
Abstract
Purpose
We performed a systematic review and meta-analysis to determine the diagnostic test accuracy of ancillary investigations for declaration of death by neurologic criteria (DNC) in infants and children.
Source
We searched MEDLINE, EMBASE, Web of Science, and Cochrane databases from their inception to June 2021 for relevant randomized controlled trials, observational studies, and abstracts published in the last three years. We identified relevant studies using Preferred Reporting Items for Systematic Reviews and Meta-Analysis methodology and a two-stage review. We assessed the risk of bias using the QUADAS-2 tool, and applied Grading of Recommendations Assessment, Development, and Evaluation methodology to determine the certainty of evidence. A fixed-effects model was used to meta-analyze pooled sensitivity and specificity data for each ancillary investigation with at least two studies.
Principal findings
Thirty-nine eligible manuscripts assessing 18 unique ancillary investigations (n = 866) were identified. The sensitivity and specificity ranged from 0.00 to 1.00 and 0.50 to 1.00, respectively. The quality of evidence was low to very low for all ancillary investigations, with the exception of radionuclide dynamic flow studies for which it was graded as moderate. Radionuclide scintigraphy using the lipophilic radiopharmaceutical 99mTc-hexamethylpropyleneamine oxime (HMPAO) with or without tomographic imaging were the most accurate ancillary investigations with a combined sensitivity of 0.99 (95% highest density interval [HDI], 0.89 to 1.00) and specificity of 0.97 (95% HDI, 0.65 to 1.00).
Conclusion
The ancillary investigation for DNC in infants and children with the greatest accuracy appears to be radionuclide scintigraphy using HMPAO with or without tomographic imaging; however, the certainty of the evidence is low. Nonimaging modalities performed at the bedside require further investigation.
Study registration: PROSPERO (CRD42021278788); registered 16 October 2021.
Résumé
Objectif
Nous avons réalisé une revue systématique et une méta-analyse pour déterminer la précision des tests diagnostiques des examens auxiliaires pour la déclaration du décès selon des critères neurologiques (DCN) chez les nourrissons et les enfants.
Sources
Nous avons effectué des recherches dans les bases de données MEDLINE, EMBASE, Web of Science et Cochrane de leur création jusqu’en juin 2021 pour trouver des études randomisées contrôlées, des études observationnelles et des résumés pertinents publiés au cours des trois dernières années. Nous avons identifié les études pertinentes utilisant la méthodologie PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) et une revue en deux étapes. Nous avons évalué le risque de biais en utilisant l’outil QUADAS-2 et appliqué la méthodologie GRADE (Grading of Recommendations Assessment, Development and Evaluation) afin d’évaluer la certitude des données probantes. Un modèle à effets fixes a été utilisé pour méta-analyser les données de sensibilité et de spécificité regroupées pour chaque examen auxiliaire avec au moins deux études.
Constatations principales
Trente-neuf manuscrits admissibles évaluant 18 examens auxiliaires uniques (n = 866) ont été identifiés. La sensibilité et la spécificité variaient de 0,00 à 1,00 et de 0,50 à 1,00, respectivement. La qualité des données probantes était faible à très faible pour tous les examens auxiliaires, à l’exception des études de circulation nucléaire dynamique, pour lesquelles elle a été classée comme modérée. La scintigraphie nucléaire à l’aide du produit radiopharmaceutique lipophile 99mTc- hexa-méthyl-propylène amine oxime (HMPAO) avec ou sans imagerie tomographique était à la base des examens auxiliaires les plus précis, avec une sensibilité combinée de 0,99 (intervalle de densité le plus élevé [IDE] à 95 %, 0,89 à 1,00) et une spécificité de 0,97 (IDE à 95 %, 0,65 à 1,00).
Conclusion
L’examen auxiliaire pour un DCN chez les nourrissons et les enfants offrant la plus grande précision semble être la scintigraphie nucléaire utilisant le HMPAO avec ou sans imagerie tomographique; cependant, la certitude des données probantes est faible. Les modalités sans imagerie réalisées au chevet du patient nécessitent un examen plus approfondi.
Enregistrement de l’étude: PROSPERO (CRD42021278788); enregistrée le 16 octobre 2021.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Traditionally, death determination was based on cessation of cardiopulmonary function. Nevertheless, the advent of cardiopulmonary resuscitation and positive pressure mechanical ventilation in the mid-20th century challenged conventional definitions of death; an increasing number of patients with catastrophic brain injuries were manifesting with absent brainstem function on clinical examination. Death determination was decoupled from cardiopulmonary arrest in 1968 when the first standards for death by neurologic criteria (DNC) were outlined by a multidisciplinary committee at Harvard Medical School.1 Since then, clinical examination has prevailed as the gold standard for the determination of neurologic death across various jurisdictions.2,3,4
Clinical criteria for DNC have primacy in adult and pediatric patients in Canada. In 2006, the forum on Severe Brain Injury to Neurological Determination of Death published specific recommendations for ancillary testing in infants and children in situations where physicians are unable to complete the required clinical test.2 The clinical criteria for diagnosis include irreversible coma, absence of brainstem reflexes, and inability to breath spontaneously, which is formally evaluated by the apnea test, in the setting of severe neurologic injury. Prior to testing for DNC, providers must attempt to correct potential confounding conditions including hypothermia, hypotension, metabolic disturbances, and ensure systemic clearance of sedative medications that can interfere with clinical assessment.2, 5
Scenarios frequently arise where the clinical exam is either confounded by metabolic derangements, sedatives, or hypothermia. In other instances, physicians may be unable to complete the clinical examination because of anatomic derangements including perforated tympanic membranes, injury to the pupils, high cervical spine injuries, or severe lung disease preventing apnea testing. In such situations, ancillary investigations are required to augment the clinical examination and minimize the false-positive and false-negative determinations of DNC.2
While there are a multitude of potential ancillary investigations, all of them evaluate one of three surrogate physiologic processes that underscore the clinical examination: brain blood flow, brain perfusion, and/or brain function. These three distinct physiologic processes necessitate different types of ancillary investigations; imaging modalities are better suited to evaluate brain blood flow or brain perfusion, while electrophysiologic modalities evaluate brain function.6
While these physiologic processes remain proximal to the clinical examination, their diagnostic accuracy in determining DNC has not yet been quantified. There is an urgent need to consolidate the evidence base and derive estimates of how accurate ancillary investigations are for determining DNC. In doing so, we will be better positioned to inform the development of pediatric specific clinical practice guidelines on the optimal ancillary testing strategy.
