
Abstract
Aim
The aim of this study was to externally validate the four commonly used scoring systems in the risk stratification of patients with upper gastrointestinal bleed (UGIB).
Methods
Patients of UGIB who underwent endoscopy within 24 h of presentation were stratified prospectively using the pre-endoscopy Rockall score (PRS) >0, complete Rockall score (CRS) >2, Glasgow Blatchford bleeding scores (GBS) >3, and modified GBS (m-GBS) >3 scores. Patients were followed up to 30 days. Prognostic accuracy of the scores was done by comparing areas under curve (AUC) in terms of overall risk stratification, re-bleeding, mortality, need for intervention, and length of hospitalization.
Results
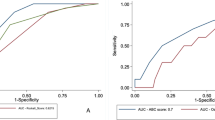
One hundred and seventy-five patients were studied. All four scores performed better in the overall risk stratification on AUC [PRS = 0.566 (CI: 0.481–0.651; p-0.043)/CRS = 0.712 (CI: 0.634–0.790); p<0.001)/GBS = 0.810 (CI: 0.744–0.877; p->0.001); m-GBS = 0.802 (CI: 0.734–0.871; p<0.001)], whereas only CRS achieved significance in identifying re-bleed [AUC—0.679 (CI: 0.579–0.780; p = 0.003)]. All the scoring systems except PRS were found to be significantly better in detecting 30-day mortality with a high AUC (CRS = 0.798; p-0.042)/GBS = 0.833; p-0.023); m-GBS = 0.816; p-0.031). All four scores demonstrated significant accuracy in the risk stratification of non-variceal patients; however, only GBS and m-GBS were significant in variceal etiology. Higher cutoff scores achieved better sensitivity/specificity [RS > 0 (50/60.8), CRS > 1 (87.5/50.6), GBS > 7 (88.5/63.3), m-GBS > 7(82.3/72.6)] in the risk stratification.
Conclusion
GBS and m-GBS appear to be more valid in risk stratification of UGIB patients in this region. Higher cutoff values achieved better predictive accuracy.



Similar content being viewed by others


References
Monjur A. Prevalence of upper gastrointestinal bleeding in a community hospital. Am J Gastroenterol. 2003;98:294–5.
Vreeburg EM, Terwee CB, Snel P, et al. Validation of the Rockall risk scoring system in upper gastrointestinal bleeding. Gut. 1999;44:331–5.
Balaban DV, Strambu V, Florea BG, Cazan AR, Bratucu M, Jinga M. Predictors for in hospital mortality and need for clinical intervention in upper GI bleeding: a 5-year observational study. Chirurg. 2014;109:48–54.
Dicu D, Pop F, Lonescu Dicu T. Comparison of risk scoring systems in predicting clinical outcome at upper gastrointestinal bleeding patients in an emergency unit. Am J Emerg Med. 2013;31:94–9.
Sung JJ, Chan FK, Chen M, et al. Asia–Pacific working group consensus on non-variceal upper gastrointestinal bleeding. Gut. 2011;60:1170–7.
McGinn TG, Guyatt GH, Wyer PC, Naylor CD, Stiell IG, Richardson WS. Users’ guides to the medical literature: how to use articles about clinical decision rules. Evidence based medicine working group. JAMA. 2000;284:79–84.
Laupacis A, Sekar N, Stiell G. Clinical prediction rules. A review and suggested modifications of methodological standards. JAMA. 1997;277:488–94.
Stanley AJ, Ashley D, Dalton HR, et al. Outpatient management of patients with low-risk upper-gastrointestinal hemorrhage: multicenter validation and prospective evaluation. Lancet. 2009;37:42–7.
Bryant RV, Kuo P, Williamson K, et al. Performance of the Glasgow Blatchford score in predicting clinical outcomes and intervention in hospitalized patients with upper GI bleeding. Gastrointest Endosc. 2013;78:576–83.
Singh SP, Panigrahi MK. Spectrum of upper gastrointestinal hemorrhage in coastal Odisha. Trop Gastroenterol. 2013;34:14–7.
Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic curve. Radiology. 1982;143:29–36.
Chandra S, Hess EP, Agarwal D, et al. External validation of the Glasgow –Blatchford bleeding score and the Rockall score in the US setting. Am J Emerg Med. 2012;30:673–9.
Rockall TA, Logan RF, Devlin HB. Risk assessment after acute upper gastrointestinal hemorrhage. Gut. 1996;38:316–21.
Blatchford O, Murray WR, Blatchford M. A risk score to predict need for treatment for upper gastrointestinal hemorrhage. Lancet. 2000;356:1318–21.
Longstreth GF. Epidemiology of hospitalization for acute upper gastrointestinal hemorrhage: a population-based study. Am J Gastroenterol. 1995;90:206–10.
Laine L, Peterson WL. Bleeding peptic ulcer. N Engl J Med. 1994;331:717–27.
Rockall TA, Logan RFA, Devlin HB, Northfield TC. Variation in outcome after acute upper gastrointestinal haemorrhage : the National Audit of acute upper gastrointestinal haemorrhage. Lancet. 1995;346:346–50.
Yavorski RT, Wong RK, Maydonovitch C, Battin LS, Furnia A, Amundson DE. Analysis of 3,294 cases of upper gastrointestinal bleeding in military medical facilities. Am J Gastroenterol. 1995;90:568–73.
Sanders DS, Perry MJ, Jones SGW, et al. Effectiveness of an upper-gastrointestinal haemorrhage unit: a prospective analysis of 900 consecutive cases using the Rockall score as a method of risk standardization. Eur J Gastroenterol Hepatol. 2004;16:487–94.
Sanders DS, Carter MJ, Goodchap RJ, et al. Prospective validation of the Rockall scoring system for upper GI haemorrhages in subgroup of patients with varices and peptic ulcers. Am J Gastroenterol. 2002;97:630–5.
Girardin M, Bertolini D, Ditisheim S, et al. Use of Glasgow-blatchford bleeding score reduces hospital stay duration and costs for patients with low-risk upper GI bleeding. Endosc Int Open. 2014;2:74–9.
Recio-Ramírez JM, Sánchez-Sánchez MP, Peña-Ojeda JA, et al. The predictive capacity of the Glasgow-Blatchford score for the risk stratification of upper gastrointestinal bleeding in an emergency department. Rev Esp Enferm Dig. 2015;107:262–7.
Bhattarai J, Acharya P, Barun B, Pokharel S, Uprety N, Shrestha UK. Comparison of endoscopic findings in patients from different ethnic groups undergoing endoscopy for upper gastrointestinal bleed in eastern Nepal. Nepal Med Coll J. 2007;9:173–5.
Wang CH, Chen YW, Young YR, Yang CJ, Chen IC. A prospective comparison of 3 scoring systems in upper gastrointestinal bleeding. Am J Emerg Med. 2013;31:775–8.
Stanley AJ. Update on risk scoring systems for patients with upper gastrointestinal haemorrhage. World J Gastroenterol. 2012;18:2739–44.
Shrestha UK, Sapkota S. Etiology and adverse outcome predictors of upper gastrointestinal bleeding in 589 patients in Nepal. Dig Dis Sci. 2012;59:814–22.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
ACA, SKM, SSM, TM, and VK declare that they have no conflict of interest.
Ethics statement
Institute ethics committee approved the study. The nature, methodology, and risks involved in the study were explained to the patient and informed consent was obtained. All the information collected was kept confidential and patient was given full freedom to withdraw at any point during the study. All provisions of the Declaration of Helsinki were followed in this study. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Institutional review board statement
The study was reviewed and approved by the JIPMER institute research committee and the institute ethics committee.
Informed consent statement
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Anchu, A.C., Mohsina, S., Sureshkumar, S. et al. External validation of scoring systems in risk stratification of upper gastrointestinal bleeding. Indian J Gastroenterol 36, 105–112 (2017). https://doi.org/10.1007/s12664-017-0740-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12664-017-0740-x