
Abstract
Delayed-onset muscle soreness (DOMS) is quite a common consequence of unaccustomed strenuous exercise, especially exercise containing eccentric contraction (lengthening contraction, LC). Its typical sign is mechanical hyperalgesia (tenderness and movement related pain). Its cause has been commonly believed to be micro-damage of the muscle and subsequent inflammation. Here we present a brief historical overview of the damage-inflammation theory followed by a discussion of our new findings. Different from previous observations, we have observed mechanical hyperalgesia in rats 1–3 days after LC without any apparent microscopic damage of the muscle or signs of inflammation. With our model we have found that two pathways are involved in inducing mechanical hyperalgesia after LC: activation of the B2 bradykinin receptor–nerve growth factor (NGF) pathway and activation of the COX-2-glial cell line-derived neurotrophic factor (GDNF) pathway. These neurotrophic factors were produced by muscle fibers and/or satellite cells. This means that muscle fiber damage is not essential, although it is sufficient, for induction of DOMS, instead, NGF and GDNF produced by muscle fibers/satellite cells play crucial roles in DOMS.
Similar content being viewed by others


Introduction
It is likely almost everyone has had more than one experience of delayed-onset muscle soreness (DOMS) after, e.g., mountain climbing for the first time for a long while, an occasional baseball game, or running in a once-a-year school sports meeting. It is quite a common consequence of unaccustomed strenuous exercise, especially exercise containing eccentric contraction (lengthening contraction, LC), in which muscle is being stretched while it is contracted [1]. Even athletes who exercise every day experience DOMS when they perform a different type of sport or practice new skills. DOMS is different from the acute pain experienced during and shortly after exercise; it usually appears after a pain-free period (12–24 h), peaks at 24–72 h, and disappears within 7 days of the exercise [2–4]. The existence of this pain-free period has made DOMS somewhat mysterious. The most characteristic symptoms of DOMS are tenderness and movement-induced pain in the exercised muscle; both are types of mechanical hyperalgesia, and there is usually no pain at rest [4]. DOMS is usually subclinical, because people recover from the soreness without medical treatment. However, DOMS may interfere with the motor performance of athletes, and there is a possibility that DOMS will lead to more debilitating and chronic injury [5] and result in chronic pain and/or hyperalgesia, with plastic changes in the central nervous system [6]. Decreases in the maximum power of the muscle and in the range of motion accompany DOMS [7–9]. These decreases are believed to be related to micro damage of the subcellular structure of the muscle fibers [10], but a discussion of the mechanism is beyond the scope of this review.
Many possible causes of DOMS have been proposed [9]; the most popularly accepted is damage of muscle fibers and subsequent inflammation [11]. Our recent research has revealed that muscle fiber damage and inflammation are sufficient but not essential for DOMS. In this review we give a brief overview of these factors; we then describe our recent findings obtained from experimental DOMS in rats and mice. Finally, we briefly introduce methods for prevention and treatment of DOMS.
Historical overview
The first report on soreness (DOMS) that appears 12 or 24 h after exercise was made by Hough [12], who proposed a hypothesis of “rupture of the muscle fiber (or connective tissue between muscle fibers)” as the cause of DOMS because soreness was observed after quick and strong contraction.
That lengthening (eccentric) but not shortening (concentric) contraction (abbreviated LC and SC, respectively) is associated with DOMS was first proposed by Asmussen [1], and later confirmed by other researchers [13, 14]. As suggested by Hough [12], muscle damage was observed after exercise, especially after LC [15–17]. In mice, slow muscle (e.g. soleus muscle) was shown to be less susceptible to LC than fast muscle (e.g. the extensor digitorum longus, EDL, muscle) [18]. With a biopsy of human muscle, type II muscle fibers (fast twitch fibers) were reported to be more susceptible to damage following exercise [19, 20]. After LC, damage including ballooning of the fiber, marked streaming, broadening, and sometimes total disruption, of the Z-band, focal disruption of the striated band pattern, and disorganized sarcomeres [15, 17] were found in the muscle of both humans and animals. Accumulation of inflammatory cells (neutrophils and then macrophages) is found in or around damaged muscle fibers after LC [3, 21], but was also observed after stretching and SC [22]. Increase of IL-6 was found in human plasma [21], and that of mRNAs for IL-6, IL-8, and COX-2 was observed in exercised muscle of humans [23]. In these studies no comparisons were made between exercise patterns (LC or SC).
Different forms of exercise have been used to induce DOMS, including downhill running, lengthening of the muscle by use of a machine while the muscle was contracted voluntarily, or by electrical stimulation by use of a surface electrode. It has been shown that lengthening exercise with voluntary contraction induces less muscle damage than contraction induced by electrical stimulation by use of a surface electrode, although the level of soreness was approximately the same [24]. Quantitative studies on the relationship between the extent of muscle damage or mechanical hyperalgesia and exercise conditions (angular velocity and range of motion) have been performed. Angular velocity dependent severe damage was observed in a study in which the muscle contraction was induced by a surface electrode [8] whereas almost no damage was observed with electrical stimulation of the nerve [25]. Even isometric contraction induced by electrical stimulation with a surface electrode resulted in more muscle damage [26, 27]. The authors of the latter experiment suggested that one possible reason is a high mechanical stress on the muscle fibers activated in a non-selective, synchronous, and spatially fixed manner. This may be also true for LC induced by electrical stimulation by use of surface electrodes.