In response to the heterogeneity in the choice and conduct of ancillary investigations in determining DNC,7, 8 we sought to perform a systematic review of the literature to determine the diagnostic accuracy of ancillary investigations for determination of DNC in infants and children.
Methods
This work was conducted as part of the “Brain-Based Definition of Death and Criteria for its Determination After Arrest of Circulation or Neurologic Function in Canada” project. We performed a systematic review following the Cochrane Handbook for Systematic Reviews of Diagnostic Test Accuracy and reported the findings in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines,9 including the PRISMA checklist (Electronic Supplementary Material [ESM] eAppendix 1), and the Cochrane Handbook for Systematic Reviews of Diagnostic Test Accuracy. The study protocol was registered with the International Prospective Register of Systematic Reviews registry (PROSPERO) prior to data extraction (CRD42021278788; registered 16 October 2021).
Search question, population, and inclusion and exclusion criteria
The primary objective of our review was to estimate the diagnostic test accuracy of ancillary investigations for DNC. The population of interest included all pediatric patients, defined as full-term infants (≥ 37 weeks gestational age) to children < 18 yr of age, who had either confirmed or suspected death as determined by clinical DNC. Children with confirmed DNC had a clinical assessment consistent with DNC prior to the ancillary investigation being performed. Children with suspected DNC had an exam concerning for DNC; however, formal testing was not undertaken prior to the ancillary investigations being performed. We did not prespecify any ancillary investigations as index tests, as we aimed to report on various potential ancillary investigations used in a pediatric cohort. An index test included any potential ancillary investigation evaluating brain blood flow, perfusion, or function that was performed in conjunction with or in addition to the clinical exam in patients with confirmed or suspected DNC. Furthermore, index tests could be administered either before or after the clinical assessment for DNC. In cases where an index test was administered multiple times to a patient, we used the results of the last index test performed. For the reference standard, we accepted the clinical assessment (either with or without an alternative ancillary investigation if the patient had any confounders) or four-vessel angiography as it has been previously recommended as a gold standard test in Canadian DNC guidelines.2 The clinical assessment included evaluation of brainstem function (absent pupillary, corneal, oculocephalic, and vestibulo–ocular reflexes, and absence of response to painful stimuli) and apnea test or absent respirations (for studies published prior to the implementation of the apnea test). In case series reporting on individual adult and pediatric data, we included pediatric data if there were two or more patients.
We excluded published editorials, letters, reviews, guidelines, scoping reviews, systematic reviews, meta-analyses, nonresearch articles, and abstracts published prior to 2018 but reviewed their bibliographies for additional eligible articles.
Search strategy
An information specialist (R. F.) modified a search that had been updated for a systematic review on ancillary investigations for adult DNC. The modified search was verified by content experts.10 The search in the original ancillary investigations systematic review was peer reviewed according to the PRESS Peer Review of Electronic Search Strategies 2015 Guideline Statement.11 We conducted a search of Ovid MEDLINE, Ovid Embase, the Cochrane Central Register of Controlled Trials (CENTRAL) via EBM Reviews (Ovid), and Web of Science (Science Citation) from inception until June 2021. Medical Subject Headings were used to identify synonyms. The MEDLINE search strategy appears in ESM eAppendix 2. Conference proceedings from the preceding three years (2018–2021) were retrieved by the Embase search and trial registry records from ClinicalTrials.gov and the World Health Organization’s International Clinical Trials Registry Platform were retrieved by the CENTRAL search. The reference lists of our full-text articles were searched for additional relevant articles. Filters were applied to limit results to references published in English or French.
Study selection
We used Covidence® software (Veritas Health Innovation Ltd., Melbourne, VIC, Australia) to screen articles in two stages. We screened titles and abstracts in the first stage followed by full-text articles in the second stage. For both stages, screening was conducted by two independent reviewers (N. M., J. K., M. S., J. G. B., O. M., L. H., L. W., C. M., J. B.). Disagreements were resolved by discussion or through arbitration by a third reviewer (J. B., N. M.).
Data extraction and summary measures
Groups of two independent reviewers (N. M., C. M./O. M., J. K./A. K., J. P./M. S., J. G. B.) extracted data through a standardized form. We collected author name, year of publication, country of origin, study design, total sample size, total number of pediatric patients, patient characteristics, presence of any confounders, data related to the flow, timing, and administration of the index test, and reference standard. We derived true positive, true-negative, false-positive, and false-negative values and summarized the data as sensitivity and specificity values for each ancillary investigation.
