). Can a little bit of mindfulness do you good? A systematic review and meta-analyses of unguided mindfulness-based self-help interventions. Clinical Psychology Review, 89, 102078. https://doi.org/10.1016/j.cpr.2021.102078
The EuroQol Group. (1990). EuroQol - A new facility for the measurement of health-related quality of life. Health Policy, 16(3), 199–208. https://doi.org/10.1016/0168-8510(90)90421-9
Topp, C. W., Østergaard, S. D., Søndergaard, S., & Bech, P. (2015). The WHO-5 Well-Being Index: A systematic review of the literature. Psychotherapy and Psychosomatics, 84(3), 167–176. https://doi.org/10.1159/000376585
Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K. K., Colquhoun, H., Levac, D., Moher, D., Peters, M. D. J., Horsley, T., Weeks, L., Hempel, S., Akl, E. A., Chang, C., McGowan, J., Stewart, L., Hartling, L., Aldcroft, A., Wilson, M. G., Garritty, C., … Straus, S. E. (2018). PRISMA Extension for Scoping Reviews (PRISMAScR): Checklist and explanation. Annals of Internal Medicine, 169(7), 467–473. https://doi.org/10.7326/M18-0850
Van Dam, N. T., Van Vugt, M. K., Vago, D. R., Schmalzl, L., Saron, C. D., Olendzki, A., Meissner, T., Lazar, S. W., Kerr, C. E., Gorchov, J., Fox, K. C. R., Field, B. A., Britton, W. B., Brefczynski-Lewis, J. A., & Meyer, D. E. (2018). Mind the hype: A critical evaluation and prescriptive agenda for research on mindfulness and meditation. Perspectives on Psychological Science, 13(1), 36–61. https://doi.org/10.1177/1745691617709589
Van Gordon, W., Shonin, E., & Griffiths, M. D. (2015). Toward a second-generation of mindfulness-based interventions. The Australian and New Zealand Journal of Psychiatry, 49(7), 591–592. https://doi.org/10.1177/0004867415577437
Villalón, F. J., Moreno, M. I., Rivera, R. Venegas, W., Arancibia, J. V., Soto, A., & Pemjean, A. (2023) Brief online mindfulness- and compassion-based inter-care program for students during COVID-19 pandemic: A randomized controlled trial. Mindfulness, 14(8), 1918–1929. https://doi.org/10.1007/s12671-023-02159-8
Wang, M., & Dai, X. Y. (2008). Chinese meaning in life questionnaire revised in college students and its reliability and validity test. Chinese Journal of Clinical Psychology, 16(5), 459–461.
Wang, C., Pan, R., Wan, X., Tan, Y., Xu, L., Ho, C. S., & Ho, R. C. (2020). Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. International Journal of Environmental Research and Public Health, 17(5), 1729. https://doi.org/10.3390/ijerph17051729
Wang, L., Li, D., Pan, S., Zhai, J., Xia, W., Sun, C., & Zou, M. (2021). The relationship between 2019-nCoV and psychological distress among parents of children with autism spectrum disorder. Globalization and Health, 17(1), 23. https://doi.org/10.1186/s12992-021-00674-8
Waterschoot, J., Van der Kaap-Deeder, J., Morbée, S., Soennens, B., & Vansteenkiste, M. (2021). “How to unlock myself from boredom?” The role of mindfulness and a dual awareness- and action-oriented pathway during the COVID-19 lockdown. Personality and Individual Differences, 175, 110729. https://doi.org/10.1016/j.paid.2021.110729
Wei, N., Huang, B. C., Lu, S. J., Hu, J. B., Zhou, X. Y., Hu, C. C., Chen, J. K., Huang, J. W., Li, S. G., Wang, Z., Wang, D. D., Xu, Y., & Hu, S. H. (2020). Efficacy of internet-based integrated intervention on depression and anxiety symptoms in patients with COVID-19. Journal of Zhejiang University. Science. b., 21(5), 400–404. https://doi.org/10.1631/jzus.B2010013
Wong, G., Sun, R., Adler, J., Yeung, K. W., Yu, S., & Gao, J. (2022). Loving-kindness meditation (LKM) modulates brain-heart connection: An EEG case study. Frontiers in Human Neuroscience, 16, 891377. https://doi.org/10.3389/fnhum.2022.891377
Wu, L. L., Lin, Z. K., Weng, H. D., Qi, Q. F., Lu, J., & Liu, K. X. (2018). Effectiveness of meditative movement on COPD: A systematic review and meta-analysis. International Journal of Chronic Obstructive Pulmonary Disease, 13, 1239–1250. https://doi.org/10.2147/COPD.S159042
