
Abstract
Objectives
College is an exhilarating but stressful time often associated with mental distress. The StudiCare project offers Internet- and mobile-based interventions (IMI) for college student mental health promotion. Within this framework, we evaluated the IMI StudiCare Mindfulness, and examined potential moderators and mediators of effectiveness.
Methods
In this randomized controlled trial, 150 college students with low to moderate mindfulness were randomly assigned to StudiCare Mindfulness or a waitlist control group (WL). StudiCare Mindfulness comprises 5 weekly online modules based on Acceptance Commitment Therapy and stress management. Assessments took place before (t0) and 6 weeks after (t1) randomization. Primary outcome was mindfulness. Secondary outcomes were stress, depression, anxiety, quality of life, intervention satisfaction, and adherence. Sociodemographic variables, pre-intervention symptomatology, personality traits, and attitudes towards IMI were examined as potential moderators.
Results
Intention-to-treat analyses (N = 149) showed a large effect of StudiCare Mindfulness on mindfulness (d = 1.37; 95% CI: 1.01–1.73) compared to WL at t1 (β = 1.18; 95% CI: 0.96–1.40). Effects on secondary outcomes were significant in favor of the intervention group except for physical quality of life. Mindfulness was found to mediate intervention effectiveness on depression, anxiety, and stress. Moderation analysis was non-significant except for baseline openness to experience, with lower openness associated with larger intervention effects on mindfulness.
Conclusions
This trial suggests that StudiCare Mindfulness may enhance mindfulness and reduce mental health problems. Its potential applicability as low-threshold prevention and treatment option on a population level should be subject to future trials.
Trial Registration
German Clinical Studies Trial Register TRN: DRKS00012559.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Mental health problems and disorders are frequent in college students (American College Health Association, 2020; Auerbach et al., 2018) and can be associated with a higher risk for college dropout and lower academic functioning (Bruffaerts et al., 2018). However, most college students who suffer from mental health problems do not receive professional help (Bruffaerts et al., 2019; Mortier et al., 2018). Preference for self-management, stigma, and embarrassment are significant barriers for help-seeking (Ebert, Mortier, et al., 2019a, 2019b). Self-help Internet- and mobile-based interventions (IMI) might be a promising way to reach these students, as college students already widely use the Internet for health purposes (Pedrelli et al., 2015). Evidence suggests the effectiveness, acceptability, and suitability of IMI targeting mental health for this population (Harrer et al., 2019; Stallman & Kavanagh, 2018). Besides anonymity, IMI offer further advantages such as flexibility in time and place (Ebert et al., 2017), and potential scalability and cost-effectiveness (Donker et al., 2015). Additionally, therapeutically guided IMI have shown to be equally effective to face-to-face treatments for various somatic and mental health problems (Carlbring et al., 2018).
Mental health IMI are typically based on cognitive behavioral therapy (CBT), aiming to reduce disorders, disability, or distress. However, there is growing evidence for IMI based on mindfulness approaches and acceptance and commitment therapy (ACT) (Ebert et al., 2018). These interventions emphasize personal growth and resilience instead of removal of symptoms or disorders (Shapiro et al., 2016). To summarize the basic idea of mindfulness, learning to observe thoughts, bodily sensations, and emotions as moment-to-moment experiences in an open and accepting manner can foster resilience to stress (Kabat-Zinn, 2003). ACT integrates mindfulness with CBT and adds a focus on committed action towards one’s values and goals (S. C. Hayes, 2004). A recent systematic review (Howell & Passmore, 2019) conceptualized ACT as a positive psychological intervention viable not only for treating mental disorders but also for promoting mental health and calls out for more research on ACT’s effect on positive mental health indicators. Research like this is in line with the WHO’s updated definition of mental health as more than just the absence of illness (World Health Organization, 2001) and mental health promotion as a key objective of the WHO Mental Health Action Plan 2013–2020 (World Health Organization, 2013).
A meta-analysis of 15 randomized controlled trials (RCTs) examined the effectiveness of mindfulness-based IMI across clinical and healthy adult populations (i.e., college students, employees) (Spijkerman et al., 2016). Different approaches were included, such as mindfulness-based stress reduction (MBSR; Kabat-Zinn, 1982), mindfulness-based cognitive therapy (MBCT) (Segal et al., 2001), and ACT (S. C. Hayes, 2004). Mindfulness-based IMI reduced stress most effectively (g = 0.51, 95% CI: 0.26–0.75), resulted in small to medium effects for depression (g = 0.29, 95% CI: 0.13–0.46) and anxiety (g = 0.22, 95% CI: 0.05–0.39) and also improved mindfulness (g = 0.32, 95% CI: 0.23–0.42). Similar results were found in another meta-analysis on preventive mindfulness-based IMI (Jayewardene et al., 2017) and a meta-analysis examining ACT-based IMI in clinical and healthy samples (Brown et al., 2016). However, only few studies focused on the effect of ACT-based interventions on positive mental health indicators (e.g., mindfulness) in college students, both face-to-face and IMI, and there is a need for more adequately powered RCTs (Howell & Passmore, 2019).
Mindfulness has also been suggested as a mechanism of change in psychological interventions (Walach et al., 2006). In their meta-analysis, Gu et al. (2015) found the mediating role of mindfulness to be well-established for depression, whereas it could only be examined in two studies each for stress and anxiety. In their subsequent study, the same researchers found mindfulness to significantly mediate reductions in stress in a mindfulness IMI (Gu et al., 2018). Similarly, Pots et al. (2016) found facets of mindfulness to mediate reductions in depression in an ACT-based IMI, whereas Viskovich and Pakenham (2018) could not confirm mindfulness to mediate changes in depression, anxiety, or stress. The limited number of studies and inconclusive findings warrant further examination of the mediating role of mindfulness on mental health outcomes in the IMI setting.
Intervention research should also address under what conditions psychological interventions are effective, e.g., to optimize target groups (Kraemer et al., 2002). For mindfulness- and ACT-based interventions, this question has mainly been studied in the face-to-face setting (Pots et al., 2016) and for negative mental health indicators (e.g., depression, anxiety). Sociodemographic variables (e.g., sex, age) were not confirmed as moderators of intervention effectiveness (Kuyken et al., 2016). For pre-intervention mindfulness, there is mixed evidence (Nyklíček et al., 2016; Shapiro et al., 2011). Baseline depressive and anxiety symptoms were found to be significant moderators (Kuyken et al., 2016; Pots et al., 2016). Finally, there is also evidence that personality traits (e.g., neuroticism, extraversion) moderate the effectiveness of such interventions (de Vibe et al., 2015; Nyklíček & Irrmischer, 2017). In conclusion, existing evidence points to several potential moderators of effectiveness of mindfulness and ACT-based interventions but is inconclusive and particularly thin in the field of IMIs.
Based on the literature presented above, the present study aimed to examine the effectiveness, acceptability, and mechanisms of change of the newly developed mindfulness- and ACT-based IMI StudiCare Mindfulness in a German-speaking college student population. It was hypothesized that participants who received the IMI would have significantly better outcomes then the waitlist control group 6 weeks after randomization on both the primary outcome mindfulness and the secondary outcomes depressive symptoms, anxiety symptoms, stress, and quality of life. Mindfulness was examined as a potential mediator of effectiveness on the secondary outcomes depressive symptoms, anxiety symptoms, and stress, and various baseline characteristics were examined as potential moderators of effectiveness on the primary outcome mindfulness.
Methods
Participants
College students were recruited via circular emails sent out by colleges across Germany, Switzerland, and Austria. Additionally, recruitment was conducted via flyers and posters, social media, student unions, and student counseling. Students were informed about StudiCare and given a link to the StudiCare homepage (www.studicare.com). The homepage provided detailed information on StudiCare Mindfulness and study participation, as well as the possibility to sign up. Participants had to (a) be at least 18 years, (b) be currently enrolled in college, (c) have a moderate to low level of mindfulness according to a cut-off of < 37 on the Freiburg Mindfulness Inventory (FMI; cutoff was chosen as it represents the medium FMI value in the general population (Walach et al., 2006)), (d) are not currently undergoing psychotherapy, (e) are not currently enrolled in another mindfulness training, (f) have sufficient knowledge of the German language (measured by the capability to proceed through enrollment and screening process), (g) have Internet access, and (h) provide written informed consent.