Statistical analysis
We analyzed studies that included patients with confirmed DNC separately from studies that included patients with suspected DNC. Additionally, we pooled and analyzed studies using the lipophilic radiopharmaceutical 99mTc-hexamethylpropyleneamine oxime (HMPAO) whether imaged by planar or single-photon emission computerized tomography (SPECT) techniques. We also pooled and analyzed all nuclear medicine imaging modalities with an initial dynamic flow phase (ESM eTable 1). We could only report pooled sensitivities for the studies that included patients with confirmed DNC because this study population did not contain false-positive cases from which to calculate specificity. For studies with suspected DNC, we reported both sensitivity and specificity. We estimated pooled sensitivities and specificities, when possible, for each ancillary investigation type with at least two studies. Pooled estimates for sensitivity were computed under the assumption that studies are exchangeable and sampled from the same binomial distribution with common sensitivity parameters. Similarly, for ancillary investigations with at least two studies with nonzero total negative cases, pooled estimates were also computed for specificity, under a similar assumption as for sensitivity. Estimates of pooled sensitivity and specificity were reported as posterior modes and 95% highest density intervals (HDI).12 For index tests with only one study, we generated 95% confidence intervals using Review Manager (RevMan, London, UK). All computations were carried out using R (R Foundation for Statistical Computing, Vienna, Austria) and Stan statistical software (Stan Development Team, New York, NY, USA).13, 14
Rating the certainty of evidence
We evaluated the certainty of the evidence using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework.15 In keeping with the GRADE framework, studies started as high-certainty evidence. We downgraded certainty based on limitations in risk of bias, inconsistency, indirectness, and imprecision (ESM eTable 1). The risk of bias was assessed at both the study and outcome levels using the Quality Assessment Tool for Diagnostic Accuracy Studies-2 (QUADAS-2) tool.16 To evaluate imprecision, we used pooled sensitivity and specificity values and their respective confidence intervals to estimate the absolute number of true-positive, false-positive, true-negative, and false-negative cases per 1,000 people at prevalence levels of 50, 90, and 95%.
Results
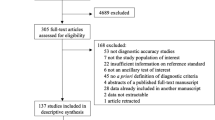
We found 39 studies that met the inclusion criteria, published between 1971 and 2017 (Figure 1; Table 1). Of these, we meta-analyzed the data from 38 studies and narratively reported the outcomes of one study given we were unable to extract patient characteristics for the index test.17 Thirty-six studies were cohort studies and three were case-controlled designs. Eighteen different ancillary investigations for DNC were evaluated across the included studies, with a total of 55 comparative evaluations of the index tests across the 38 manuscripts (Table 1). Of the 18 different ancillary investigations, eight were evaluated in only a single study (Table 1).18,19,20,21,22,23,24,25

PRISMA flow diagram. Details of the citation search and screening process in this systematic review
Eighteen studies included patients who met clinical exam criteria for DNC and 18 studies included patients who were suspected of DNC but had not undergone formal testing. The case–control studies (n = 3, 7.7%) included pediatric patients who were confirmed to have met DNC.26,27,28 All studies included a clinical exam or a clinical exam and an ancillary investigation as the gold standard. One study did not define the criteria for a clinical exam consistent with DNC; however, the clinical exam was combined with four-vessel cerebral angiography for all pediatric patients and as such was determined to meet criteria to be included as a reference standard.29
Imaging-based ancillary investigations (Tables 2 and 3)
Accuracy of radionuclide dynamic flow imaging
Thirteen studies (n = 249) used radiopharmaceutical-based flow imaging to determine DNC. Of those, 12 studies used a lipophobic radiopharmaceutical—five with 99mTc-diethylenetriaminepentaacetic acid (DTPA),23, 29,30,31,32 four with 99mTc-pertechnetate,22, 33,34,35 one with 99mTc-glucoheptonate (GHA),23 two with unspecified radiopharmaceuticals36, 37—and one study reported the initial flow phase of a 99mTc-labeled lipophilic radiopharmaceutical in sufficient detail to be included38 (ESM eTable 2). We included one study that used 99mTc-pertechnetate and a bedside triple probe scintillation counting system to assess the presence or absence of cerebral blood flow. This is not a conventional nuclear medicine scan; however, it used a lipophobic radiopharmaceutical and assessed cerebral blood flow, so we included it in our analysis.34 We meta-analyzed these studies together based on the identical functional properties of the radiopharmaceuticals used. In eight studies that enrolled patients suspected of DNC (n = 116),22, 24, 29, 31, 34, 35, 37, 38 radionuclide flow imaging had a sensitivity of 0.95 (95% HDI, 0.89 to 0.98) and a specificity of 0.88 (95% HDI, 0.67 to 0.98). The certainty of evidence was downgraded to moderate for both sensitivity and specificity because of serious risk of bias (ESM eTable 3).
99mTc-diethylenetriaminepentaacetic acid (DTPA)
Five studies (n = 100) assessed cerebral blood flow using 99mTc-DTPA23, 29,30,31,32; and two studies (n = 7)29, 31 reported diagnostic accuracy outcomes in patients with suspected DNC. In the first study,29 the two patients with suspected DNC had no detectable flow in their craniums. In the second study, Erbengi et al. (1990)31 included five pediatric patients suspected of DNC. The absence of intracranial arterial flow and absence of sagittal sinus activity on dynamic and static images were the criteria set for a test to be consistent with DNC. Of the five pediatric patients, three had absent flow and no uptake on static blood pool images, consistent with DNC. One patient had flow present, and another had no flow present but sagittal sinus activity on static images not consistent with DNC per the author’s criteria. In patients with suspected DNC, 99mTc-DTPA had a sensitivity of 0.87 (95% HDI, 0.53 to 0.99). The certainty of evidence is very low because of serious risk of bias, indirectness, and imprecision.
Of the three studies involving patients with confirmed DNC, Erbengi et al. (1991)30 included only one pediatric participant in whom both the dynamic and static images showed an absence of cerebral circulation. In Schober et al. (1987),23 two patients showed no flow, consistent with DNC. In the third study, no cerebral blood flow was detected in 83 patients with confirmed DNC, whereas persistent intracranial blood flow was present in seven patients.32 Pooled analysis for these three studies showed a sensitivity of 0.92 (95% HDI, 0.86 to 0.97). The certainty of evidence was very low because of serious risk of bias, indirectness, and imprecision.
99mTc-pertechnetate
Four studies enrolling 49 patients assessed cerebral blood flow using 99mTc-pertechnetate.22, 33,34,35 Of those, 30 patients in three studies were suspected of DNC while 19 patients22, 34, 35 in one study were confirmed to be DNC.33 In patients with suspected DNC, 99mTc-pertechnetate showed a sensitivity of 0.91 (95% HDI, 0.77 to 0.99) and a specificity of 0.97 (95% HDI, 0.65 to 1.00). The certainty of the evidence for both sensitivity and specificity was downgraded to low because of high risk of bias and imprecision.