Xiao, H., Zhang, Y., Kong, D., Li, S., & Yang, N. (2020). The effects of social support on sleep quality of medical staff treating patients with coronavirus disease 2019 (COVID-19) in January and February 2020 in China. Medical Science Monitor, 26, e923549. https://doi.org/10.12659/MSM.923549
Yang, J., Zheng, Y., Gou, X., Pu, K., Chen, Z., Guo, Q., Ji, R., Wang, H., Wang, Y., & Zhou, Y. (2020). Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: A systematic review and meta-analysis. International Journal of Infectious Diseases, 94, 91–95. https://doi.org/10.1016/j.ijid.2020.03.017
Yu, X., & Zhang, J. (2007). Factor analysis and psychometric evaluation of the Connor Davidson Resilience Scale (CD-RISC) with Chinese people. Social Behavior and Personality, 35(1), 19–30. https://doi.org/10.2224/sbp.2007.35.1.19
Yu, J., Yu, J., & Li, B. (2020). Effects of mindfulness and meaning in life on psychological distress in Chinese university students during the COVID-19 epidemic: A chained mediation model. Asian Journal of Psychiatry, 53, 102211. https://doi.org/10.1016/j.ajp.2020.102211
Yuan, Y. (2021). Mindfulness training on the resilience of adolescents under the COVID-19 epidemic: A latent growth curve analysis. Personality and Individual Differences, 172, 110560. https://doi.org/10.1016/j.paid.2020.110560
Zhang, Y., & Ma, Z. F. (2020). Impact of the COVID-19 pandemic on mental health and quality of life among local residents in Liaoning Province, China: A cross-sectional study. International Journal of Environmental Research and Public Health, 17(7), 2381. https://doi.org/10.3390/ijerph17072381
Zhang, D., Lee, E. K., Mak, E. C., Ho, C. Y., & Wong, S. Y. (2021). Mindfulness-based interventions: An overall review. British Medical Bulletin, 138(1), 41–57. https://doi.org/10.1093/bmb/ldab005
Zhao, N., & Zhou, G. (2020). Social media use and mental health during the COVID-19 pandemic: Moderator role of disaster stressor and mediator role of negative affect. Applied Psychology: Health and Well-Being, 12(4), 1019–1038. https://doi.org/10.1111/aphw.12226
Zheng, M. X., Masters-Waage, T. C., Yao, J., Lu, Y., Tan, N., & Narayanan, J. (2020). Stay mindful and carry on: Mindfulness neutralizes COVID-19 Stressors on work engagement via sleep duration. Frontiers in psychology, 11, 610156. https://doi.org/10.3389/fpsyg.2020.610156
Zhou, X., & Wu, X. (2016). The relationship between rumination, posttraumatic stress disorder, and posttraumatic growth among Chinese adolescents after earthquake: A longitudinal study. Journal of Affective Disorders, 193, 242–248. https://doi.org/10.1016/j.jad.2015.12.076
Funding
Open Access funding provided thanks to the CRUE-CSIC agreement with Springer Nature.
Author information
Authors and Affiliations
Contributions
M. F. L.-R.: conceptualization, methodology, writing-reviewing and editing, English editing, original draft preparation, supervision. V. M.-C.: data curation, writing-original draft preparation. Y. A.-E.: data curation, writing-original draft preparation. E. N.-P.: writing-reviewing and editing. F. A.-M.: writing-reviewing and editing.
Corresponding author
Ethics declarations
Use of Artificial Intelligence
Artificial intelligence (AI) was used for editing the manuscript to improve English grammar only at the last stage of the review process.
Ethics Approval
The University of Valencia provided IRB approval for the study.
Consent to Participate
Informed consent was not required because the manuscript does not contain clinical studies or patient data.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
López-Ramón, M.F., Moreno-Campos, V., Alonso-Esteban, Y. et al. Mindfulness Interventions and Surveys as Tools for Positive Emotional Regulation During COVID-19: A Scoping Review. Mindfulness 14, 2583–2601 (2023). https://doi.org/10.1007/s12671-023-02234-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12671-023-02234-0