Biochemical studies have revealed leakage of such enzymes as creatine kinase and lactic dehydrogenase from exercised muscle [17]. Both histological changes and leakage of enzymes from exercised muscle have led to the idea that muscle damage is the cause of DOMS. The presence of invading inflammatory cells (macrophages) in the muscle suggests that inflammation is a cause of DOMS (reviewed elsewhere [11]). A recent intensive, comprehensive study [28] of humans found no difference between markers of inflammation for subjects who underwent LC and those who underwent SC. The involvement of inflammation was also examined by using anti-inflammatory drugs. However, the effects of the drugs differed among laboratories, and there were more reports of effective results when a drug was administered prophylactically (before exercise) than when it was given therapeutically (after exercise) (reviewed elsewhere [9]). A very recent investigation with a placebo control showed that application of topical diclofenac sodium gel 1 % over the exercised leg every 3 h for 24 h helped to reduce DOMS [29].
Lactic acid, found at increased levels in muscles and plasma shortly after exercise [30], was once believed to be a cause of DOMS. However, this hypothesis has been strongly discredited by the discovery that concentric (shortening) exercise, which involves greater metabolism, fails to produce DOMS [30]. In addition, lactic acid levels return to pre-exercise levels within an hour after exercise. Therefore, although lactic acid may contribute to the acute pain associated with fatigue after intense exercise, or initiate DOMS, it cannot be a crucial molecule when DOMS is at its peak.
Increases in resting muscle activity (EMG activity) [31] and connective tissue damage [32] have also been proposed as the cause of DOMS.
New mechanism
Because mechanical hyperalgesia without damage is observed for muscle undergoing LC by electrical stimulation of the nerve [25], the mechanism of DOMS must involve other than damage and/or inflammation. We propose here a new mechanism in which nerve growth factor (NGF) and glial cell line-derived neurotrophic factor (GDNF) produced by muscle fibers and/or satellite cells are themselves responsible for DOMS.
As mentioned in the previous section, muscle damage and the subsequent inflammation after exercise has been reported after many studies, and is thus the most commonly accepted cause of DOMS. However, several reports have suggested this may not be the real cause of DOMS. The time course of the damage and degenerative changes does not fit well with the time course of DOMS, and similar changes, for example disrupted sarcolemma, degenerating fibers, Z-line streaming, and central nuclei are observed among pain-free individuals and regularly exercising athletes [3, 33, 34]. Second, DOMS can be observed in cases without damage of the muscle [24, 25]. Third, anti-inflammatory drugs (NSAID) rarely help to reduce DOMS that has developed mechanical hyperalgesia (reviewed elsewhere [9]).
For better insight into the mechanism of DOMS, animal models are needed for evaluation of the mechanical hyperalgesia of exercised muscle. We contracted the hindpaw extensors of rats, mainly the EDL muscle, by electrically stimulating the common peroneal nerve while synchronously stretching the muscles [35]. The gastrocnemius muscle of rabbits [36], rats [5, 37] and mice [38] has also been used for this purpose.
To evaluate the mechanical withdrawal threshold a parallel of the human mechanical (pressure) pain threshold) of the muscle through the skin, we used a Randall–Selitto apparatus equipped with a larger tip than that supplied by the distributor. The same has been done for humans, using probes with a diameter of 1 cm or with surface area of 1 cm2 [39, 40]. Use of larger probes is based on evidence obtained experimentally [41] and by computer simulation [42–44]. The measured mechanical threshold with these larger probes was not affected by surface anesthesia of the skin over the muscle [38, 41, 45], ensuring the value is indicative of the withdrawal threshold of the deep tissues, including muscles.
Mechanical hyperalgesia after exercise (DOMS) in animal models
In measurements with a Randall–Selitto apparatus (probe diameter 2.6 mm), the mechanical withdrawal threshold decreased significantly 1 day after LC in rats. It reached its lowest point on the second day, and remained low until the third day after exercise [35]. On day four the threshold completely returned to the baseline level [46]. For animals with DOMS produced by the same method, no apparent damage (light microscopic level) of the muscle fibers was observed [37, 47].
That the reduced mechanical withdrawal threshold reflects mechanical hyperalgesia in the exercised muscles was confirmed by an increase in c-Fos expression in the dorsal horn. Expression of this protein in the superficial dorsal horn of the spinal cord has been used as a neural marker of pain since Hunt et al. [48] reported that different kinds of noxious stimuli induce its expression in the superficial dorsal horn, which contains secondary neurons receiving nociceptive C-fiber inputs from the skin [49] and muscle [50]. The number of c-Fos-immunoreactive neurons in the dorsal horn was increased only in the animal group that received muscle compression 2 days after LC, especially in the superficial dorsal horn corresponding to laminae I and II at the L4 level of the spinal cord [35]. Compression alone, LC only, and stretching only did not increase c-Fos expression. Thus, neither the compression nor the LC used in this experiment activated the nociceptive pathway 2 days later, the latter corresponds to that spontaneous pain is absent in DOMS [4]. Increased expression of c-Fos in the superficial dorsal horn after compression 2 days after LC was completely suppressed with morphine (10 mg/kg i.p., given 20 min before compression) [35]. These observations provide further evidence that the muscle was hyperalgesic 2 days after LC.
Mechanical hyperalgesia is also observed for mice after LC, but the time course is much shorter than for rats or humans [38].
Facilitated response of muscle thin-fiber afferents in DOMS
What kind afferents are responsible for DOMS? Muscle nociception is believed to be transmitted by thin muscle afferent fibers (Aδ and C-fibers) [51]. To examine whether the activity of muscle thin-fiber afferents is sensitized in DOMS, we recorded single-fiber activity from rat EDL muscle–common peroneal nerve preparations in vitro [52]. We recorded activity from 25 muscle fibers 2 days after LC and from 33 fibers from control animals. The only difference we found was the mechanical sensitivity: the mechanical threshold was lower by half and the magnitude of the response (number of induced discharges) to ramped mechanical stimulation (0–196 mN in 10 s) was twice as large in the exercised group as in the unexercised controls. Spontaneous activity and the responses to other stimuli (ratio of responding fibers and the magnitude of the response to algesic substances, for example bradykinin and ATP [52], and to heat stimulation [53]) were no different between groups. The observed augmented sensitivity to mechanical stimulation is the neural basis for mechanical hyperalgesia after exercise, i.e. DOMS.