Ashwal et al. (1977)34 used 99mTc-pertechnetate and a bedside triple probe scintillation counting system to assess the presence or absence of cerebral blood flow. Nine patients with a clinical exam concerning for DNC had no cranial isotope bolus detected in the presence of a systemic bolus. Three children who did not meet DNC criteria had detectable flow, showed by a positive cranial and systemic isotope bolus.
Schwartz et al. (1984)22 reported on nine children with suspected DNC. None of the nine children had arterial flow detected after systemic isotope injection; however, activity was detected in the sagittal sinus, which they discounted as insignificant (n = 3). In a study by Thompson et al. (1986)35 that used dynamic brain scintigraphy, flow was graded from 0 to +4, with 0 reflecting no cerebral activity and absent or minimal but delayed sinus activity to +4 representing peak cerebral activity to sagittal sinus in less than six seconds. A study with a scintigraphy grade of 0 meets DNC criteria. The study results included three patients without cerebral activity (grade flow of 0) and clinical assessments consistent with DNC, four patients with graded flow of +3 and +4 and a clinical assessment inconsistent with DNC, and two patients with graded flow of +1 and +3 but meeting clinical assessment criteria for DNC; both of these infants survived.
Flowers et al. (2000)33 was the only study to include patients with a confirmed diagnosis of DNC. They defined a study with the absence of arterial flow in the cerebral circulation as consistent with DNC. No arterial flow was detected in the 19 patients studied; however, one patient did have evidence of radiopharmaceutical detected in the superior sagittal sinus, which the authors state was likely to have been due to flow from extradural perforating arteries originating from the external carotid circulation,37 and as such was discounted as not indicative of brain viability or cortical flow. The sensitivity for this study was 1.0.
Accuracy of radionuclide parenchymal uptake studies
Ten studies used lipophilic radiopharmaceuticals, one (n = 14) using N-isopropyl-p-[123I]iodoamphetamine (123I-IMP)23 and nine (n = 84) using 99mTc-HMPAO.23, 30, 31, 38,39,40,41,42,43 Of the nine 99mTc-radiopharmaceutical studies, five used planar imaging23, 38, 41,42,43 and four SPECT imaging.23, 38, 41,42,43 We combined the parenchymal uptake studies using 99mTc-HMPAO. The pooled sensitivity and specificity were 0.99 (95% HDI, 0.89 to 1.00) and 0.97 (95% HDI, 0.65 to 1.00), respectively. The certainty of the evidence for both sensitivity and specificity was downgraded to low because of high risk of bias and imprecision.
99mTc-hexamethylpropyleneamine oxime (HMPAO) (planar imaging)
Five studies (n = 65) reported on the diagnostic accuracy of 99mTc-HMPAO with planar imaging.23, 38, 41,42,43 Of those, two studies included patients with confirmed DNC by clinical exam23, 41 and three studies included patients with suspected DNC.38, 42, 43 Parker et al. (1995)41 included 13 patients in whom clinical criteria for DNC could not be completed. None of these patients showed parenchymal uptake. Laurin et al. (1989)38 described a mixed cohort of both children and adults suspected of meeting DNC. The authors noted that nine of 25 patients with no arterial flow did have 99mTc-HMPAO uptake into the dural venous sinus, which they discounted as not contradicting the diagnosis of DNC. The authors did not stratify this finding by age; therefore, it is unclear if any of the pediatric patients (n = 9) without arterial flow had blood pool noted in their dural venous sinuses. The sensitivity and specificity of 99mTc-HMPAO was 0.99 (95% HDI, 0.87 to 1.00) and 0.97 (95% HDI, 0.65 to 1.00), respectively. The certainty of evidence for both sensitivity and specificity was deemed to be low because of serious risk of bias, imprecision, and heterogeneity.
99mTc-hexamethylpropyleneamine oxime (HMPAO) (SPECT imaging)
Four studies (n = 19) used 99mTc-HMPAO with SPECT imaging.30, 31, 39, 40 One study investigated patients with suspected DNC31, while three studies reported the diagnostic accuracy in patients with confirmed DNC. All studies defined a scan consistent with DNC as the absence of parenchymal uptake in both the cerebral hemispheres and cerebellum on the tomographic images. None of the 19 patients had parenchymal uptake in either their cerebral hemispheres or cerebellum. In patients with suspected DNC (n = 4), sensitivity of 99mTc-HMPAO SPECT was 1.00 (95% CI, 0.40 to 1.00). Specificity could not be determined because no patients who had absent flow were deemed to be alive. Certainty of evidence for sensitivity is very low because of serious risk of bias and very serious concerns of imprecision.
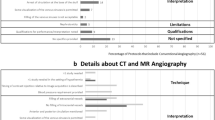
Accuracy of computed tomography (CT) angiography
Only one study (n = 19) reported on the diagnostic accuracy of CT angiography.21 The estimated sensitivity was 1.00 (95% CI, 0.82 to 1.00). The certainty of this evidence was very low because of high risk of bias, indirectness, and imprecision.
Accuracy of four-vessel cerebral angiography
Only one study (n = 9) investigated four-vessel cerebral angiography as the ancillary investigation in children (n = 9) with clinical exams suggestive of DNC.22 In their study, all children had absent cerebral arterial filling and met criteria for DNC. The sensitivity of four-vessel cerebral angiography was 1.00 (95% CI, 0.66 to 1.00). The certainty of this evidence was low because of serious risk of bias, indirectness, and imprecision. A second study had 28 patients who underwent either four-vessel cerebral angiography or an unspecified radionuclide scan following clinical exam consistent with DNC.44 No cerebral blood flow was present for any patients with suspected DNC (n = 28); however, given the investigations were not stratified per patient, we were unable to use the data in the four-vessel cerebral angiography analysis. Unfortunately, no pediatric or adult studies included patients without DNC, so no data exist from which to calculate specificity.
