
Abstract
Purpose
Patients undergoing lung resection are at increased risk for acute kidney injury (AKI) in the immediate postoperative period, with important consequences for longer term morbidity and mortality. Lung resection surgery has unique considerations that could increase the risk of AKI, including lung resection volume, duration of one-lung ventilation (OLV), and intraoperative fluid restriction. Yet, specific risk factor data are lacking. The objective of this study was to identify independent risk factors for early AKI after lung resection surgery.
Methods
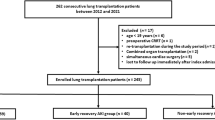
We conducted a retrospective case-control study of all patients presenting for elective lung resection surgery at an academic medical centre over a four-year period. Cases were patients who experienced an AKI and control patients were those who did not experience an AKI, based on KDIGO criteria. Baseline demographics and comorbidities along with duration of OLV and amount of lung resected were collected by retrospective chart review. The data were analyzed using multivariable logistic regression to identify independent predictors of AKI.
Results
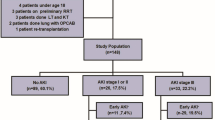
Acute kidney injury occurred within 48 hr in 57/1,045 (5.5%; 95% confidence interval, 4.2 to 7.0) of patients. On multivariable analysis, our model of best fit included preoperative serum creatinine, male sex, use of angiotensin II receptor blockers, and duration of OLV. The rate of complications, intensive care unit admission, and risk of death were all higher in the group of patients who experienced AKI.
Conclusions
Acute kidney injury occurs frequently after lung resection surgery and is associated with increased risk of postoperative complications. Increased duration of OLV may be a risk factor for AKI in this population.
Résumé
Objectif
Les patient·es bénéficiant d’une résection pulmonaire courent un risque accru d’insuffisance rénale aiguë (IRA) en période postopératoire immédiate, avec des conséquences importantes pour la morbidité et la mortalité à long terme. La chirurgie de résection pulmonaire entraîne des considérations uniques qui pourraient augmenter le risque d’IRA, notamment le volume de la résection pulmonaire, la durée de la ventilation unipulmonaire (VUP) et la restriction liquidienne peropératoire. Pourtant, les données spécifiques sur les facteurs de risque font défaut. L’objectif de cette étude était d’identifier les facteurs de risque indépendants d’IRA précoce après une chirurgie de résection pulmonaire.
Méthode
Nous avons mené une étude cas témoins rétrospective de toute la patientèle se présentant pour une chirurgie de résection pulmonaire non urgente dans un centre médical universitaire sur une période de quatre ans. Les cas étaient des patient·es qui ont présenté une IRA et des patient·es témoins qui n’ont pas eu d’IRA, selon les critères KDIGO. Les données démographiques et les comorbidités de base ainsi que la durée de la VUP et le volume de poumon réséqué ont été recueillis par examen rétrospectif des dossiers. Les données ont été analysées à l’aide d’une régression logistique multivariée afin d’identifier des prédicteurs indépendants d’IRA.
Résultats
Une insuffisance rénale aiguë est survenue dans les premières 48 heures postopératoires chez 57/1045 (5,5 %; intervalle de confiance à 95 %, 4,2 à 7,0) des patient·es. Sur l’analyse multivariée, notre modèle de meilleur ajustement incluait la créatininémie préopératoire, le sexe masculin, l’utilisation d’antagonistes des récepteurs de l’angiotensine II et la durée de la VUP. Le taux de complications, l’admission en unité de soins intensifs et le risque de décès étaient tous plus élevés dans le groupe de patient·es ayant présenté une IRA.
Conclusion
L’insuffisance rénale aiguë survient fréquemment après une chirurgie de résection pulmonaire et est associée à un risque accru de complications postopératoires. Une durée prolongée de VUP pourrait constituer un facteur de risque d’IRA dans cette population.