Different from our observations are reports suggesting that DOMS is transmitted by thick A-fiber afferents including muscle spindles. This hypothesis is based on observations that pain induced by hypertonic saline did not change after exercise, that A-fiber block increased the pain threshold, and that vibration of the muscle exacerbated muscle pain [54, 55]. The absence of increased sensitivity to hypertonic saline cannot be the reason C-fibers do not contribute to DOMS, because it has been shown that muscle C-fiber sensitivity to hypertonic saline does not change in DOMS [56]. The vibration might have induced reflex muscle contraction and this contraction might have resulted in more pain. Another possibility is that some of the sensitized C-fibers after exercise might be also be sensitive to vibration of the size used in these papers. The same authors also showed that differential block of A-fibers by compression of the nerve increased the pressure pain threshold in the exercised leg [55]. In this case, pain induced at the site of compression might have masked the pain in the exercised leg.
To examine the possible contribution of A-fibers to DOMS, we investigated whether DOMS could be induced in rats treated neonatally with capsaicin, which is known to destroy a large proportion of unmyelinated afferent fibers [57]. Among these animals, LC failed to induce muscular mechanical hyperalgesia [58]. mRNA of NGF in the muscle, which is crucial in maintaining mechanical hyperalgesia (described later in this review), was upregulated similarly in the capsaicin-treated and vehicle-treated animals. These results indicate that C-fiber afferents are essential in transmitting the nociceptive information from exercised muscle in DOMS, and that thick A-fibers are not crucially involved in DOMS.
What causes DOMS?: the B2 receptor-NGF pathway
Bradykinin (later shown to be Arg-bradykinin in rats [59, 60]), abbreviated in this review as BK, an agonist of the B2 bradykinin receptor) is released during exercise via activation of vascular endothelial adenosine receptors [59]. Bradykinin is known to sensitize thin fiber afferents in a variety of tissues to mechanical stimulation via the B2 bradykinin receptor [61–63]. However, BK is not present 2 days after exercise, and hence cannot be responsible for sensitization of muscle thin-fibers to mechanical stimulation in muscle that is hyperalgesic after LC. Its contribution to initiation of DOMS, however, has not been examined. B2 bradykinin receptor antagonist HOE 140 completely suppressed generation of muscular mechanical hyperalgesia when injected before LC, but when injected 2 days after LC failed to reverse the mechanical hyperalgesia that had already developed [64]. To determine the exact time window in which BK acts, we injected B2 antagonist shortly after exercise. DOMS then developed normally, demonstrating that BK acts during exercise and possibly shortly after exercise (up to 1 h). B1 antagonist was ineffective, irrespective of the timing of its injection. These observations indicate that BK, via the B2 bradykinin receptor, is crucially involved in initiating the processes that lead to mechanical hyperalgesia, but it is not a substance that sensitizes nociceptors to induce mechanical hyperalgesia.
What, then, is the agent that sensitizes nociceptors when muscle is sore? NGF is known to be produced in the muscle after ischemia [65] or nerve injury [66], and is also known to induce mechanical hyperalgesia without inducing apparent pain when injected into muscle [67]. Therefore we examined the change in NGF after LC. Upregulation of NGF mRNA and protein occurred in exercised muscle over a time course (12 h to 2 days after LC) comparable with that for muscle mechanical hyperalgesia (Fig. 1a, b). Antibodies to NGF injected intramuscularly 2 days after exercise reversed the muscle mechanical hyperalgesia in 3 h (Fig. 1c). HOE 140 inhibited upregulation of NGF. In contrast, SC or stretching induced neither mechanical hyperalgesia nor NGF upregulation. Upregulation of IL-6 after LC has been reported for humans [21] and mice [68], and the possibility of a contribution by other cytokines has also been examined in this model [64]. All of IL-1, IL-6, and TNF-α mRNAs were upregulated immediately after LC (0 h) and 6 or 12 h after LC. However, they were also upregulated after SC and/or stretching, and, except for IL-6, were not affected by HOE140. However, a contribution of IL-6 to DOMS is not supported because anti-IL-6 antibody failed to reverse the established mechanical hyperalgesia after LC [64].

NGF involvement in DOMS. a NGF mRNA of the EDL was upregulated first 12 h after LC, and continued to be upregulated up to 2 days after LC. b NGF protein was also upregulated in a time course similar to that for mRNA. c Intramuscular injection of anti-NGF antibody reversed already established mechanical hyperalgesia in 3 h. Black filled circles, normal goat IgG injection group; grey filled squares, anti-NGF antibody injection group. Modified from Murase et al. [64]
Murase et al. [64] also showed that rat NGF sensitized C-fiber afferents to mechanical stimulation in the periphery after 10–20 min in excised muscle-nerve preparation (Fig. 2). This latency is too short if it is caused after transport of NGF to the afferent cell body and changes the expression of ion channels or transducers, or neuropeptides, after which these molecules are transported back to the afferent terminals [69]. In addition, because this preparation was detached from the cell body, sensitization should have occurred at the periphery. Several mechanisms have been proposed [70–74] and the sensitizing mechanism of muscular C-fibers is now being studied. Thus, NGF upregulation by activation of B2 bradykinin receptors is essential to mechanical hyperalgesia after exercise.