Accuracy of transcranial Doppler (TCD)
We identified seven studies27, 45,46,47,48,49,50 (n = 149) that reported on the use of TCD in determination of DNC. Three studies defined a priori the waveforms that were consistent with DNC,47, 49, 50 with two of these studies further clarifying the required waveforms to be present bilaterally for the investigation to be consistent with DNC.47, 50 One study did not define transcranial waveforms consistent with DNC, but stated that “cerebral circulatory arrest” is consistent with DNC.48 The remaining studies described waveforms in patients with exams suspicious for DNC but did not a priori define the criteria for a TCD consistent with DNC.27, 45, 46 In patients with suspected DNC (four studies, n = 79 patients), the sensitivity and specificity were 0.91 (95% HDI, 0.77 to 0.98) and 0.88 (95% HDI, 0.77 to 0.95), respectively. The certainty of the evidence was very low for both sensitivity and specificity because of serious risk of bias, indirectness, and imprecision.
Nonimaging-based ancillary investigations (Tables 2 and 3)
Accuracy of electroencephalography (EEG)
We identified 13 studies (n = 299) that evaluated EEG as an ancillary investigation for DNC.20, 24, 26, 32, 34,35,36, 40, 41, 44, 51,52,53 Thirteen patients studied had known confounders including detectable phenobarbital levels (n = 11),34, 41, 44 or hypothermia and a detectable phenobarbital level (n = 2)35 at the time of EEG. Typical studies defined an EEG with electrocerebral silence as consistent with DNC, one stated an isoelectric EEG was consistent and another defined a “flat” EEG as consistent with DNC.40 Seven studies included patients with confirmed DNC.32, 36, 40, 41, 44, 52, 53 In patients with suspected DNC, pooled analysis showed a sensitivity of 0.88 (95% HDI, 0.78 to 0.96) and a specificity of 0.96 (95% HDI, 0.82 to 1.00). The certainty of evidence is very low for both sensitivity and specificity because of serious risk of bias, indirectness, and imprecision (ESM eTable 4).
Accuracy of brain auditory evoked potentials (BAEPs)
A total of three studies (n = 31)28, 30, 52 reported on the diagnostic accuracy of BAEPs as determining DNC. Only one study a priori defined a BAEP consistent with DNC, stating that a recording with no response in the C2 to A1/A2 electrode30 was consistent with DNC, whereas the other studies were descriptive.28, 52 Typical patients did not have confounders.28, 30 In the one study (n = 23) of patients with suspected DNC, the sensitivity and specificity were 0.90 (95% CI, 0.55 to 1.00) and 1.00 (95% CI, 0.75 to 1.00), respectively. The certainty of the evidence was very low for both sensitivity and specificity because of serious risk of bias, indirectness, and imprecision.
Accuracy of brain auditory evoked potentials and somatosensory evoked potentials (SSEPs)
Two studies (n = 158) evaluated the accuracy of BAEPs and SSEPs in patients with confirmed DNC.32, 54 Confounding variables such as barbiturate coma or hypothermia were not described in any patients. Ruiz-García et al. (2000)32 defined an investigation consistent with DNC as no observable waveforms for both brainstem and somatosensory evoked potentials. Ruiz-López et al. (1999)54 did not explicitly define the methodology waveforms consistent with DNC and instead described waveforms in the patient population. Pooled sensitivity for the two studies was 0.92 (95% HDI, 0.87 to 0.96). The certainty of the evidence was very low because of serious risk of bias, indirectness, and imprecision.
Discussion
Ancillary investigations are essential for DNC when the clinical assessment cannot be completed in its entirety. Nevertheless, the wide variety of available ancillary investigations and uncertainty around their diagnostic accuracy creates a challenge for patient families, clinicians, and organ donation organizations when DNC is being considered. This systematic review and meta-analysis consolidates the literature to date on the diagnostic accuracy of ancillary investigations in infants and children with suspected or confirmed DNC. We identified 39 manuscripts reporting on 18 different ancillary investigations in 866 infants and children. Of all ancillary investigations examined, the radionuclide studies, including pooled lipophobic radiopharmaceuticals and pooled lipophilic radiopharmaceuticals, showed the highest sensitivities and specificities.
The World Brain Death Project recommends the use of radionuclide angiography as the preferred ancillary investigation for DNC in infants and children.3 Despite high diagnostic accuracy, the certainty of evidence is moderate for studies based on lipophobic flow and low for studies based on lipophilic parenchymal uptake. Certainty in diagnostic accuracy estimates could be further improved by refining the criteria for DNC. For example, in one study, activity in the superior sagittal sinus was defined as not consistent with DNC.31 Superior sagittal sinus activity is believed to be due to flow from extradural perforating arteries originating from the external carotid circulation and has been shown to occur not infrequently in children meeting DNC criteria.37 A final caveat in the analysis of lipophilic radiopharmaceuticals is that only studies that used 99mTc-HMPAO have been evaluated; a second lipophilic radiopharmaceutical in common use today, 99mTc-bicisate, may be similar but has not been rigorously evaluated.
Estimates of the diagnostic accuracy of all ancillary investigations were limited by low certainty of evidence due to risk of bias, indirectness, imprecision, and heterogeneity. For the other imaging modalities, we could not derive specificity data for CT angiography and four-vessel cerebral angiography. Extrapolation of CT angiography from adult studies is severely limited by the anatomical and physiologic differences of infants and young children for several reasons. First, newer multiphase CT angiography, an increasingly common ancillary investigations in adults, requires a dose of radiation that would be uncharacteristically high for infants and young children. Furthermore, their smaller veins limit the contrast injection rates required to perform these studies. Two-phase spiral CT has been shown in a small international study to be an ancillary investigation for DNC in smaller children, details on the protocol used or vessels evaluated preclude its generalizability.17 Future studies investigating CT angiography would benefit from clearly defining if 4, 7, or 10 vessels were evaluated, and should include vessels in both the supratentorial and infratentorial regions of the brain to evaluate blood flow to the cortex and the brainstem.