Using G*Power 3.1.9.2 (Faul et al., 2007), the sample size was estimated a priori for the expected effectiveness of StudiCare Mindfulness compared to WL on the primary outcome mindfulness at post-intervention (t1). In a meta-analysis of Internet-based mindfulness interventions, an effect size of g = 0.3 was found (Spijkerman et al., 2016). To detect an effect of this size, the sample size was calculated to be n = 60 subjects per group, with power set at 1-ß = 0.9 and α = 0.05. In total, 25% of the sample size was added to account for expected dropout (Spijkerman et al., 2016), resulting in a total of N = 150.
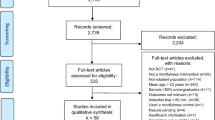
The study flow is illustrated in Fig. 1. Between May and September 2017, 415 persons registered for the study via the StudiCare homepage (see study flow, Fig. 1). Subsequently, 276 of them participated in the eligibility screening, and 150 ultimately enrolled in the study. There were various reasons for exclusion (FMI > 37, n = 25; no informed consent, n = 89; no baseline data, n = 2; withdrawal of consent; n = 1). Twelve participants in the IG (attrition rate: 16%) and 3 participants in the WL (attrition rate: 4%) did not participate in the post-assessment (t1).

Participant flow
Baseline characteristics were comparably distributed in both study arms, as can be obtained from Table 1 and Table 2. Participants had a mean age of 28 years (SD = 8.3), and the majority of them were female (81%), single (58%), and of German citizenship (83%). They mainly were full-time students (71%), had absolved an average of 10 semesters at college (SD = 5.3), and almost one-third of them studied psychology (28%). Concerning previous treatment, nearly one-quarter of participants had psychotherapy experience (23%). Participants’ general attitude towards Internet- and mobile-based interventions (IMI) and their confidence in the effectiveness of IMI were moderate to high, whereas their perception of risks, technologization threats, and anonymity benefits were moderate.
Procedure
In this two-armed randomized controlled trial of parallel-group design, we compared the effectiveness of the newly developed guided Internet-based intervention StudiCare Mindfulness (intervention group, IG) to a waitlist control group (WL) (see Fig. 1 for flowchart). Both study groups had unrestricted access to usual treatment options (TAU). The StudiCare Project (https://www.studicare.com/) was funded by the health insurance company BARMER and has set itself the task of examining and promoting college students’ mental health (Ebert et al., 2019a; Kählke et al., 2019). It is embedded in the “World Mental Health International College Student Initiative” (WMH-ICS) (https://www.hcp.med.harvard.edu/wmh/college_student_survey.php) and provides a wide selection of Internet- and mobile-based interventions (IMI) (e.g., procrastination, test anxiety, physical activity, depression, substance abuse) to students from German, Swiss, and Austrian colleges and universities while simultaneously evaluating them (Harrer et al., 2018; Kählke et al., 2019). This RCT was conducted and reported according to the CONSORT 2010 statement (Schulz et al., 2010). It was registered a priori at the WHO International Clinical Trials Registry Platform via the German Clinical Studies Trial Register (TRN: DRKS00012559; registration date: 06/29/2017). Additionally, details of study design were described in a study protocol published on OSF (Open Science Framework; https://osf.io/5msn6/).
Participants were screened for eligibility via the online survey platform “Unipark” (www.unipark.com). After providing written informed consent, they completed baseline assessment (t0). They were then randomly allocated to one of the two study groups (IG, WL) by an independent researcher not otherwise involved in the study using an online-based, automated randomization program (www.sealedenvelope.com). For this procedure, permuted block randomization with an allocation ratio of 1:1 and variable block sizes of 2 and 4 (randomly arranged) was employed. Because the study was open-label, blinding of group allocation to participants and e-coaches was not possible.
Following randomization, participants were informed about their group allocation, and the IG was given immediate access to the intervention with e-coach guidance. At this point, WL participants only received an information leaflet (the same as the IG) about alternative support options such as psychotherapy, student counseling services, or helplines, and were encouraged to consult the leaflet and seek support if they noticed a deterioration of wellbeing. Six weeks (t1) after randomization, post-assessment took place and WL participants received access to the same intervention as the IG, but without e-coach guidance. Instead, WL participants only received support from the study team in case of technical difficulties. Both IG and the WL participants were informed that the intervention involves some kind of support but did not know about differences in guidance to prevent potential bias.
The intervention StudiCare Mindfulness integrated elements of acceptance and commitment therapy (ACT) (S. C. Hayes et al., 1999), mindfulness-based stress reduction (MBSR) (Kabat-Zinn, 1982), and general stress management techniques (Kaluza, 2015). The intervention was developed by the Department for Clinical Psychology and Psychotherapy of Ulm University in collaboration with psychology students (“by students, for students”). All five modules had a different focus and were developed to be completed in about 60 min (see Table 3 for a detailed description). Contents were chosen based on easy learnability, applicability, and usability for everyday college life. Even though they were a mixture of the three different approaches mentioned above, care was taken to address all six core processes of ACT (Being present, Acceptance, Cognitive Defusion, Self as Context, Values, Committed Action). Participants were recommended to work on one module each week. At the beginning of each module, participants were encouraged to review their most and least mindful moments. Contents of the intervention were mostly provided via text, images, case examples, and interactive elements (e.g., questionnaires), and also emphasized the regular practice of formal (e.g., body scan) and informal (e.g., mindful nature walk) mindfulness exercises by providing a new audio file (á 5–10 min) each module. Homework assignments between modules promoted daily formal meditation practice. Intervention design and content were tailored to the college student population (e.g., student case examples, identification of study-related personal stressors). Participants could access the intervention on the Minddistrict platform (www.minddistrict.com), a company specializing in the provision of IMIs. The intervention was available via personal username and password on a 24/7 basis. All transferred data was secured based on ISO27001 and NEN7510 guidelines. Participants were informed that StudiCare Mindfulness is not a replacement for psychotherapy, recommended to seek counseling in case of distinctive mental health problems, and provided with further support options and contact details. To increase intervention adherence (Mohr et al., 2011), e-coaches (psychologists DV and KP, trained and supervised by HB and AK) gave weekly semi-standardized feedbacks after completion of each module specific to the participants’ input via the online-massaging system of the Minddistrict platform and responded to messages within two workdays. Additionally, they could be contacted by participants on demand. The main aim of the feedback messages was to provide positive reinforcement and encourage participants to continue working on the intervention. For this purpose, e-coaches also sent reminders if participants did not meet their self-chosen deadline for the next module. If participants did not respond to three reminders, the module was temporarily disabled until participants got back in touch with the e-coach.
Measurement took place before (t0; baseline) and 6 weeks after randomization (t1; post-intervention) via the online survey platform “Unipark.” An email reminder strategy was employed to minimize study dropout.
Measures
The primary outcome mindfulness was assessed with the short scale of the Freiburg Mindfulness Inventory (FMI) (Walach et al., 2006). The 14 items are rated on a 4-point scale (1 = “rarely” to 4 = “almost always”; total score: 14–56). It was chosen due to its brevity and multi-aspect operationalization of the mindfulness construct, covering the aspects “Mindful presence,” “Non-judgmental Acceptance,” “Openness to experience,” and “Insight.” However, as factor analysis revealed high inter-correlations between these aspects, the FMI measures mindfulness as a holistic, single-factor construct. Because it is semantically independent of a Buddhist or meditation context, the FMI is also suitable for participants without meditation experience. It has previously demonstrated high internal consistency (α = 0.84) (Heidenreich et al., 2006), as well as sensitivity to change (Walach et al., 2006). In this study, Cronbach’s α was 0.73 and McDonald’s ω was 0.72.
The widely used 9-item depression screening of the Patient Health Questionnaire (PHQ-9) was used to measure depressive symptoms (Kroenke & Spitzer, 2002). The nine items range from 0 = “not at all” to 3 = “nearly every day” (total score: 0–27). The PHQ-9 has proven to be a valid instrument with excellent internal consistency of Cronbach’s α = 0.89 (Kroenke et al., 2001). A Cronbach α of 0.72 and a McDonald ω of 0.71 were calculated in this study.
The 7-item Generalized Anxiety Disorder Questionnaire (GAD-7) (Spitzer et al., 2006) was used for assessing anxiety. It is rated on a 4-point scale from 0 = “not at all” 3 = to “nearly every day” (total score: 0–21) and is a valid and reliable screening instrument for anxiety with a high internal consistency of Cronbach’s α = 0.89 (Löwe et al., 2008). In this study, Cronbach’s α of 0.85 and McDonald’s ω of 0.86 were found.