NGF sensitized muscle C-fiber afferents to mechanical stimulation. a, b Sample recording of muscle C-fibers with intramuscular injection of phosphate-buffered saline (PBS) (a) and NGF (b). Upper right insets in a, b show the location of the receptive field of the fiber. The 1st and 3rd traces are raw recordings of the fiber, and the 2nd and 4th traces show readouts of the mechanical force applied to the receptive field. c Summary of the change in the mechanical threshold. The threshold of the PBS group at each time point was set as 100 %. White circles, PBS group; filled black circles, NGF group. d Summary of the change in the magnitude of the response (number of discharges induced by mechanical stimulation). The magnitude of the response of the PBS group at each time point was set as 100 %. NGF was injected at time 0. *p < 0.05, **p < 0.01 compared with the PBS group at each time point in both c, d. From Murase et al. [64]
The contribution of transient receptor potential vanilloid 1 (TRPV1) to DOMS and NGF-induced mechanical hyperalgesia has been shown by use of TRPV1-deficient mice and by use of a capsaicin antagonist, capsazepine [37, 38].
Because our model showed no apparent inflammatory signs, inflammatory cells are unlikely to be responsible for the production of NGF. Instead, by use of in-situ hybridization, we found upregulation of mRNA signals around the nuclei of muscle fibers and/or satellite cells 12 h after exercise [75]. When inflammation is produced after severe LC or LC induced by surface electrical stimulation [8], or after LC for 2 weeks [5], NGF is produced in inflammatory cells and regenerating muscle fibers.
What causes DOMS? The COX2-GDNF pathway
In addition to the B2 bradykinin receptor and NGF pathway, we showed that cyclooxygenase (COX)-2 and glial cell line-derived neurotrophic factor (GDNF) were also involved in DOMS [47]. COX-2 inhibitors, but not COX-1 inhibitors, given orally before LC completely blocked the development of DOMS, but when given 2 days after LC they failed to reverse the mechanical hyperalgesia. COX-2 mRNA and protein in exercised muscle increased 0–12 h after LC. This time course is a good fit for a trigger of NGF upregulation. However, COX-2 inhibitors did not suppress NGF upregulation after LC. Instead, we found that GDNF mRNA was upregulated in the exercised muscle 12 h–1 day after LC (Fig. 3a) and that this upregulation was blocked by pretreatment with COX-2 inhibitors. mRNAs of other members of the GDNF family, namely, artemin, persephin, and neurturin, were not upregulated [47]. In-situ hybridization studies revealed that COX-2 and GDNF mRNA signals increased at the periphery of skeletal muscle cells and/or satellite cells (around nuclei) 0 and 12 h after LC, respectively (Fig. 3b–d for GDNF). Accumulation of COX-2 mRNA signals was also observed in small blood vessels and epimysium. Intramuscular injection of anti-GDNF antibody 2 days after LC partly reversed DOMS. On the basis of these findings we conclude that GDNF upregulation via COX-2 activation is essential to mechanical hyperalgesia after exercise.

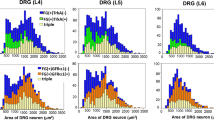
GDNF upregulation in the muscle after LC. a GDNF mRNA of the EDL was upregulated 12 h–1 day after LC. b, c Expression of GDNF mRNA (white arrowheads) in EDL muscle 12 h after LC, shown by use of dark-field photomicrographs of in-situ hybridization histochemistry (oblique sections), was increased on the ipsilateral side (c) compared with the contralateral side (b). Scale bar 100 µm. d Bright-field photomicrograph (longitudinal section) at greater magnification shows in-situ hybridization signals for GDNF mRNA (black arrowhead) in the ipsilateral muscle. Scale bar 10 µm. Note that GDNF mRNA signals are observed around the nuclei of muscle cells and/or satellite cells. Modified from Murase et al. [47]
GDNF also sensitized muscle afferents but, in contrast with NGF, it sensitized Aδ fibers. C-fibers were not sensitized by GDNF (Fig. 4) [76]. This is unexpected because DOMS is a vague sensation and it is generally believed that Aδ-fiber activation in the skin induces sharp pain. Nobody knows what kind of sensation is induced when only muscular Aδ-fibers are activated.

a GDNF sensitized muscle Aδ-fiber afferents to mechanical stimulation. The method of presentation is similar to Fig. 2. The black triangles in b represent the GDNF injection group. # p < 0.05, two-way ANOVA, **p < 0.01, ***p < 0.001, two-way ANOVA followed by Bonferroni’s multiple comparison test. Modified from Murase et al. [76]
Involvement of acid-sensing ion channels (ASIC) in DOMS mechanical hyperalgesia has been demonstrated pharmacologically by use of an antagonist, amiloride [37]. GDNF-induced muscular mechanical hyperalgesia was reversed by amiloride [76]. Fujii et al. [37] also showed that ASIC were expressed in muscle afferent neurons larger than those expressing TRPV1. These observations together are a good fit with our observation that GDNF sensitized Aδ-fibers.
Involvement of TRPV1 and TRPV4 in GDNF-induced mechanical hyperalgesia has been shown in mice deficient in these receptors [38]. Upregulation of GDNF after LC was normal in TRPV1 knockout mice but decreased in TRPV4-deficient mice. Application of TRPV4 antagonist (HC-067047) reversed the mechanical hyperalgesia after LC, but did not affect upregulation of GDNF [38]; thus, the site of action of GDNF is, similar to NGF, in the periphery of the afferents.
The receptor subtype for prostaglandin-E2 [77] that is involved in GDNF production after LC was sought by use of a pharmacological method and EP2 deficient mice, and was demonstrated to be the EP2 subtype [78].