Transcranial Doppler is a potentially promising ancillary investigation for determination of DNC since it can be performed at the bedside without the need for patient transport. Nevertheless, the findings of our review suggest that TCDs are more specific than they are sensitive. Few studies reported the diagnostic criteria for TCDs with respect to the vessels that were evaluated, the cut-offs for Doppler waveforms, and whether TCDs were done bilaterally or unilaterally. Standardizing TCD criteria for DNC in pediatric patients as well as the inclusion of both the anterior and posterior cerebral circulation could minimize false negatives and improve sensitivity measures. Future implementation of TCD as an ancillary investigation for pediatric DNC would require additional resources and education of pediatric sonographers, given that currently, TCDs are not performed regularly at all pediatric institutions. Nevertheless, prior to this, we require additional studies to improve the certainty in the diagnostic accuracy of TCDs, and to better delineate the diagnostic thresholds for the determination of DNC.
Electroencephalography is another promising ancillary investigation that has been used for determination of DNC. Although the sensitivity and specificity of EEGs in our review were 88% and 96%, respectively, our findings are limited by low certainty evidence. Very few studies we identified included patients with confounders that could meaningfully alter the diagnostic accuracy of EEGs. As a result, there is uncertainty in how EEGs would perform if used on patients who have been heavily sedated or those with uncorrectable hypothermia. Future studies are needed to validate the diagnostic accuracy of EEGs in the context of clinical confounders.
In terms of strengths, this systematic review and meta-analysis was conducted using established systematic review methodology and is the largest and most inclusive evaluation of ancillary investigations for DNC in infants and children. We registered the systematic review protocol prior to the initiation of the review and employed a search strategy that did not restrict studies by publication type. We employed a two-step review process for both title and abstract screening as well as full-text review to minimize bias due to selective reporting.
Our review also has important limitations. The originally planned analyses were to use (1) multi-level models to estimate partially pooled sensitivities; and (2) hierarchical summary receiver operating characteristic curve models to estimate partially pooled sensitivities and specificities, in both cases per type of ancillary investigation and per study nested within each ancillary investigation type. Unfortunately, these analyses were not feasible because of the limited number of studies per ancillary investigation, the relatively small sample sizes of most of the studies, and missing data from within the studies. Because of all these shortcomings, our analysis used fixed-effect models and pooled sensitivity and specificity independently of one another, and as such our estimates do not account for between-study heterogeneity nor the inherent trade-off between sensitivity and specificity. This is a limitation to keep in mind when interpreting the results. Other limitations include the exclusion of studies published in languages other than English and French, omission of the gray literature, and the exclusion of abstracts published prior to 2018.
Conclusion
Our systematic review suggests that flow-based nuclear medicine imaging modalities are the most accurate ancillary investigations for DNC in infants and children—more specifically, radionuclide scintigraphy using 99mTc-HMPAO, combined with planar or SPECT imaging (low certainty of evidence). This lipophilic radiopharmaceutical incorporates both a parenchymal and a flow phase. Further studies are required to refine our diagnostic accuracy estimates and certainty of the evidence in more readily available and bedside ancillary investigations such as EEGs and TCDs.
References
Beecher HK. A definition of irreversible coma: report of the ad hoc Committee of the Harvard Medical School to examine the definition of brain death. JAMA 1968; 205: 337–40.
Shemie SD, Doig C, Dickens B, et al. Severe brain injury to neurological determination of death: Canadian forum recommendations. CMAJ 2006; 174: S1–12. https://doi.org/10.1503/cmaj.045142
Greer DM, Shemie SD, Lewis A, et al. Determination of brain death/death by neurologic criteria: the World Brain Death Project. JAMA 2020; 324: 1078–97. https://doi.org/10.1001/jama.2020.11586
Nakagawa TA, Ashwal S, Mathur M, et al. Guidelines for the determination of brain death in infants and children: an update of the 1987 Task Force recommendations. Crit Care Med 2011; 39: 2139–55. https://doi.org/10.1097/ccm.0b013e31821f0d4f
Kanji S, Williamson D, Hartwick M .Potential pharmacological confounders in the setting of death determined by neurologic criteria: a narrative review. Can J Anesth 2023; https://doi.org/10.1007/s12630-023-02415-4
Plourde G, Briard JN, Shemie SD, Shankar JJS, Chassé M. Flow is not perfusion, and perfusion is not function: ancillary testing for the diagnosis of brain death. Can J Anesth 2021; 68: 953–61. https://doi.org/10.1007/s12630-021-01988-2
Lewis A, Liebman J, Kreiger-Benson E, et al. Ancillary testing for determination of death by neurologic criteria around the world. Neurocrit Care 2021; 34: 473–84. https://doi.org/10.1007/s12028-020-01039-6
Lewis A, Bakkar A, Kreiger-Benson E, et al. Determination of death by neurologic criteria around the world. Neurology 2020; 95: e299–309. https://doi.org/10.1212/wnl.0000000000009888
Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021; 372: n71. https://doi.org/10.1136/bmj.n71
Chassé M, Glen P, Doyle MA, et al. Ancillary testing for diagnosis of brain death: a protocol for a systematic review and meta-analysis. Syst Rev 2013; 2: 100. https://doi.org/10.1186/2046-4053-2-100
McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS peer review of electronic search strategies: 2015 guideline statement. J Clin Epidemiol 2016; 75: 40–6. https://doi.org/10.1016/j.jclinepi.2016.01.021
Kruschke JK. Doing Bayesian Data Analysis: A Tutorial with R, JAGS and Stan, 2nd edition. London: Elsevier; 2014.