Subjectively experienced stress was measured using the Perceived Stress Questionnaire (PSQ-20) (Fliege et al., 2005). The PSQ-20 consists of 20 items rated on a 4-point Likert scale from 1 = “almost never” to 4 = “usually” (total score: 0–100). Its four subscales (worries, tension, joy, demands) with five items each were shown to have satisfactory internal consistencies with Cronbach’s α = 0.80–0.86 (Fliege et al., 2005). Both Cronbach’s α and McDonald’s ω were 0.91 in this study.
The Short-Form Survey 12 (SF-12) is a widely used instrument to measure health-related quality of life (Ware et al., 1996). It consists of 12 items and two subscales, the physical component summary score (PCS) and the mental component summary score (MCS) (total scores: 0–100). The SF-12 has been demonstrated to be psychometrically valid and reliable, with Cronbach’s α of 0.89 for the PCS and 0.79 for the MCS (Wirtz et al., 2018). In this study, for the PCS Cronbach’s α was 0.65 and McDonald’s ω was 0.69, and for the MCS Cronbach’s α was 0.74 and McDonald’s ω was 0.75.
Acceptability was operationalized by assessing intervention satisfaction and adherence. Based on the Client Satisfaction Questionnaire (CSQ-8) (Larsen et al., 1979), four items were created to briefly assess intervention satisfaction (“To what extent did our online-training meet your needs?”). The items were rated on a 4-point scale of specific response alternatives (e.g., 1 = “met almost all of my needs,” 4 = “didn’t meet any of my needs”). Additionally, participants rated each module regarding how much they liked it on a 10-point scale (1 = “not at all,” 10 = “very much”). Adherence was assessed by recording the number of modules completed, defining “per protocol” (PP) adherence as the percentage of participants that completed at least 4 out of 5 modules (80% of the intervention) 6 weeks after randomization (t1). Finally, quantitative and qualitative data were collected on participants’ satisfaction with various aspects of the intervention using self-constructed items (e.g., “What could be optimized?”).
Several sociodemographic and other variables were assessed to investigate potential effect-modifying influences: age, gender, marital status, psychotherapy experience and baseline mindfulness, depressive symptoms, anxiety symptoms, and stress. Additionally, baseline personality scores were assessed via the Big Five Inventory (BFI-10) (Rammstedt & John, 2007), which measures the five dimensions extraversion, agreeableness, conscientiousness, neuroticism, and openness. Two items for each dimension are rated on a 5-point Likert scale from 1 = “disagree strongly” to 5 = “agree strongly” (total scores: 1–5). The BFI-10 has been demonstrated to have acceptable validity and reliability (test–retest reliability: 0.65–0.87) (Rammstedt & John, 2007). In this study, test–retest reliability of the five dimensions was 0.64 to 0.85. Finally, the Attitudes towards Psychological Online Interventions Questionnaire (APOI) (Schröder et al., 2015) was employed to measure attitudes towards IMI. It consists of 16 items that form a total score (16–80) as well as four sub-dimensions (“Skepticism and Perception of Risks,” “Confidence in Effectiveness,” “Technologization Threat,” “Anonymity Benefits”; total scores: 4–20) and is rated on a 5-point Likert scale from 1 = “totally agree” to 5 = “totally disagree.” The APOI has previously demonstrated acceptable to good internal consistency with Cronbach’s α of 0.77 (Schröder et al., 2015). Both Cronbach’s α and McDonald’s ω in this study were α = 0.70. For the moderator analyses, only the baseline total score was tested.
Data Analyses
All statistical analyses were performed with IBM SPSS (version 26) with a significance level of α = 0.05 (two-sided). Reliability of outcome measures was assessed by calculating both Cronbach’s alpha (α) and McDonald’s omega (ω) at t0. An exception was the BFI-10, for which test–retest reliability was calculated due to only two items in each dimension.
Data analyses were conducted according to intention-to-treat (ITT) principle, comprising all randomized participants. Missing data was imputed employing a Markov chain Monte Carlo multivariate imputation algorithm (van Buuren, 2007), setting all viable variables from t0 and t1 as predictors. N = 20 datasets were imputed. We assumed data to be missing at random (Enders, 2010). Predictive mean matching was applied as the imputation method (Little, 1988). Additional per-protocol analyses (PP) were conducted for intervention completers to examine potential influence of intervention adherence on effectiveness. Following the PP definition above, these subanalyses (n = 122) included all IG participants who completed at least 80% of the intervention (4 of 5 modules) at t1. Additionally, to investigate potential baseline differences between intervention completers and dropouts, independent samples t-tests (continuous variables) or chi-squared tests (discrete variables) were calculated.
To examine group differences post-intervention (t1), general linear modeling (GLM) was utilized. While checking assumptions for the initially planned ANCOVAs, unequal regression slopes were detected for some of the secondary outcome variables, violating the assumption of homogeneity of regression slopes. Consequently, a switch to GLM was decided to account for interactions between group variable and baseline scores. For these respective secondary outcome variables (depressive symptoms, anxiety symptoms, stress), interactions were added to the regression models and reported accordingly. To further examine significant interactions between participants’ baseline characteristics and outcome variables, simple slopes analyses were conducted via the “Process” macro for SPSS, version 3.5 (A. Hayes, 2017). Dichotomous variables were dummy-coded; continuous variables were z-standardized. Means (M), standard deviations (SD), standardized regression coefficients (β), and their 95% confidence intervals (CI) were reported. Additionally, Cohen’s d (within-group, between-groups) along with 95% CI was calculated. Following Cohen’s rule of thumb (Cohen, n.d.), d = 0.2 was interpreted as a small, d = 0.5 a medium, and d = 0.8 a large effect.
For the primary outcome mindfulness (FMI), Reliable Change Index (RCI) was calculated in order to assess the number of participants achieving a reliable, positive outcome vs. no change vs. reliable deterioration (Jacobson & Truax, 1991; Morley & Dowzer, 2014) using the following formula: 1.96 * SD * sqrt(2) * sqrt(1—rel). We used the SD of the whole sample at t0 (SD = 4.43) and the internal reliability of the FMI (α = 0.84) according to the test authors (Walach et al., 2006). If participants’ FMI score increased or decreased more than 4.91 points from t0 to t1, they were coded as reliably improved reliably deteriorated, respectively.
Moderation and Mediation Analyses
Moderation and mediation analyses of the intervention effect on mindfulness at post-intervention (t1) were conducted using the “Process” macro for SPSS, version 3.5 (A. Hayes, 2017). Dichotomous variables were dummy-coded, and multicategorical variables were dichotomized (e.g., civil status into “single” vs. “in partnership”). Continuous variables were z-standardized. Beta, HC3 heteroscedasticity consistent standard errors (SE) (Long & Ervin, 2000), t-statistics (t), and 95% CIs were reported.
For moderation analyses, bilinear interaction models were calculated with the primary outcome mindfulness as a dependent variable while controlling for baseline mindfulness. In case of significant interactions, moderation effects were further tested via simple slopes analyses (high level of variable: + 1 SD; average level: M; low level: − 1 SD).
For mediation analyses, a potential mediating effect of mindfulness (FMI) at t1 on the relationship between group and outcome variables of depressive symptoms (PHQ-9), anxiety symptoms (GAD-7), and stress (PSQ-20) at t1 was examined while controlling for the respective baseline values. A separate mediation model was tested for each of these outcome variables. Bootstrapped 95% bias-corrected CIs were computed with 1000 resamples. Instead of applying the casual steps strategy (Baron & Kenny, 1986), this approach focuses on the indirect effect (a*b) as the difference between the total (c = c’ + a*b) and the direct effect (c’). This method has been shown to have superior power and robustness towards violations of regression assumptions (Preacher & Hayes, 2008). The indirect effect of group on post-intervention depressive symptoms, stress, and anxiety symptoms through the proposed mediator (post-intervention mindfulness) was considered significant if the bootstrapped 95% CI did not cross 0. Non-bootstrapped path coefficients were also computed for the effect of group on mediator (path a), group on respective outcome variable while controlling for predictor variable (path b), and group on respective outcome variable while controlling for the mediator (path c'). Additionally, for each of these path coefficients, baseline values of moderator and respective outcome variable were statistically controlled for (see Fig. 2 in supplementary material).