A schematic diagram of the new mechanism for DOMS proposed on the basis of our observations is shown in Fig. 5.

Schematic diagram of the mechanism proposed for DOMS. The upper part of the figure in the shaded area was based on Boix et al. [59]. BK, bradykinin-like substance (Arg-bradykinin in rats); COX2, cyclooxygenase-2; PGs, prostaglandins; EP2, prostaglandin EP2 receptor; GDNF, glial cell line-derived neurotrophic factor; NGF, nerve growth factor; ASIC, acid sensing ion channel; TRPV1 and TRPV4 transient receptor potential vanilloids 1 and 4. Modified from Mizumura et al. [79]
When B2 bradykinin receptor antagonist HOE140 was administered before LC, upregulation after LC of not only NGF but also GDNF and COX-2 was blocked [47], i.e., there is an interaction between these two pathways at the COX-2 level. In contrast, NGF upregulation after LC remained unchanged after application of COX-2 inhibitors yet development of DOMS was blocked [47]. This observation might suggest that NGF produced after LC is not present in amounts large enough to sensitize muscle thin fiber afferents and induce mechanical hyperalgesia. The concentrations of NGF and GDNF used in the experiments that showed sensitization of muscle thin-fiber afferents to mechanical stimulation would have been much higher than those produced after LC. There may be collaboration between NGF and GDNF, although this is not supported by the current understanding that sensory neurons sensitive to NGF and those sensitive to GDNF belong to different neuron groups [80]. Further experiments are needed to clarify this point.
Adaptation (repeated bout effect)
It is well known that DOMS is reduced when the same exercise is repeated after a specific interval. This adaptation, called the “repeated bout effect”, has been attributed to adaptations of neural or connective tissue or cellular mechanisms. In addition, adaptation in excitation–contraction coupling or adaptation in the inflammatory response have also been proposed as mechanisms (reviewed elsewhere [81, 82]; also see Ref. [22]). Hoping to shed light on this effect, on the basis of our findings described above, we found that mechanical hyperalgesia and NGF upregulation were reduced after the 2nd bout of exercise in rats [83]. In addition, these adaptation phenomena were observed even when downstream pathways of the B2 bradykinin receptor were unaffected by its antagonist HOE140. This observation suggests adaptation occurs in the process of BK release, or at a level upstream of adenosine release.
Muscle or fascia?
Some reports indicate fascia is important in DOMS. Itoh et al. [84] examined the electrical sensitivity of tissue at different depths from the skin to the muscle inside after LC in humans, and found the largest decrease in the current threshold of pain at the depth of fascia. Gibson et al. also found that injection of hypertonic saline [56] into the exercised muscle did not change the pain intensity (VAS) after LC in humans, but that injection into the fascia clearly increased it. This observation may indicate that the fascial afferents are important in DOMS. However, the response to hypertonic saline of muscle afferent fibers was not sensitized after LC [56], only mechanical sensitivity was increased [52, 53]. A recent report showed that the electrical pain threshold decrease after LC was greater for fascia than for muscle [85]. To understand the relative contribution of both structures to DOMS, we must differentially measure the mechanical pain threshold of both tissues, or record afferent activity after LC. Innervation of the fascia and its afferent characteristics were only recently reported [86, 87]. Whether fascial thin-fiber afferents are more strongly sensitized in DOMS than muscle afferents remains to be analyzed.
Prevention and treatment of DOMS
Because DOMS may interfere with everyday life and the performance of athletes, and because it may make it difficult for those who are not familiar with exercise to continue exercise for fitness, effective methods for preventing from DOMS are needed. As shown in the previous section, B2 receptor antagonist, COX-2 inhibitor, anti-NGF antibody, and anti-GDNF antibody can, theoretically, be helpful. For the moment, the only drugs applicable for humans are COX-2 inhibitors. As described in the introduction, the effectiveness of non-steroidal anti-inflammatory drugs (NSAID) against DOMS is variable, depending on the time of administration and dosage [9]. A recent systematic review [29] of a large number of reports on the effects of NSAID found that many did not follow an appropriate experimental design. Therefore, they performed a randomized, double-blind, placebo-controlled within-subject experiment. Topical diclofenac (moderately selective to COX-2) sodium gel 1 % was applied over the exercised leg every 3 h for 24 h and was found to help reduce DOMS [29]. It would be interesting to study how this works in the context of the mechanism we have proposed (Fig. 5).
Exercise consisting of a small number of maximal isometric contractions [88] or weak LC [89, 90] beforehand (up to 2 weeks before) is reported to be effective in preventing DOMS. Massage after exercise has been proved to be effective in reducing DOMS in rats [91]. Reduction of DOMS by massage has also been reported for humans by Farr et al. [92], although they did not find any beneficial effect on reduced muscular strength or other functional decline.
Perspective
Several aspects of DOMS must still be studied. When one of the pathways described above (B2 bradykinin receptor-NGF pathway and COX-2-GDNF pathway) is blocked by a B2 bradykinin receptor antagonist or a COX-2 inhibitor, DOMS does not occur. This might suggest an interaction between the two pathways. In addition, the very early event that induces adenosine (possibly ATP) release from the muscle or activates muscle COX-2 during LC, and which might be related to the adaptation mechanism, is also unknown. This must be intimately related to why only LC, and not SC, induces DOMS, and must be studied.
The DOMS model has been used for study of myofascial pain syndrome, because it shows taut band-like muscle hardening, and localized decreased nociceptive threshold in it (trigger point), which are of diagnostic importance for myofascial pain symptoms. When LC was repeated every day, instead of adaptation there were longer-lasting mechanical hyperalgesia and muscle signs of degeneration and regeneration [5]. This observation suggests that this repetitive model is clinically relevant for study of myofascial pain syndrome. Further study of the DOMS mechanism might reveal the mechanism of myofascial pain syndrome and may suggest possibilities for treatment.
