
Abstract
Objectives
Our aim was to explain the spectrum of clinical and CT findings in 18 patients with acute epiploic appendagitis.
Methods and Materials
We reviewed the clinical records and CT pictures of 18 consecutive patients seen in Nejran Armed Forces Hospital, Nejran, Kingdom of Saudi Arabia and Sohag University Hospital, Sohag, Egypt between July 2006 and June 2013 with a diagnosis of primary epiploic appendagitis.
Results
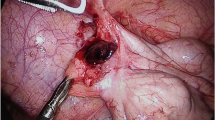
The age ranged between 22 and 64 years old with a mean of 44.3. Males were affected in 72 % of cases. Eleven patients had acute pain in left lower quadrant. Nausea and vomiting were encountered in four patients. No fever was recorded in all cases. Leukocytosis was found in four patients and C-reactive protein (CRP) was high in five. CT scan diagnosed primary epiploic appendagitis (PEA) in 15 patients, while 3 patients were diagnosed intraoperatively. The left colon was affected in 11 patients. All patients except one had a central fatty core surrounded by inflammation with size ranging between 1.5 and 3.5 cm in length. Fifteen patients were treated conservatively, and three cases underwent surgical exploration. Ten patients (55.5 %) completed the follow up schedule. Complete resolution was noted in three patients at 2 weeks, in six patients at 3 months, and only one patient had residual changes at 6 months.
Conclusion
PEA is a challenging clinical diagnosis, and CT scan is extremely necessary in diagnosing this disease accurately. The awareness of the surgeons concerning this rare occasion will avoid unnecessary hospital admission and operative treatment.







Similar content being viewed by others


References
Birjawi GA, Haddad MC, Zantout HM, Uthman SZ. Primary epiploic appendagitis: a report of two cases. Clin Imaging. 2000;24:207–9.
Ross JA. Vascular loops in the appendices epiploicae; their anatomy and surgical significance, with a review of the surgical pathology of appendices epiploicae. Br J Surg. 1950;37:464–6.
Horvath E, Majlis S, Seguel S, et al. Primary epiploic appendagitis: clinical and radiological diagnosis. Rev Med Chil. 2000;128:601–7.
Chowbey PK, Singh G, Sharma A, Khullar R, Soni V, Baijal M. Torsion of appendices epiploicae presenting as acute abdomen: laparoscopic diagnosis and therapy. Indian J Gastroenterol. 2003;22:68–9.
Singh AK, Gervais DA, Hahn PF, Rhea J, Mueller PR. CT appearance of acute appendagitis. AJR Am J Roentgenol. 2004;183:1303–7.
Son HJ, Lee SJ, Lee JH, et al. Clinical diagnosis of primary epiploic appendagitis: differentiation from acute diverticulitis. J Clin Gastroenterol. 2002;34:435–8.
Jang JI, Lim YS, Choi JW, Lee YS. Management of right colon diverticulitis. J Korean Soc Coloproctol. 2010;26:22–8.
Choi YU, Choi PW, Park YH, et al. Clinical characteristics of primary epiploic appendagitis. J Korean Soc Coloproctol. 2011;27:114–21.
Mollà E, Ripollés T, Martínez MJ, Morote V, Roselló-Sastre E. Primary epiploic appendagitis: US and CT findings. Eur Radiol. 1998;8:435–8.
Hwang JA, Kim SM, Song HJ, Lee YM. Differential diagnosis of left-sided abdominal pain: primary epiploic appendagitis vs colonic diverticulitis. World J Gastroenterol. 2013;19:6842–8.
Hiller N, Berelowitz D, Hadas-Halpern I. Primary epiploic appendagitis: clinical and radiological manifestations. Isr Med Assoc J. 2000;2:896–8.
Hanson JM, Kam AW. Paracolic echogenic mass in a man with lower abdominal pain. Is epiploic appendagitis more common than previously thought? Emerg Med J. 2006;23:e17.
Singh AK, Gervais DA, Hahn PF, Sagar P, Mueller PR, Novelline RA. Acute epiploic appendagitis and its mimics. Radiographics. 2005;25:1521–34.
Rao PM, Wittenberg J, Lawrason JN. Primary epiploic appendagitis: evolutionary changes in CT appearance. Radiology. 1997;204:713–7.
Danielson K, Chernin MM, Amberg JR, Goff S, Durham JR. Epiploic appendagitis: CT characteristics. J Comput Assist Tomogr. 1986;10:142–3.
Legome EL, Belton AL, Murray RE, Rao PM, Novelline RA. Epiploic appendagitis: the emergency department presentation. J Emerg Med. 2002;22:9–13.
Jalaguier A, Zins M, Rodallec M, Nakache JP, Boulay-Coletta I, Jullès MC. Accuracy of multidetector computed tomography in differentiating primary epiploic appendagitis from left acute colonic diverticulitis associated with secondary epiploic appendagitis. Emerg Radiol. 2010;17:51–6.
Unal E, Yankol Y, Sanal T, Haholu A, Buyukdogan V, Ozdemir Y. Laparoscopic resection of a torsioned appendix epiploica in a previously appendectomized patient. Surg Laparosc Endosc Percutan Tech. 2005;15:371–3.
Romaniuk CS, Simpkins KC. Case report: pericolic abscess secondary to torsion of an appendix epiploica. Clin Radiol. 1993;47:216–7.
Bastidas JG, Danzy LE, Blackwell L, Bostick PJ, Hayden R. Epiploic appendagitis in a 24-year-old woman. Am J Emerg Med. 2008;26:838.e1-2.
Carmichael DH, Organ CH Jr. Epiploic disorders. Conditions of the epiploic appendages. Arch Surg. 1985;120:1167–72.
Sand M, Gelos M, Bechara FG, et al. Epiploic appendagitis—clinical characteristics of an uncommon surgical diagnosis. BMC Surg. 2007;7:11.
Vazquez-Frias JA, Castaneda P, Valencia S, Cueto J. Laparoscopic diagnosis and treatment of an acute epiploic appendagitis with torsion and necrosis causing an acute abdomen. JSLS. 2000;4:247–50.
Conflict of interest
JS, HAM, AME, FA, and SA all declare that they have no conflict of interest.
Ethical statement
The authors declare that the study was performed in a manner to conform with the Helsinki Declaration of 1975, as revised in 2000 and 2008 concerning Human and Animal Rights, and the authors followed the policy concerning Informed Consent as shown on Springer.com.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Saad, J., Mustafa, H.A., Elsani, A.M. et al. Primary epiploic appendagitis: Reconciling CT and clinical challenges. Indian J Gastroenterol 33, 420–426 (2014). https://doi.org/10.1007/s12664-014-0466-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12664-014-0466-y