Results
Primary Outcome
Six weeks post-intervention (t1), mindfulness was significantly improved by 1.18 standard deviations in intervention group (IG) compared to waitlist control group (WL) (β = 1.18, 95% CI: 0.96 to 1.40, p > 0.001), corresponding to a between-group effect size of d = 1.37 (95% CI: 1.01; 1.73) (see Table 2).
Reliable Improvement and Deterioration
More participants in IG compared to WL showed reliable improvement in mindfulness (IG: n = 74, 77.0%, WL: n = 75, 10.7%; χ2(1) = 66.70, p < 0.001). Additionally, fewer patients in the IG compared to the WL showed reliable deterioration (IG: n = 74, 1.4%; WL: n = 75, 10.7%; χ2(1) = 5.70, p < 0.034).
Secondary Outcomes
For four of the five secondary outcomes, significant group differences were found in IG compared to WL at t1 (see Table 2 for overview and Table 5 in the supplementary material for detailed regression results). For depressive symptoms (interaction: F(3, 145) = − 2.06, p = 0.041), anxiety symptoms (interaction: F(3, 145) = − 2.72, p = 0.007), and stress (interaction: F(3, 145) = − 3.11, p = 0.002), interactions of group and respective baseline values were significant and therefore added to the model. For these three outcomes, size and, in one case (anxiety symptoms), even significance of the intervention effect depended on participants’ baseline level of the respective outcome. Depressive symptoms were significantly reduced by 0.75 standard deviations in IG compared to WL at average baseline depressive symptom level (β = − 0.75, 95% CI: − 0.99 to − 0.51, p < 0.001). Participants with low baseline depressive symptoms (− 1 SD) profited less from the intervention (β = − 0.50, 95% CI: − 0.84 to − 0.16), whereas participants high on baseline depressive symptoms (+ 1 SD) benefited the most (β = − 1.00, 95% CI: − 1.34 to − 0.66). Similar results were found for stress, which was also significantly reduced in IG compared to WL at average baseline stress level (β = − 0.94, 95% CI: − 1.17 to − 0.72, p < 0.001). Participants with low baseline stress (− 1 SD) profited less from the intervention (β = − 0.59, 95% CI: − 0.90 to − 0.27), whereas participants with high baseline stress level (+ 1 SD) benefited the most (β = − 1.30, 95% CI: − 1.61 to − 0.98). Finally, anxiety symptoms were also significantly decreased in IG compared to WL at average baseline anxiety level (β = − 0.49, 95% CI: − 0.77 to − 0.22, p < 0.001). Participants with low baseline anxiety symptoms (− 1 SD) profited less from the intervention, with the CI crossing 0 and the difference between IG and WL no longer being significant at this level of baseline anxiety (β = − 0.11, 95% CI: − 0.50 to 0.28). Again, participants with high baseline anxiety levels (+ 1 SD) benefited the most from the intervention (β = − 0.87, 95% CI: − 1.27 to − 0.48).
The mental quality of life component was significantly improved by 0.70 standard deviations (β = 0.70, 95% CI: 0.32 to 0.60, p < 0.001). No significant differences were found for the physical quality of life component (β = 0.02, 95% CI: − 0.26 to 0.30).
Per-Protocol Analyses
For the primary outcome mindfulness, per-protocol analysis (PP; all IG participants that had completed at least 80% of the intervention at t1) showed similar results to the ITT analysis (β = 1.25, 95% CI: 0.99 to 1.50, p < 0.001). The same applies for the secondary outcomes physical (β = − 0.04, 95% CI: − 0.39 to 0.30, p = 0.801) and mental quality of life (β = 0.75, 95% CI: 0.42 to 1.07, p < 0.001). PP effects for depressive symptoms (β = − 0.79, 95% CI: − 1.06 to − 0.51, p < 0.001), stress (β = − 0.96, 95% CI: − 1.22 to − 0.69, p < 0.001) and anxiety symptoms (β = − 0.50, 95% CI: − 0.83 to − 0.17, p = 0.003) were also similar to ITT results. However, intervention effects no longer varied with baseline levels of the respective outcomes.
Intervention Adherence and Satisfaction
At t1, participants of the IG had completed an average of 3.57 modules (SD = 1.55), which equals around 70% of the intervention. Seventy participants had completed module 1 (95%), 64 completed module 2 (86%), 55 module 3 (74%), 48 module 4 (65%), and 27 had completed all modules (36%). Consequently, two-thirds of IG participants were adherent according to the “per protocol” definition (4 of 5 modules completed). No significant differences between adherent and non-adherent participants were found on any of the baseline variables. Participants were able to keep using the intervention after t1, increasing the average number of modules in the IG to 4.00 (SD = 1.58; 80% of the intervention) by the time of data analysis in June 2020. In IG participants that took part in t1 assessment (n = 62), satisfaction with the intervention was high. The intervention was rated as excellent or good by 95%, 90% would definitely or probably recommend it to a friend, 90% definitely or generally received the intervention they had hoped for, and 87% stated that their needs were almost all or mostly met. The same applies to satisfaction with every single module, with a medium of M = 8.08 (SD = 0.41) on a 10-point scale. The highest-rated module was module 5 (“Being mindful towards yourself”) with M = 8.60 (SD = 1.54), whereas the lowest-rated module was module 4 (“What makes your life valuable?”) with M = 7.39 (SD = 2.42).
Moderators
Of the variables potentially moderating the effect of the intervention on the primary outcome mindfulness at t1, only baseline level of BFI-10 personality dimension “Openness to experience” was found to significantly moderate intervention effect (interaction: β = − 0.24, 95% CI: − 0.44 to − 0.04; p = 0.018). Mindfulness at t1 was increased most effectively in participants low on baseline openness (− 1 SD; β = 1.42, 95% CI: 1.17 to 1.68) in IG compared to WL, whereas participants with high baseline openness levels (+ 1 SD; β = 0.94, 95% CI: 0.62 to 1.27) benefited the least. None of the other examined moderator variables yielded significant results (see Table 6 in the supplementary material).
Mediators
Table 4 reports the results of the mediation analyses for the three outcome variables, which examined whether mindfulness at t1 mediated the association between group and depressive symptoms/anxiety symptoms/stress at t1 for the IG versus the WL, controlling for the baseline values of mindfulness and the respective outcome variable (for path diagrams, see Fig. 2 in supplementary material). Mindfulness at t1 was found to mediate the association between being in IG vs. WL and depressive symptoms, anxiety symptoms, and stress 6 weeks post-intervention (t1), which is indicated by bootstrapped 95% confidence intervals of the indirect effects (a*b) not crossing 0.
Discussion
This randomized controlled trial (RCT) evaluated the effectiveness of a guided Internet- and mobile-based intervention (IMI) based on mindfulness-based stress reduction and Acceptance and Commitment Therapy (StudiCare Mindfulness) in a sample of German-speaking college students. Our results confirmed effectiveness for our primary outcome mindfulness and also suggested significant effects on secondary outcomes. Additionally, within our exploratory analyses, mindfulness was found to mediate intervention effects on depressive symptoms, anxiety symptoms, and stress. The only variable found to moderate intervention effectiveness on mindfulness was the personality trait “Openness to experience.” Finally, intervention adherence and satisfaction turned out to be adequate, suggesting StudiCare Mindfulness to be an acceptable intervention for the college student population.
StudiCare Mindfulness yielded moderate to large effects for all outcomes except the physical component of quality of life. Consequently, our results contribute to existing evidence for the potential effectiveness of mindfulness- and ACT-based IMIs in college students. The fact that we found the largest effect of the intervention for the primary outcome mindfulness, together with the substantial positive effect on quality of life, strengthens the conceptualization of ACT as a positive psychology intervention could make a valuable contribution to mental health prevention and promotion (Howell & Passmore, 2019). Our effects were considerably larger than the ones found by meta-analyses on the effectiveness of mental health IMI in general and mindfulness- and ACT-based IMI in particular (Brown et al., 2016; Harrer et al., 2019; Jayewardene et al., 2017; Spijkerman et al., 2016). These meta-analyses reported small effects of IMIs on mindfulness, depression, anxiety, and stress. Compared to Spijkerman et al.’s results, our between-groups effect sizes for mindfulness and depressive symptoms lay above their calculated confidence intervals. These findings might be explained by the fact that StudiCare Mindfulness was realized as a guided IMI. Research has shown effectiveness of guided IMI to be superior to unguided ones, potentially because guidance fosters adherence in participants (Baumeister et al., 2014). Non-significant findings for the physical component of quality of life might be explained by the fact that the physical component summary score of the SF-12 (Ware et al., 1995) mainly assesses aspects of physical health that were not addressed by our intervention (e.g., difficulties with climbing multiple steps of stairs).