References
Asmussen E (1956) Observations on experimental muscular soreness. Acta Rheum Scand 2:109–116
Armstrong RB (1984) Mechanisms of exercise-induced delayed onset muscular soreness: a brief review. Med Sci Sports Exerc 16:529–538
Newham DJ (1988) The consequences of eccentric contractions and their relationship to delayed onset muscle pain. Eur J Appl Physiol 57:353–359
Graven-Nielsen T, Arendt-Nielsen L (2003) Induction and assessment of muscle pain, referred pain, and muscular hyperalgesia. Curr Pain Headache Rep 7:443–451
Hayashi K, Ozaki N, Kawakita K, Itoh K, Mizumura K, Furukawa K, Yasui M, Hori K, Yi S-Q, Yamaguchi T, Sugiura Y (2011) Involvement of NGF in the rat model of persistent muscle pain associated with taut band. J Pain 12:1059–1068
Sluka KA, Danielson J, Rasmussen L, DaSilva LF (2012) Exercise-induced pain requires NMDA receptor activation in the medullary raphe nuclei. Med Sci Sports Exerc 44:420–427
Chapman D, Newton M, Sacco P, Nosaka K (2006) Greater muscle damage induced by fast versus slow velocity eccentric exercise. Int J Sports Med 27:591–598
Mori T, Agata N, Itoh Y, Miyazu-Inoue M, Sokabe M, Taguchi T, Kawakam K (2014) Stretch speed-dependent myofiber damage and functional deficits in rat skeletal muscle induced by lengthening contraction. Physiol Rep 2(11):e12213
Cheung K, Hume P, Maxwell L (2003) Delayed-onset muscle soreness: treatment strategies and performance factors. Sports Med 33:145–164
Friden J, Lieber RL (1992) Structural and mechanical basis of exercise-induced muscle injury. Med Sci Sports Exerc 24:521–530
Smith LL (1991) Acute inflammation: the underlying mechanism in delayed-onset muscle soreness. Med Sci Sports Exerc 23:542–551
Hough T (1902) Ergographic studies in muscular soreness. Am J Physiol 7:76–92
Newham DJ, Mills KR, Quigley BM, Edwards RHT (1983) Pain and fatigue after concentric and eccentric muscle contractions. Clin Sci 64:55–62
Surmeier DJ, Reiner A, Levine MS, Ariano MA (1993) Are neostriatal dopamine receptors co-localized? Trends Neurosci 16:299–305
Newham DJ, McPhail G, Mills KR, Edwards RHT (1983) Ultrastructural changes after concentric and eccentric contractions of human muscle. J Neurol Sci 61:109–122
Friden J, Sjostrom M, Ekblom B (1981) A morphological study of delayed muscle soreness. Experientia 37:506–507
Armstrong RB, Oglive RW, Schwane JA (1983) Eccentric exercise-induced injury to rat skeletal muscle. J Appl Physiol 54:80–93
Head SI, Bakker AJ, Liangas G (2004) EDL and soleus muscles of the C57BL6J/dy2j laminin-alpha 2-deficient dystrophic mouse are not vulnerable to eccentric contractions. Exp Physiol 89:531–539
Friden J, Sjostrom M, Ekblom B (1983) Myofibrillar damage following intense eccentric exercise in man. Int J Sports Med 4(3):170–176
Treede RD, Davis KD, Campbell JN, Raja SN (1992) The plasticity of cutaneous hyperalgesia during sympathetic ganglion blockade in patients with neuropathic pain. Brain 115:607–621
MacIntyre DL, Sorichter S, Mair J, Berg A, McKenzie DC (2001) Markers of inflammation and myofibrillar proteins following eccentric exercise in humans. Eur J Appl Physiol 84:180–186
Pizza FX, Koh TJ, McGregor SJ, Brooks SV (2002) Muscle inflammatory cells after passive stretches, isometric contractions, and lengthening contractions. J Appl Physiol 92:1873–1878
Buford TW, Cooke MB, Shelmadine BD, Hudson GM, Redd L, Willoughby DS (2009) Effects of eccentric treadmill exercise on inflammatory gene expression in human skeletal muscle. Appl Physiol Nutr Metab 34:745–753
Crameri RM, Aagaard P, Qvortrup K, Langberg H, Olesen J, Kjaer M (2007) Myofibre damage in human skeletal muscle: effects of electrical stimulation versus voluntary contraction. J Physiol 583:365–380
Hayashi K, Abe M, Yamanaka A, Mizumura K, Taguchi T (2015) Degenerative histological alteration is not required for the induction of muscular mechanical hyperalgesia after lengthening contraction in rats. J Physiol Sci 65(suppl):S277
Nosaka K, Aldayel A, Jubeau M, Chen TC (2011) Muscle damage induced by electrical stimulation. Eur J Appl Physiol 111:2427–2437
Jubeau M, Muthalib M, Millet GY, Maffiuletti NA, Nosaka K (2012) Comparison in muscle damage between maximal voluntary and electrically evoked isometric contractions of the elbow flexors. Eur J Appl Physiol 112:429–438
Malm C, Sjodin TL, Sjoberg B, Lenkei R, Renstrom P, Lundberg IE, Ekblom B (2004) Leukocytes, cytokines, growth factors and hormones in human skeletal muscle and blood after uphill or downhill running. J Physiol 556:983–1000
Singla N, Desjardins PJ, Cosca EB, Parulan C, Arriaga A, Poole KC, Batz DM, Chang PD (2015) Delayed-onset muscle soreness: a pilot study to assess analgesic study design features. Pain 156:1036–1045