R Core Team (2021). R: a language and environment for statistical computing. Available from URL: https://www.R-project.org/ (accessed December 2022).
Stan Development Team. Stan modeling language users guide and reference manual. Available from URL: https://mc-stan.org (accessed December 2022).
Guyatt G, Oxman AD, Akl EA, et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J Clin Epidemiol 2011; 64: 383–94. https://doi.org/10.1016/j.jclinepi.2010.04.026
Whiting PF, Rutjes AW, Westwood ME, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med 2011; 155: 529–36. https://doi.org/10.7326/0003-4819-155-8-201110180-00009
Hindy-François C, Orliaguet G, Meyer P, et al. Pediatric brain death diagnosis in the view of organ donation in France. Transplantation 2009; 87: 616–7. https://doi.org/10.1097/tp.0b013e3181963d91
Riggs BJ, Cohen JS, Shivakumar B, et al. Doppler ultrasonography of the central retinal vessels in children with brain death. Pediatr Crit Care Med 2017; 18: 258–64. https://doi.org/10.1097/pcc.0000000000001087
Okuyaz Ç, Birbiçer H, Doruk N, Atici A. Bispectral index monitoring in confirmation of brain death in children. J Child Neurol 2006; 21: 799–801. https://doi.org/10.1177/08830738060210090101
Furgiele TL, Frank LM, Riegle C, Wirth F, Earley LC. Prediction of cerebral death by cranial sector scan. Crit Care Med 1984; 12: 1–3. https://doi.org/10.1097/00003246-198401000-00001
Duyu M, Karakaya Z. Evaluation of patients diagnosed with brain death in paediatric critical care. J Pediatric Res 2020; 7: 250–6. https://doi.org/10.4274/jpr.galenos.2020.82474
Schwartz JA, Baxter J, Brill DR. Diagnosis of brain death in children by radionuclide cerebral imaging. Pediatrics 1984; 73: 14–8.
Schober O, Galaske R, Heyer R. Determination of brain death with 123I-IMP and 99mTc-HM-PAO. Neurosurg Rev 1987; 10: 19–22. https://doi.org/10.1007/BF01780588
Holzman BH, Curless RG, Sfakianakis GN, Ajmone-Marsan C, Montes JE. Radionuclide cerebral perfusion scintigraphy in determination of brain death in children. Neurology 1983; 33: 1027–31. https://doi.org/10.1212/wnl.33.8.1027
Jalili M, Crade M, Davis AL. Carotid blood-flow velocity changes detected by Doppler ultrasound in determination of brain death in children. Clin Pediatr 1994; 33: 669–74. https://doi.org/10.1177/000992289403301106
Ashwal S, Schneider S, Thompson J. Xenon computed tomography measuring cerebral blood flow in the determination of brain death in children. Ann Neurol 1989; 25: 539–46. https://doi.org/10.1002/ana.410250603
Rodriguez RA, Cornel G, Alghofaili F, Hutchison J, Nathan HJ. Transcranial Doppler during suspected brain death in children: potential limitation in patients with cardiac “shunt.” Pediatr Crit Care Med 2002; 3: 153–7. https://doi.org/10.1097/00130478-200204000-00012
Steinhart CM, Weiss IP. Use of brainstem auditory evoked potentials in pediatric brain death. Crit Care Med 1985; 13: 560–2. https://doi.org/10.1097/00003246-198507000-00010
Tribolet N de, Schäfer K, Oberson R, Zander E. Radioisotope diagnosis of brain death [French]. Schweiz Med Wochenschr 1977; 107: 464–7.
Erbengi A, Erbengi G, Cataltepe O, Topcu M, Erbas B, Aras T. Brain death: determination with brain stem evoked potentials and radionuclide isotope studies. Acta Neurochir 1991; 112: 118–25. https://doi.org/10.1007/bf01405139
Erbengi G, Erbengi A, Erbas B, Aras T. Diagnosis of brain death using TC-99m-HMPAO/SPECT, Tc-99m-DTPA scintigraphy and radionuclide angiography. NucCompact 1990; 21: 177–9.
Ruiz-García M, Gonzalez-Astiazarán A, Collado-Corona MA, Rueda-Franco F, Sosa-de-Martínez C. Brain death in children: clinical, neurophysiological and radioisotopic angiography findings in 125 patients. Childs Nerv Syst 2000; 16: 40–5. https://doi.org/10.1007/s003810050010
Flowers WM Jr, Patel BR. Accuracy of clinical evaluation in the determination of brain death. South J Med 2000; 93: 203–6.
Ashwal S, Smith AJ, Torres F, Loken M, Chou SN. Radionuclide bolus angiography: A technique for verification of brain death in infants and children. J Pediatr 1977; 91: 722–7. https://doi.org/10.1016/s0022-3476(77)81023-8
Thompson JR, Ashwal S, Schneider S, Hasso AN, Hinshaw DB, Kirk G. Comparison of cerebral blood flow measurements by xenon computed tomography and dynamic brain scintigraphy in clinically brain dead children. Acta Radiologica Suppl 1986; 369: 675–9.
Ashwal S. Brain death in early infancy. J Heart Lung Transplant 1993; 12: S176–8.
Coker SB, Dillehay GL. Radionuclide cerebral imaging for confirmation of brain death in children: the significance of dural sinus activity. Pediatr Neurol 1986; 2: 43–6. https://doi.org/10.1016/0887-8994(86)90039-1
Laurin NR, Driedger AA, Hurwitz GA, et al. Cerebral perfusion imaging with technetium-99m HM-PAO in brain death and severe central nervous system injury. J Nucl Med 1989; 30: 1627–35.
Kahveci F, Bekar A, Tamgac F. Tc-99 HMPAO cerebral SPECT imaging in brain death patients with complex spinal automatism. Ulus Travma Derg 2002; 8: 198–201.