Concerning baseline symptomatology, our sample was characterized by high stress levels corresponding to those found in psychosomatic patients (Fliege et al., 2001), high levels of neuroticism (Rammstedt et al., 2012), low mental quality of life (Ware et al., 1996), and mild depressive (Kroenke et al., 2001) and anxiety (Spitzer et al., 2006) symptomatology. However, average PHQ-9 and GAD-7 scores lay below the recommended cutoff score of 10 for diagnosing both depression (Kroenke et al., 2001) and generalized anxiety disorder (Spitzer et al., 2006). Thus, it seems that by offering a low-threshold, resource-oriented, non-stigmatizing, and generic intervention, we might have reached students with subclinical mental health problems. Additionally, our secondary analyses suggest that those symptoms were significantly reduced by the intervention, which could potentially help prevent the development of mental disorders.
Simple slope analyses proposed that StudiCare Mindfulness reduces baseline symptomatology most effectively for participants with high baseline depressive symptoms, anxiety symptoms, and stress. Those findings align with results from previous research that found more pronounced symptomatology to be associated with greater intervention effects (Button et al., 2012; Spek et al., 2008; Warmerdam et al., 2013). This suggests that StudiCare Mindfulness could be useful in both prevention and treatment of depression and anxiety. However, these results need to be interpreted with caution as analyses were exploratory, and the respective interactions were no longer significant in the PP analyses.
Mediation analyses found mindfulness to mediate the effect of the intervention on depressive symptoms, anxiety symptoms, and stress. These findings suggest that the acquisition of mindfulness skills is an important working mechanism behind the efficacy of mindfulness IMIs on mental health outcomes. Our results align with earlier findings from face-to-face settings (Gu et al., 2018; Pots et al., 2016). They also support a recent meta-analysis, concluding that approach-specific mediators found in face-to-face depression therapy (i.e., mindfulness in ACT) might be just as active in depression IMIs (Domhardt et al., 2021).
Moderation analyses mainly were non-significant. Although analyses were exploratory, this might indicate that our IMI increased mindfulness in all participants of this specific population equally effectively. Systematic evidence concerning moderators of mindfulness- and ACT-based interventions is still inconclusive and sparse (Pots et al., 2016), particularly for IMI and the outcome mindfulness. Confirming existing research (Kuyken et al., 2016), we did not find sociodemographic variables to moderate intervention effectiveness. Contrary to earlier findings, we could not confirm that participants with higher baseline mindfulness (Shapiro et al., 2011), neuroticism (de Vibe et al., 2015), or extraversion (Nyklíček & Irrmischer, 2017) benefited more from our intervention. However, all cited studies except Shapiro et al. (2011) used outcomes other than mindfulness (e.g., anxiety, depression). Concerning baseline depression, anxiety, and stress, we did find baseline values to moderate the effect on the respective outcomes, which is in line with previous findings (Kuyken et al., 2016; Pots et al., 2016). However, we did not find these variables to moderate the primary outcome mindfulness. The personality trait “Openness to experiences” was the only variable that significantly moderated intervention effect on mindfulness. Interestingly, the increase in mindfulness in the IG compared to the WL was most prominent in participants with low baseline openness. Mindfulness comprises the concepts of attention, curiosity, and receptivity, suggesting a positive relationship to openness to experience (Giluk, 2009). Consequently, individuals low on openness might also be low on specific aspects of mindfulness and therefore benefit more from the intervention.
Intervention satisfaction was high, and adherence was adequate. On average, participants had completed 70% of the intervention after 6 weeks (t1), and 65% were adherent according to the per-protocol definition of four modules at t1. No significant baseline differences were found between adherent and non-adherent participants, suggesting applicability of StudiCare Mindfulness regardless of the assessed baseline characteristics. Spijkerman et al. (2016) reported adherence rates of 35 to 92% and found guided IMI to be superior especially for stress (guided: g = 0.89; unguided: g = 0.19) and mindfulness (guided: g = 0.43; unguided: g = 0.22). This increased effectiveness, possibly through better adherence (Baumeister et al., 2014), poses the interesting question of how much guidance is needed vs. willingness to pay for guidance. This is particularly relevant in the context of scalable health promotion IMI. Future research should address whether the impact of human guidance on the effectiveness of mindfulness-based IMIs can be reduced by concepts like “guidance on demand” or persuasive design optimized IMI (Baumeister et al., 2019; Küchler et al., 2020).
In summary, the results of this trial suggest that StudiCare Mindfulness could provide an effective and acceptable way to support college students improve their mindfulness and mental health. If results can be replicated in further trials, StudiCare Mindfulness might offer a low-threshold prevention and treatment option for college students. Future research should examine if and how StudiCare Mindfulness could be implemented as a scalable intervention utilized on a population level.
Limitations and Future Research
First, this study lacks long-term follow-up assessment, which made evaluation of long-term effects impossible.
A second limitation is our choice of a waitlist control group. It has been discussed that using passive control groups can be associated with bias in estimating intervention effects (i.e., overestimation) (Furukawa et al., 2014). Future studies could evaluate the effectiveness of StudiCare Mindfulness in comparison to attention placebo or alternative interventions such as face-to-face mindfulness training.
Third, our study design did not allow us to evaluate effectiveness of the Internet-based intervention independent of e-coaching. To answer this question and ensure intervention scalability, future trials should dismantle the effectiveness of an unguided versus guided version of StudiCare Mindfulness.
A fourth limitation concerns the exploratory mediation and moderation analyses. Because we only had two assessment time points, we could not establish chronology of change in the mediation analyses (Kazdin, 2007). Therefore, we cannot definitively exclude the possibility that mediation flows in a different direction. Additionally, other meaningful mediation variables might be at work that we did not explore, such as constructs specific to ACT (e.g., psychological flexibility, meaningfulness). Because of our limited sample size, we might have failed to find existing moderators due to insufficient power. Furthermore, our eligibility criteria and recruitment measures resulted in restricted variance for some variables (e.g., low mindfulness, young college students, positive attitudes towards IMI). This might have limited the generalizability of the results of both the main and exploratory analyses.
A fifth limitation concerns the fact that the exclusive use of self-report instruments can lead to overestimating intervention effects (e.g., social desirability bias) (Nederhof, 1985). One way to deal with this problem is to combine self-report data with psychobiological markers. StudiCare Mindfulness is currently being evaluated in another subsequent study that includes the examination of effects on psychobiological markers such as hair stress markers (Schultchen et al., 2020).
As no universally accepted definition of mindfulness exists, another important concern relates to the operationalization of mindfulness chosen for a given trial (Vam Dam et al., 2018). Following Van Dam et al.’s recommendations, we carefully outlined our primary outcome measure (mindfulness as holistic, single factor construct assessed with the Freiburg Mindfulness Inventory), mindfulness/meditation practices, and intervention protocol. When interpreting results, one must consider the boundaries associated with this specific operationalization of mindfulness. For example, we were not able to differentiate between different aspects of mindfulness or between state and trait mindfulness.
A final limitation concerns the potential negative effects of mindfulness, which we did not explore in this RCT. Although evidence points to the potential of mindfulness interventions for mental health promotion, researchers call for a better understanding of differential effects, adverse effects, and optimal dosage of such interventions (Britton, 2019). Future study designs should allow for a systematic investigation of these questions.
Data Availability
All principal investigators were given full access to the datasets. The dataset is stored on password-protected servers of Ulm University with restricted access. External researchers may get access to the final trial dataset on request (HB) depending on to be specified data security and data exchange regulation agreements.
References
American College Health Association. (2020). American College Health Association-National College Health Assessment III: Reference group executive summary spring 2020. American College Health Association.