Schwane JA, Watrous BG, Johnson SR, Armstrong RB (1983) Is lactic acid related to delayed-onset muscle soreness? Phys Sportsmed 11:124–131
De Vries HA (1966) Quantitative electromyographic investigation of the spasm theory of muscle pain. Am J Phys Med 45:119–134
Lieber RL, Friden J (1988) Selective damage of fast glycolytic muscle fibres with eccentric contraction of the rabbit tibialis anterior. Acta Physiol Scand 133:587–588
Hikida RS, Staron RS, Hagerman C, Sherman WM, Costill DL (1983) Muscle fiber necrosis associated with human marathon runners. J Neurol Sci 59:185–203
Meltzer HY, Kuncl RW, Yang V (1976) Incidence of Z band streaming and myofibrillar disruptions in skeletal muscle from healthy young people. Neurology 26:853–857
Taguchi T, Matsuda T, Tamura R, Sato J, Mizumura K (2005) Muscular mechanical hyperalgesia revealed by behavioural pain test and c-Fos expression in the spinal dorsal horn after eccentric contraction in rats. J Physiol 564:259–268
Itoh K, Kawakita K (2002) Effect of indomethacin on the development of eccentric exercise-induced localized sensitive region in the fascia of the rabbit. Jpn J Physiol 52:173–180
Fujii Y, Ozaki N, Taguchi T, Mizumura K, Sugiura Y (2008) TRP channels and ASICs mediate mechanical hyperalgesia in models of inflammatory muscle pain and delayed-onset muscle soreness. Pain 140:292–304
Ota H, Katanosaka K, Murase S, Kashio M, Tominaga M, Mizumura K (2013) TRPV1 and TRPV4 play pivotal roles in delayed-onset muscle soreness. PLoS ONE 8:e65751
Fischer AA (1987) Pressure algometry over normal muscles. Standard values, validity and reproducibility of pressure threshold. Pain 30:115–126
Andersen H, Arendt-Nielsen L, Danneskiold-Samsoe B, Graven-Nielsen T (2006) Pressure pain sensitivity and hardness along human normal and sensitized muscle. Somatosens Mot Res 23:97–109
Takahashi K, Taguchi T, Itoh K, Okada K, Kawakita K, Mizumura K (2005) Influence of surface anesthesia on the pressure pain threshold measured with different-sized probes. Somatosens Mot Res 22:299–305
Takahashi K, Mizumura K (2004) 3-D finite element analysis of stresses in the epidermis and the muscle given by a transcutaneous pressure. Jpn J Physiol 54(Suppl):S175
Finocchietti S, Takahashi K, Okada K, Watanabe Y, Graven-Nielsen T, Mizumura K (2013) Deformation and pressure propagation in deep-tissue duiring mechanical painful pressure stimulation. Med Biol Eng Comput 51:113–122
Finocchietti S, Andresen T, Arendt-Nielsen L, Graven-Nielsen T (2012) Pain evoked by pressure stimulation on the tibia bone—influence of probe diameter on tissue stress and strain. Eur J Pain 16:534–542
Nasu T, Taguchi T, Mizumura K (2010) Persistent deep mechanical hyperalgesia induced by repeated cold stress in rats. Eur J Pain 14:236–244
Taguchi T, Matsuda T, Mizumura K (2007) Change with age in muscular mechanical hyperalgesia after lengthening contraction in rats. Neurosci Res 57:331–338
Murase S, Terazawa E, Hirate K, Yamanaka H, Kanda H, Noguchi K, Ota H, Queme F, Taguchi T, Mizumura K (2013) Upregulated glial cell line-derived neurotrophic factor through cyclooxygenase-2 activation in the muscle is required for mechanical hyperalgesia after exercise in rats. J Physiol 591:3035–3048
Hunt SP, Pini A, Evan G (1987) Induction of c-fos-like protein in spinal cord neurons following sensory stimulation. Nature 328:632–634
Sugiura Y, Lee CL, Perl ER (1986) Central projections of identified, unmyelinated (C) afferent fibers innervating mammalian skin. Science 234:358–361
Ling LJ, Honda T, Shimada Y, Ozaki N, Shiraishi Y, Sugiura Y (2003) Central projection of unmyelinated (C) primary afferent fibers from gastrocnemius muscle in the guinea pig. J Comput Neurol 461(2):140–150
Graven-Nielsen T, Mense S (2001) The peripheral apparatus of muscle pain: evidence from animal and human studies. Clin J Pain 17:2–10
Taguchi T, Sato J, Mizumura K (2005) Augmented mechanical response of muscle thin-fiber sensory receptors recorded from rat muscle-nerve preparations in vitro after eccentric contraction. J Neurophysiol 94:2822–2831
Queme F, Taguchi T, Mizumura K, Graven-Nielsen T (2013) Muscular heat and mechanical pain sensitivity after lengthening contraction in humans and animals. J Pain 14:1425–1436
Weerakkody NS, Whitehead NP, Canny BJ, Gregory JE, Proske U (2001) Large-fiber mechanoreceptors contribute to muscle soreness after eccentric exercise. J Pain 2:209–219
Weerakkody NS, Percival P, Hickey MW, Morgan DL, Gregory JE, Canny BJ, Proske U (2003) Effects of local pressure and vibration on muscle pain from eccentric exercise and hypertonic saline. Pain 105:425–435
Gibson W, Arendt-Nielsen L, Taguchi T, Mizumura K, Graven-Nielsen T (2009) Increased pain from muscle fascia following eccentric exercise: animal and human findings. Exp Brain Res 194:299–308