Similar content being viewed by others

References
Bihorac A, Yavas S, Subbiah S, et al. Long-term risk of mortality and acute kidney injury during hospitalization after major surgery. Ann Surg 2009; 249: 851–8. https://doi.org/10.1097/sla.0b013e3181a40a0b
Biteker M, Dayan A, Tekkeşin A, et al. Incidence, risk factors, and outcomes of perioperative acute kidney injury in noncardiac and nonvascular surgery. Am J Surg 2014; 207: 53–9. https://doi.org/10.1016/j.amjsurg.2013.04.006
Hobson C, Ozrazgat-Baslanti T, Kuxhausen A, et al. Cost and mortality associated with postoperative acute kidney injury. Ann Surg 2015; 261: 1207–14. https://doi.org/10.1097/sla.0000000000000732
Carmichael P, Carmichael AR. Acute renal failure in the surgical setting. ANZ J Surg 2003; 73: 144–53. https://doi.org/10.1046/j.1445-2197.2003.02640.x
Abelha FJ, Botelho M, Fernandes V, Barros H. Determinants of postoperative acute kidney injury. Crit Care 2009; 13: R79. https://doi.org/10.1186/cc7894
Kheterpal S, Tremper KK, Englesbe MJ, et al. Predictors of postoperative acute renal failure after noncardiac surgery in patients with previously normal renal function. Anesthesiology 2007; 107: 892–902. https://doi.org/10.1097/01.anes.0000290588.29668.38
Kheterpal S, Tremper KK, Heung M, et al. Development and validation of an acute kidney injury risk index for patients undergoing general surgery: results from a national data set. Anesthesiology 2009; 110: 505–15. https://doi.org/10.1097/aln.0b013e3181979440
Borthwick E, Ferguson A. Perioperative acute kidney injury: risk factors, recognition, management, and outcomes. BMJ 2010; 341: c3365. https://doi.org/10.1136/bmj.c3365
Yu Y, Xu S, Yan B, et al. Incidence and associations of acute kidney injury after general thoracic surgery: a system review and meta-analysis. J Clin Med 2022; 12: 37. https://doi.org/10.3390/jcm12010037
Amar D, Burt ME, Roistacher N, Reinsel RA, Ginsberg RJ, Wilson RS. Value of perioperative Doppler echocardiography in patients undergoing major lung resection. Ann Thorac Surg 1996; 61: 516–20. https://doi.org/10.1016/0003-4975(95)00939-6
Foroulis CN, Kotoulas CS, Kakouros S, et al. Study on the late effect of pneumonectomy on right heart pressures using Doppler echocardiography. Eur J Cardiothorac Surg 2004; 26: 508–14. https://doi.org/10.1016/j.ejcts.2004.05.036
Katz WE, Gasior TA, Quinlan JJ, et al. Immediate effects of lung transplantation on right ventricular morphology and function in patients with variable degrees of pulmonary hypertension. J Am Coll Cardiol 1996; 27: 384–91. https://doi.org/10.1016/0735-1097(95)00502-1
Kowalewski J, Brocki M, Dryjański T, Kaproń K, Barcikowski S. Right ventricular morphology and function after pulmonary resection. Eur J Cardiothorac Surg 1999; 15: 444–8. https://doi.org/10.1016/s1010-7940(99)00032-9
Pedoto A, Amar D. Right heart function in thoracic surgery: role of echocardiography. Curr Opin Anaesthesiol 2009; 22: 44–9. https://doi.org/10.1097/aco.0b013e32831d7b72
Smulders SA, Holverda S, Vonk-Noordegraaf A, et al. Cardiac function and position more than 5 years after pneumonectomy. Ann Thorac Surg 2007; 83: 1986-92.
Venuta F, Sciomer S, Andreetti C, et al. Long-term Doppler echocardiographic evaluation of the right heart after major lung resections. Eur J Cardiothorac Surg 2007; 32: 787–90. https://doi.org/10.1016/j.ejcts.2007.07.033
Lohser J, Slinger P. Lung injury after one-lung ventilation: a review of the pathophysiologic mechanisms affecting the ventilated and the collapsed lung. Anesth Analg 2015; 121: 302–18. https://doi.org/10.1213/ane.0000000000000808
Imai Y, Parodo J, Kajikawa O, et al. Injurious mechanical ventilation and end-organ epithelial cell apoptosis and organ dysfunction in an experimental model of acute respiratory distress syndrome. JAMA 2003; 289: 2104–12. https://doi.org/10.1001/jama.289.16.2104
Licker M, Cartier V, Robert J, et al. Risk factors of acute kidney injury according to RIFLE criteria after lung cancer surgery. Ann Thorac Surg 2011; 91: 844–50. https://doi.org/10.1016/j.athoracsur.2010.10.037
Ishikawa S, Griesdale DE, Lohser J. Acute kidney injury after lung resection surgery: incidence and perioperative risk factors. Anesth Analg 2012; 114: 1256–62. https://doi.org/10.1213/ane.0b013e31824e2d20
Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract 2012; 120: c179–84. https://doi.org/10.1159/000339789
Naruka V, McKie MA, Ahmadi N, Pama EAC, Coonar AS, Merits Collaborators. Multicentre evaluation of renal impairment in thoracic surgery (MERITS): a retrospective cohort study. BMJ Open 2022; 12: e058542. https://doi.org/10.1136/bmjopen-2021-058542
Arora P, Rajagopalam S, Ranjan R, et al. Preoperative use of angiotensin-converting enzyme inhibitors/angiotensin receptor blockers is associated with increased risk for acute kidney injury after cardiovascular surgery. Clin J Am Soc Nephrol 2008; 3: 1266–73. https://doi.org/10.2215/cjn.05271107
Author contributions
Ethan Bohn contributed to the conception and design of the study, preparation of the manuscript, and was responsible for the acquisition of data. Sadeesh Srinathan was responsible for study design and contributed to the interpretation of data and drafting the article. Joel Adu-Quaye contributed to the acquisition of data. Duane Funk contributed to all aspects of this manuscript, including conception and design; acquisition, analysis, and interpretation of data and drafting the article.
Disclosures
None.
Funding statement
Dr. Funk is funded by the Beckstead Anesthesiology Professorship.
Editorial responsibility
This submission was handled by Dr. Philip M. Jones, Deputy Editor-in-Chief, Canadian Journal of Anesthesia/Journal canadien d’anesthésie.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original article has been updated to correct the degree for co-author Joel Adu-Quaye.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Bohn, E., Srinathan, S., Adu-Quaye, J. et al. Predictors of acute kidney injury after lung resection surgery: a retrospective case-control study. Can J Anesth/J Can Anesth 70, 1901–1908 (2023). https://doi.org/10.1007/s12630-023-02602-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-023-02602-3