Auerbach, R. P., Mortier, P., Bruffaerts, R., Alonso, J., Benjet, C., Cuijpers, P., Demyttenaere, K., Ebert, D. D., Green, J. G., Hasking, P., Murray, E., Nock, M. K., Pinder-Amaker, S., Sampson, N. A., Stein, D. J., Vilagut, G., Zaslavsky, A. M., & Kessler, R. C. (2018). WHO World Mental Health Surveys International College Student Project: Prevalence and distribution of mental disorders. Journal of Abnormal Psychology, 127(7), 623–638. https://doi.org/10.1037/abn0000362
Baron, R. M., & Kenny, D. A. (1986). The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51(6), 1173–1182. https://doi.org/10.1037/0022-3514.51.6.1173
Baumeister, H., Reichler, L., Munzinger, M., & Lin, J. (2014). The impact of guidance on internet-based mental health interventions — a systematic review. Internet Interventions, 1(4), 205–215. https://doi.org/10.1016/j.invent.2014.08.003
Baumeister, H., Kraft, R., Baumel, A., Pryss, R., & Rathner, E. (2019). Persuasive e-Health design for behavior change. In H. Baumeister & R. Pryss (Eds.), Mobile sensing and digital penotyping (pp. 261–276). Springer.
Britton, W. B. (2019). Can mindfulness be too much of a good thing? The value of a middle way. Current Opinion in Psychology, 28(1), 159–165. https://doi.org/10.1016/j.copsyc.2018.12.011
Brown, M., Glendenning, A., Hoon, A. E., & John, A. (2016). Effectiveness of web-delivered acceptance and commitment therapy in relation to mental health and well-being: A systematic review and meta-analysis. Journal of Medical Internet Research, 18(8), e221. https://doi.org/10.2196/jmir.6200
Bruffaerts, R., Mortier, P., Kiekens, G., Auerbach, R. P., Cuijpers, P., Demyttenaere, K., Green, J. G., Nock, M. K., & Kessler, R. C. (2018). Mental health problems in college freshmen: Prevalence and academic functioning. Journal of Affective Disorders, 225(1), 97–103. https://doi.org/10.1016/j.jad.2017.07.044
Bruffaerts, R., Mortier, P., Auerbach, R. P., Alonso, J., Hermosillo De la Torre, A. E., Cuijpers, P., Demyttenaere, K., Ebert, D. D., Green, J. G., Hasking, P., Stein, D. J., Ennis, E., Nock, M. K., Pinder-Amaker, S., Sampson, N. A., Vilagut, G., Zaslavsky, A. M., & Kessler, R. C. (2019). Lifetime and 12-month treatment for mental disorders and suicidal thoughts and behaviors among first year college students. International Journal of Methods in Psychiatric Research, 28(2), e1764. https://doi.org/10.1002/mpr.1764
Button, K. S., Wiles, N. J., Lewis, G., Peters, T. J., & Kessler, D. (2012). Factors associated with differential response to online cognitive behavioural therapy. Social Psychiatry and Psychiatric Epidemiology, 47(5), 827–833. https://doi.org/10.1007/s00127-011-0389-1
Carlbring, P., Andersson, G., Cuijpers, P., Riper, H., & Hedman-Lagerlöf, E. (2018). Internet-based vs face-to-face cognitive behavior therapy for psychiatric and somatic disorders: an updated systematic review and meta-analysis. Cognitive Behaviour Therapy, 47(1), 1–18. https://doi.org/10.1080/16506073.2017.1401115
Cohen, J. (n.d.). Statistical power analysis for the behavioral sciences. Lawrence Erlbaum.
de Vibe, M., Solhaug, I., Tyssen, R., Friborg, O., Rosenvinge, J. H., Sorlie, T., Halland, E., & Bjorndal, A. (2015). Does personality moderate the effects of mindfulness training for medical and psychology students? Mindfulness (N Y), 6(2), 281–289. https://doi.org/10.1007/s12671-013-0258-y
Domhardt, M., Steubl, L., Boettcher, J., Buntrock, C., Karyotaki, E., Ebert, D. D., Cuijpers, P., & Baumeister, H. (2021). Mediators and mechanisms of change in internet- and mobile-based interventions for depression: A systematic review. Clinical Psychology Review, 83(1), 101953. https://doi.org/10.1016/j.cpr.2020.101953
Donker, T., Blankers, M., Hedman, E., Ljótsson, B., Petrie, K., & Christensen, H. (2015). Economic evaluations of internet interventions for mental health: A systematic review. Psychological Medicine, 45(16), 3357–3376. https://doi.org/10.1017/S0033291715001427
Ebert, D. D., Cuijpers, P., Muñoz, R. F., & Baumeister, H. (2017). Prevention of mental health disorders using internet- and mobile-based interventions: A narrative review and recommendations for future research. Frontiers in Psychiatry, 8(116), 1–16. https://doi.org/10.3389/fpsyt.2017.00116
Ebert, D. D., Van Daele, T., Nordgreen, T., Karekla, M., Compare, A., Zarbo, C., Brugnera, A., Øverland, S., Trebbi, G., Jensen, K. L., Kaehlke, F., & Baumeister, H. (2018). Internet- and mobile-based psychological interventions: Applications, efficacy, and potential for improving mental health. European Psychologist, 23(2), 167–187. https://doi.org/10.1027/1016-9040/a000318
Ebert, D. D., Franke, M., Kählke, F., Küchler, A.-M., Bruffaerts, R., Mortier, P., Karyotaki, E., Alonso, J., Cuijpers, P., Berking, M., Auerbach, R. P., Kessler, R. C., & Baumeister, H. (2019a). Increasing intentions to use mental health services among university students. Results of a pilot randomized controlled trial within the World Health Organization’s World Mental Health International College Student Initiative. International Journal of Methods in Psychiatric Research, 28(2), e1754. https://doi.org/10.1002/mpr.1754
Ebert, D. D., Mortier, P., Kaehlke, F., Bruffaerts, R., Baumeister, H., Auerbach, R. P., Alonso, J., Vilagut, G., Martínez, K. U., Lochner, C., Cuijpers, P., Kuechler, A., Green, J., Hasking, P., Lapsley, C., Sampson, N. A., & Kessler, R. C. (2019b). Barriers of mental health treatment utilization among first-year college students: First cross-national results from the WHO World Mental Health International College Student Initiative. International Journal of Methods in Psychiatric Research, 28(2), e1782. https://doi.org/10.1002/mpr.1782
Enders, C. K. (2010). Applied missing data analysis. Guilford Press.
Faul, F., Erdfelder, E., Lang, A.-G., & Buchner, A. (2007). G*Power: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39(2), 175–191. https://doi.org/10.3758/BF03193146
Fliege, H., Rose, M., Arck, P., Levenstein, S., & Klapp, B. (2001). Validation of the “Perceived Stress Questionnaire” (PSQ) in a German sample. Diagnostica, 47(3), 142–152. https://doi.org/10.1026//0012-1924.47.3.142
Fliege, H., Rose, M., Arck, P., Walter, O. B., Kocalevent, R.-D., Weber, C., & Klapp, B. F. (2005). The Perceived Stress Questionnaire (PSQ) Reconsidered: Validation and reference values from different clinical and healthy adult samples. Psychosomatic Medicine, 67(1), 78–88. https://doi.org/10.1097/01.psy.0000151491.80178.78
Furukawa, T. A., Noma, H., Caldwell, D. M., Honyashiki, M., Shinohara, K., Imai, H., Chen, P., Hunot, V., & Churchill, R. (2014). Waiting list may be a nocebo condition in psychotherapy trials: A contribution from network meta-analysis. Acta Psychiatrica Scandinavica, 130(3), 181–192. https://doi.org/10.1111/acps.12275
Giluk, T. L. (2009). Mindfulness, Big Five personality, and affect: A meta-analysis. Personality and Individual Differences, 47(8), 805–811. https://doi.org/10.1016/j.paid.2009.06.026
Gu, J., Strauss, C., Bond, R., & Cavanagh, K. (2015). How do mindfulness-based cognitive therapy and mindfulness-based stress reduction improve mental health and wellbeing? A systematic review and meta-analysis of mediation studies. Clinical Psychology Review, 37(1), 1–12. https://doi.org/10.1016/j.cpr.2015.01.006
Gu, J., Cavanagh, K., & Strauss, C. (2018). Investigating the specific effects of an online mindfulness-based self-help intervention on stress and underlying mechanisms. Mindfulness, 9(4), 1245–1257. https://doi.org/10.1007/s12671-017-0867-y
Harrer, M., Adam, S. H., Fleischmann, R. J., Baumeister, H., Auerbach, R., Bruffaerts, R., Cuijpers, P., Kessler, R. C., Berking, M., Lehr, D., & Ebert, D. D. (2018). Effectiveness of an internet- and app-based intervention for college students with elevated stress: Randomized controlled trial. Journal of Medical Internet Research, 20(4), 1–16. https://doi.org/10.2196/jmir.9293
Harrer, M., Adam, S. H., Baumeister, H., Cuijpers, P., Karyotaki, E., Auerbach, R. P., Kessler, R. C., Bruffaerts, R., Berking, M., & Ebert, D. D. (2019). Internet interventions for mental health in university students: A systematic review and meta-analysis. International Journal of Methods in Psychiatric Research, 28(2), e1759. https://doi.org/10.1002/mpr.1759
Hayes, S. C. (2004). Acceptance and commitment therapy, relational frame theory, and the third wave of behavioral and cognitive therapies. Behavior Therapy, 35(4), 639–665. https://doi.org/10.1016/S0005-7894(04)80013-3
Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (1999). Acceptance and commitment therapy: An experiential approach to behavior change. Guilford Press.