Okuyaz Ç, Gücüyener K, Karabacak Nİ, Aydin K, Serdaroğlu A, Cingi E. Tc‐99m‐HMPAO SPECT in the diagnosis of brain death in children. Pediatr Int 2004; 46: 711–4. https://doi.org/10.1111/j.1442-200x.2004.01976.x
Parker BL, Frewen TC, Levin SD, et al. Declaring pediatric brain death: current practice in a Canadian pediatric critical care unit. CMAJ 1995; 153: 909–16.
Kraft O, Samlík J, Chmelová J. The diagnosis of brain death—own experience. Nucl Med Rev Cent East Eur 2006; 9: 132–7.
Wilson K, Gordon L, Selby JB Sr. The diagnosis of brain death with Tc-99m HMPAO. Clin Nucl Med 1993; 18: 428–34. https://doi.org/10.1097/00003072-199305000-00013
Fackler JC, Troncoso JC, Gioia FR. Age-specific characteristics of brain death in children. Am J Dis Child 1988; 142: 999–1003. https://doi.org/10.1001/archpedi.1988.02150090097034
Powers AD, Graeber MC, Smith RR. Transcranial Doppler ultrasonography in the determination of brain death. Neurosurgery 1989; 24: 884–9. https://doi.org/10.1227/00006123-198906000-00015
Qian SY, Fan XM, Yin HH. Transcranial Doppler assessment of brain death in children. Singap Med J 1998; 39: 247–50.
Bode H, Sauer M, Pringsheim W. Diagnosis of brain death by transcranial Doppler sonography. Arch Dis Child 1988; 63: 1474–8. https://doi.org/10.1136/adc.63.12.1474
Blanot S, Montmayeur J, Salvadori A, Ottonello G, Orliaguet G. Évaluation rétrospective de l’épreuve d’apnée chez l’enfant en mort encéphalique. Méd Intensive Réa 2016; 25: 171–8. https://doi.org/10.1007/s13546-016-1222-3
Newell DW, Grady SM, Sirotta P, Winn RH. Evaluation of brain death using transcranial Doppler. Neurosurgery 1989; 24: 509–13. https://doi.org/10.1227/00006123-198904000-00004
Gencpinar P, Dursun O, Teküc H, Ünal A, Haspolat Ş, Duman Ö. Pediatric brain death: experience of a single center. Turkiye Klinikleri J Medical Sci 2015; 35: 60–6.
Ashwal S, Schneider S. Failure of electroencephalography to diagnose brain death in comatose children. Ann Neurol 1979; 6: 512–7. https://doi.org/10.1002/ana.410060609
Goh A, Mok Q. Clinical course and determination of brainstem death in a children’s hospital. Acta Paediatr 2004; 93: 47–52. https://doi.org/10.1111/j.1651-2227.2004.tb00673.x
Mohandas A, Chou SN. Brain death: a clinical and pathological study. J Neurosurg 1971; 35: 211–8. https://doi.org/10.3171/jns.1971.35.2.0211
Ruiz-López MJ, de Azagra AM, Serrano A, Casado-Flores J. Brain death and evoked potentials in pediatric patients. Crit Care Med 1999; 27: 412–6. https://doi.org/10.1097/00003246-199902000-00051
Author contributions
Nicole K. McKinnon, Lionel S. Zuckier, J. Gordon Boyd, Michaël Chassé, Andreas Kramer, Julie Kromm, Owen Mooney, Marat Slessarev, and John Basmaji designed the study. Nicole K. McKinnon, Julie Kromm, Marat Slessarev, J. Gordon Boyd, Owen Mooney, Laura Hornby, Christina Maratta, and John Basmaji assessed citations for eligibility. Nicole K. McKinnon, Christina Maratta, Owen Mooney, Julie Kromm, Andreas Kramer, Jaewoo Park, Marat Slessarev, J. Gordon Boyd, and John Basmaji abstracted data. Nicole K. McKinnon, Christina Maratta, Owen Mooney, Julie Kromm, Andreas Kramer, Jaewoo Park, Marat Slessarev, J. Gordon Boyd, and John Basmaji assessed risk of bias, and Nicole K. McKinnon, Christina Maratta, Lionel S. Zuckier, Prakash Muthusami, and John Basmaji checked data for accuracy. Nicole K. McKinnon, Lionel S. Zuckier, Prakash Muthusami, Roy Nitulescu, Michaël Chassé, and John Basmaji conducted analyses. All authors contributed to interpret the data. All authors read the manuscript and provided feedback.
Acknowledgements
The authors would like to express their appreciation to Robin Featherstone, MLIS, and Daniela Ziegler, MSI, for modifying our search strategy. Additionally, the authors would like to thank Lindsay C. Wilson, MHA, and Sam D. Shemie, MD, for their leadership, support, and coordination.
Disclosures
Laura Hornby is a paid consultant for Canadian Blood Services.
Funding statement
This work was conducted as part of the project entitled, “A Brain-Based Definition of Death and Criteria for its Determination After Arrest of Circulation or Neurologic Function in Canada,” made possible through a financial contribution from Health Canada through the Organ Donation and Transplantation Collaborative and developed in collaboration with the Canadian Critical Care Society, Canadian Blood Services, and the Canadian Medical Association. The views expressed herein do not necessarily represent the views of Health Canada, the Canadian Critical Care Society, Canadian Blood Services, or the Canadian Medical Association.
Prior conference presentations
These findings have been presented at The Canadian Association of Nuclear Medicine Annual Conference in Montreal, QC on 30 September 2022 and the Critical Care Canada Forum meeting in Toronto, ON on 24 November 2022.
Editorial responsibility
This submission was handled by Dr. Maureen Meade, Guest Editor, Canadian Journal of Anesthesia/Journal canadien d’anesthésie.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
McKinnon, N.K., Maratta, C., Zuckier, L.S. et al. Ancillary investigations for death determination in infants and children: a systematic review and meta-analysis. Can J Anesth/J Can Anesth 70, 749–770 (2023). https://doi.org/10.1007/s12630-023-02418-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-023-02418-1