Hayes, A. (2017). Introduction to mediation, moderation, and conditional process analysis: a regression-based approach. (2nd ed.). Guilford Publications.
Heidenreich, T., Ströhle, G., & Michalak, J. (2006). Achtsamkeit: Konzeptuelle Aspekte und Ergebnisse zum Freiburger Achtsamkeitsfragebogen. Verhaltenstherapie, 16(1), 33–40. https://doi.org/10.1159/000091521
Howell, A. J., & Passmore, H.-A. (2019). Acceptance and commitment training (ACT) as a positive psychological intervention: A systematic review and initial meta-analysis regarding ACT’s role in well-being promotion among university students. Journal of Happiness Studies, 20(6), 1995–2010. https://doi.org/10.1007/s10902-018-0027-7
Jacobson, N. S., & Truax, P. (1991). Clinical significance: A statistical approach to defining meaningful change in psychotherapy research. Journal of Consulting and Clinical Psychology, 59(1), 12–19. https://doi.org/10.1037/0022-006X.59.1.12
Jayewardene, W. P., Lohrmann, D. K., Erbe, R. G., & Torabi, M. R. (2017). Effects of preventive online mindfulness interventions on stress and mindfulness: A meta-analysis of randomized controlled trials. Preventive Medicine Reports, 5(1), 150–159. https://doi.org/10.1016/j.pmedr.2016.11.013
Kabat-Zinn, J. (1982). An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: Theoretical considerations and preliminary results. General Hospital Psychiatry, 4(1), 33–47. https://doi.org/10.1016/0163-8343(82)90026-3
Kabat-Zinn, J. (2003). Mindfulness-based interventions in context: Past, present, and future. Clinical Psychology: Science and Practice, 10(2), 144–156. https://doi.org/10.1093/clipsy.bpg016
Kählke, F., Küchler, A.-M., Baumeister, H., & Ebert, D. D. (2019). StudiCare erfolgreich und gesund studieren –ein umfassendes deutsches und internationales Projekt zur Förderung der psychischen Gesundheit von Studierenden. E-Beratungsjournal, 2, 133–156.
Kaluza, G. (2015). Stressbewältigung. Springer. https://doi.org/10.1007/978-3-662-44016-2
Kazdin, A. E. (2007). Mediators and mechanisms of change in psychotherapy research. Annual Review of Clinical Psychology, 3(1), 1–27. https://doi.org/10.1146/annurev.clinpsy.3.022806.091432
Kraemer, H. C., Wilson, T., Fairburn, C. G., & Argas, W. S. (2002). Mediators and moderators of treatment effects in randomized clinical trials. Archives of General Psychiatry, 59(1), 877–883. https://doi.org/10.1001/archpsyc.59.10.877
Kroenke, K., & Spitzer, R. L. (2002). The PHQ-9: A new depression diagnostic and severity measure. Psychiatric Annals, 32(9), 509–515. https://doi.org/10.3928/0048-5713-20020901-06
Kroenke, K., Spitzer, R. L., & Williams, J. B. W. (2001). The PHQ-9. Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613. https://doi.org/10.1046/j.1525-1497.2001.016009606.x
Küchler, A.-M., Schultchen, D., Pollatos, O., Moshagen, M., Ebert, D. D., & Baumeister, H. (2020). StudiCare mindfulness—study protocol of a randomized controlled trial evaluating an internet- and mobile-based intervention for college students with no and “on demand” guidance. Trials, 21(1), 975. https://doi.org/10.1186/s13063-020-04868-0
Kuyken, W., Warren, F. C., Taylor, R. S., Whalley, B., Crane, C., Bondolfi, G., Hayes, R., Huijbers, M., Ma, H., Schweizer, S., Segal, Z., Speckens, A., Teasdale, J. D., Van Heeringen, K., Williams, M., Byford, S., Byng, R., & Dalgleish, T. (2016). Efficacy of mindfulness-based cognitive therapy in prevention of depressive relapse an individual patient data meta-analysis from randomized trials. JAMA Psychiatry, 73(6), 565–574. https://doi.org/10.1001/jamapsychiatry.2016.0076
Larsen, D. L., Attkisson, C. C., Hargreaves, W. A., & Nguyen, T. D. (1979). Assessment of client/patient satisfaction: Development of a general scale. Evaluation and Program Planning, 2(3), 197–207. https://doi.org/10.1016/0149-7189(79)90094-6
Little, R. J. A. (1988). Missing-data adjustments in large surveys. Journal of Business and Economic Statistics, 6(3), 287–296. https://doi.org/10.1080/07350015.1988.10509663
Long, J. S., & Ervin, L. H. (2000). Using heteroscedasticity consistent standard errors in the linear regression model. The American Statistician, 54(3), 217–224. https://doi.org/10.2307/2685594
Löwe, B., Decker, O., Müller, S., Brähler, E., Schellberg, D., Herzog, W., & Herzberg, P. Y. (2008). Validation and standardization of the generalized anxiety disorder screener (GAD-7) in the general population. Medical Care, 46(3), 266–274. https://doi.org/10.1097/MLR.0b013e318160d093
Mohr, D. C., Cuijpers, P., & Lehman, K. (2011). Supportive accountability: A model for providing human support to enhance adherence to eHealth interventions. Journal of Medical Internet Research, 13(1), e30. https://doi.org/10.2196/jmir.1602
Morley, S., & Dowzer, C. N. (2014). Manual for the Leeds Reliable Change Indicator: Simple Excel(tm)applications for the analysis of individual patient and group data. University of Leeds.
Mortier, P., Auerbach, R. P., Alonso, J., Bantjes, J., Benjet, C., Cuijpers, P., Ebert, D. D., Green, J. G., Hasking, P., Nock, M. K., O’Neill, S., Pinder-Amaker, S., Sampson, N. A., Vilagut, G., Zaslavsky, A. M., Bruffaerts, R., Kessler, R. C., Boyes, M., Kiekens, G., & Vives, M. (2018). Suicidal thoughts and behaviors among first-year college students: Results from the WMH-ICS Project. Journal of the American Academy of Child and Adolescent Psychiatry, 57(4), 263-273.e1. https://doi.org/10.1016/j.jaac.2018.01.018
Nederhof, A. J. (1985). Methods of coping with social desirability bias: A review. European Journal of Social Psychology, 15(3), 263–280. https://doi.org/10.1002/ejsp.2420150303
Nyklíček, I., & Irrmischer, M. (2017). For whom does mindfulness-based stress reduction work? Moderating Effects of Personality. Mindfulness, 8(4), 1106–1116. https://doi.org/10.1007/s12671-017-0687-0
Nyklíček, I., van Son, J., Pop, V. J., Denollet, J., & Pouwer, F. (2016). Does mindfulness-based cognitive therapy benefit all people with diabetes and comorbid emotional complaints equally? Moderators in the DiaMind trial. Journal of Psychosomatic Research, 91(1), 40–47. https://doi.org/10.1016/j.jpsychores.2016.10.009
Pedrelli, P., Nyer, M., Yeung, A., Zulauf, C., & Wilens, T. (2015). College students: Mental health problems and treatment considerations. Academic Psychiatry, 39(5), 503–511. https://doi.org/10.1007/s40596-014-0205-9
Pots, W. T. M., Trompetter, H. R., Schreurs, K. M. G., & Bohlmeijer, E. T. (2016). How and for whom does web-based acceptance and commitment therapy work? Mediation and moderation analyses of web-based ACT for depressive symptoms. BMC Psychiatry, 16(1), 158. https://doi.org/10.1186/s12888-016-0841-6
Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 40(3), 879–891. https://doi.org/10.3758/BRM.40.3.879
Rammstedt, B., Kemper, C. J., Klein, M. C., Beierlein, C., & Kovaleva, A. (2012). Eine kurze Skala zur Messung der fünf Dimensionen der Persönlichkeit: Big-Five-Inventory-10 (BFI-10). In GESIS Working Papers 2012|23. GESIS.
Rammstedt, B., & John, O. (2007). Measuring personality in one minute or less: A 10-item short version of the Big Five Inventory in English and German. Journal of Research in Personality, 41(1), 203–212. https://doi.org/10.1016/j.jrp.2006.02.001
Schröder, J., Sautier, L., Kriston, L., Berger, T., Meyer, B., Späth, C., Köther, U., Nestoriuc, Y., Klein, J. P., & Moritz, S. (2015). Development of a questionnaire measuring attitudes towards psychological online interventions–the APOI. Journal of Affective Disorders, 187(1), 136–141. https://doi.org/10.1016/j.jad.2015.08.044
Schultchen, D., Küchler, A.-M., Schillings, C., Weineck, F., Karabatsiakis, A., Ebert, D. D., Baumeister, H., & Pollatos, O. (2020). Effectiveness of a guided online mindfulness-focused intervention in a student population: Study protocol for a randomised control trial. British Medical Journal Open, 10(3), e032775. https://doi.org/10.1136/bmjopen-2019-032775
Schulz, K. F., Altman, D. G., & Moher, D. (2010). CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMJ, 340, c332. https://doi.org/10.1136/bmj.c332
Segal, Z. V., Williams, M. G., & Teasdale, J. D. (2001). Mindfulness-based cognitive therapy for depression: A new approach to preventing relapse. The Guilford Press.
Shapiro, S. L., Brown, K. W., Thoresen, C., & Plante, T. G. (2011). The moderation of mindfulness-based stress reduction effects by trait mindfulness: Results from a randomized controlled trial. Journal of Clinical Psychology, 67(3), 267–277. https://doi.org/10.1002/jclp.20761
Shapiro, S. L., de Sousa, S., & Jazaieri, H. (2016). Mindfulness, mental health, and positive psychology. In I. Ivtzan & T. Lomas (Eds.), Mindfulness in positive psychology. Routledge.
Spek, V., Nyklíček, I., Cuijpers, P., & Pop, V. (2008). Predictors of outcome of group and internet-based cognitive behavior therapy. Journal of Affective Disorders, 105(1–3), 137–145. https://doi.org/10.1016/j.jad.2007.05.001
Spijkerman, M. P. J., Pots, W. T. M., & Bohlmeijer, E. T. (2016). Effectiveness of online mindfulness-based interventions in improving mental health: A review and meta-analysis of randomised controlled trials. Clinical Psychology Review, 45(1), 102–114. https://doi.org/10.1016/j.cpr.2016.03.009
Spitzer, R. L., Kroenke, K., Williams, J. B., & Löwe, B. (2006). The GAD-7. A brief measure for assessing generalized anxiety disorder. Archives of Internal Medicine, 166(10), 1092–1097. https://doi.org/10.1001/archinte.166.10.1092
Stallman, H. M., & Kavanagh, D. J. (2018). Development of an internet intervention to promote wellbeing in college students. Australian Psychologist, 53(1), 60–67. https://doi.org/10.1111/ap.12246
van Buuren, S. (2007). Multiple imputation of discrete and continuous data by fully conditional specification. Statistical Methods in Medical Research, 16(3), 219–242. https://doi.org/10.1177/0962280206074463
Van Dam, N. T., van Vugt, M. K., Vago, D. R., Schmalzl, L., Saron, C. D., Olendzki, A., Meissner, T., Lazar, S. W., Kerr, C. E., Gorchov, J., Fox, K. C. R., Field, B. A., Britton, W. B., Brefczynski-Lewis, J. A., & Meyer, D. E. (2018). Mind the hype: A critical evaluation and prescriptive agenda for research on mindfulness and meditation. Perspectives on Psychological Science, 13(1), 36–61. https://doi.org/10.1177/1745691617709589
Viskovich, S., & Pakenham, K. I. (2018). Pilot evaluation of a web-based acceptance and commitment therapy program to promote mental health skills in university students. Journal of Clinical Psychology, 74(12), 2047–2069. https://doi.org/10.1002/jclp.22656
Walach, H., Buchheld, N., Buttenmüller, V., Kleinknecht, N., & Schmidt, S. (2006). Measuring mindfulness - The Freiburg Mindfulness Inventory (FMI). Personality and Individual Differences, 40(8), 1543–1555. https://doi.org/10.1016/j.paid.2005.11.025
Ware, J. E., Kosinski, M., & Keller, S. D. (1996). A 12-item short-form health survey: Construction of scales and preliminary tests of reliability and validity. Medical Care, 34(3), 220–233. https://doi.org/10.1097/00005650-199603000-00003
Ware, J. E., Kosinski, M., & Keller, S. D. (1995). How to score the SF-12 physical and mental health summary scales. The Health Institute, New England Medical Center.
Warmerdam, L., Van Straten, A., Twisk, J., & Cuijpers, P. (2013). Predicting outcome of internet-based treatment for depressive symptoms. Psychotherapy Research, 23(5), 559–567. https://doi.org/10.1080/10503307.2013.807377
Wirtz, M. A., Morfeld, M., Glaesmer, H., & Brähler, E. (2018). Normierung des SF-12 Version 2.0 zur Messung der gesundheitsbezogenen Lebensqualität in einer deutschen bevölkerungsrepräsentativen Stichprobe. Diagnostica, 64(4), 215–226. https://doi.org/10.1026/0012-1924/a000205
World Health Organization. (2001). The World health report 2001. Mental health - new understanding, new hope. World Health Organization.
World Health Organization. (2013). Mental health action plan 2013–2020. World Health Organization.
Funding
Open Access funding enabled and organized by Projekt DEAL. The StudiCare project was funded by the BARMER, a major healthcare insurance company in Germany. BARMER had no role in development of the intervention, study design, data collection, analysis, decision to publish, or preparation of this manuscript or future manuscripts regarding the StudiCare project.
Author information
Authors and Affiliations
Contributions
DDE and HB obtained funding for this study. AK, DDE, and HB initiated this study. AK, FK, and HB contributed to the design of this study. AK, DV, KP, and HB developed intervention content. AK obtained ethics approval and coordinated the trial. DV and KP conducted participant management. AK conducted data analyses and wrote the draft of the manuscript. All the authors contributed to the further writing of the manuscript and interpretation of data. All the authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics Approval
All study procedures were approved by the ethics committee of the Ulm University (application no. 105/17; approval date: May 11, 2017).
Informed Consent
Participants received written information on study conditions, data security, voluntariness of participation, anonymized publication of results, and the right to leave the study at all times. Written consent was obtained from all participants prior to study entry. Data collection was pseudonymized and data was only accessed by authorized study personnel obliged to secrecy. After data collection was completed, personalized information was deleted and all data was completely anonymized.
Conflict of Interest
AK, HB, DV, and KP were involved in the development of StudiCare Mindfulness or its predecessor versions. AK has received fees for lectures/workshops from chambers of psychotherapists and health insurance companies. HB reports to have received consultancy fees and fees for lectures/workshops from chambers of psychotherapists and training institutes for psychotherapists in the e-mental-health context. DDE reports to have received consultancy fees/served in the scientific advisory board from several companies such as Minddistrict, Lantern, Schoen Kliniken, and German health insurance companies. He is a stakeholder of the Institute for health training online (GET.ON), which aims to implement scientific findings related to digital health interventions into routine care.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Küchler, AM., Kählke, F., Vollbrecht, D. et al. Effectiveness, Acceptability, and Mechanisms of Change of the Internet-Based Intervention StudiCare Mindfulness for College Students: a Randomized Controlled Trial. Mindfulness 13, 2140–2154 (2022). https://doi.org/10.1007/s12671-022-01949-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12671-022-01949-w