Nagy JI, Iversen LL, Goedert M, Chapman D, Hunt SP (1983) Dose-dependent effects of capsaicin on primary sensory neurons in the neonatal rat. J Neurosci 3:399–406
Kubo A, Koyama M, Tamura R, Takagishi Y, Murase S, Mizumura K (2012) Absence of mechanical hyperalgesia after exercise (delayed-onset muscle soreness) in neonatally capsaicin-treated rats. Neurosci Res 73:56–60
Boix F, Rosenborg L, Hilgenfeldt U, Knardahl S (2002) Contraction-related factors affect the concentration of a kallidin-like peptide in rat muscle tissue. J Physiol 544:127–136
Wilson SR, Boix F, Holm A, Molander P, Lundanes E, Greibrokk T (2005) Determination of bradykinin and arg-bradykinin in rat muscle tissue by microdialysis and capillary column-switching liquid chromatography with mass spectrometric detection. J Sep Sci 28:1751–1758
Koda H, Mizumura K (2002) Sensitization to mechanical stimulation by inflammatory mediators, by second messengers possibly mediating these sensitizing effects, and by mild burn in canine visceral nociceptors in vitro. J Neurophysiol 87:2043–2051
Mense S, Meyer H (1988) Bradykinin-induced modulation of the response behaviour of different types of feline group III and IV muscle receptors. J Physiol 398:49–63
Mizumura K, Sugiura T, Katanosaka K, Banik RK, Kozaki Y (2009) Excitation and sensitization of nociceptors by bradykinin: what do we know– Exp Brain Res 196:53–65
Murase S, Terazawa E, Queme F, Ota H, Matsuda T, Hirate K, Kozaki Y, Katanosaka K, Taguchi T, Mizumura K (2010) Bradykinin and nerve-growth factor play pivotal roles in muscular mechanical hyperalgesia after exercise (delayed-onset muscle soreness). J Neurosci 30:3752–3761
Turrini P, Gaetano C, Antonelli A, Capogrossi MC, Aloe L (2002) Nerve-growth factor induces angiogenic activity in a mouse model of hindlimb ischemia. Neurosci Lett 323:109–112
Amano T, Yamakuni T, Okabe N, Sakimura K, Takahashi Y (1991) Production of nerve-growth factor in rat skeletal muscle. Neurosci Lett 132:5–7
Andersen H, Arendt-Nielsen L, Svensson P, Danneskiold-Samsoe B, Graven-Nielsen T (2008) Spatial and temporal aspects of muscle hyperalgesia induced by nerve-growth factor in humans. Exp Brain Res 191:371–382
Tomiya A, Aizawa T, Nagatomi R, Sensui H, Kokubun S (2004) Myofibers express IL-6 after eccentric exercise. Am J Sports Med 32:503–508
Harrington AW, Ginty DD (2013) Long-distance retrograde neurotrophic factor signalling in neurons. Nat Rev Neurosci 14:177–187
Di Castro A, Drew LJ, Wood JN, Cesare P (2006) Modulation of sensory neuron mechanotransduction by PKC- and nerve-growth factor-dependent pathways. Proc Natl Acad Sci USA 103:4699–4704
Malik-Hall M, Dina OA, Levine JD (2005) Primary afferent nociceptor mechanisms mediating NGF-induced mechanical hyperalgesia. Eur J Neurosci 21(12):3387–3394
Bonnington JK, McNaughton PA (2003) Signalling pathways involved in the sensitisation of mouse nociceptive neurones by nerve-growth factor. J Physiol 551:433–446
Zhang X, Huang J, McNaughton PA (2005) NGF rapidly increases membrane expression of TRPV1 heat-gated ion channels. EMBO J 24:4211–4223
Zhu W, Oxford GS (2007) Phosphoinositide-3-kinase and mitogen activated protein kinase signaling pathways mediate acute NGF sensitization of TRPV1. Mol Cell Neurosci 34:689–700
Murase S, Yamanaka Y, Kanda H, Mizumura K (2012) COX-2, nerve-growth factor (NGF) and glial cell-derived neurotrophic factor (GDNF), which play pivotal roles in delayed-onset muscle soreness (DOMS), are produced by exercised skeletal muscle. J Physiol Sci 62(suppl):S179
Murase S, Kato K, Taguchi T, Mizumura K (2014) Glial cell line-derived neurotrophic factor sensitized the mechanical response of muscular thin-fiber afferents in rats. Eur J Pain 18:629–638
Sugimoto Y, Narumiya S (2007) Prostaglandin E receptors. J Biol Chem 282:11613–11617
Ota H, Katanosaka K, Murase S, Narumiya S, Mizumura K (2015) Contribution of EP2 receptor to generation of delayed-onset muscle soreness. J Physiol Sci 65(Suppl):S234
Mizumura K, Taguchi T, Murase S (2014) Facilitation of mechanical response of muscle nociceptors after exercise: Involvement of neurotrophic factors. In: Graven-Nielsen T, Arendt-Nielsen L (eds) Musculoskeletal pain: Basic mechanisms and implications, IASP Press, Washington DC, pp 223–235
Priestley JV, Michael GJ, Averill S, Liu M, Willmott N (2002) Regulation of nociceptive neurons by nerve-growth factor and glial cell line derived neurotrophic factor. Can J Physiol Pharmacol 80:495–505
McHugh MP, Connolly DA, Eston RG, Gleim GW (1999) Exercise-induced muscle damage and potential mechanisms for the repeated bout effect. Sports Med 27:157–170
McHugh MP (2003) Recent advances in the understanding of the repeated bout effect: the protective effect against muscle damage from a single bout of eccentric exercise. Scand J Med Sci Sports 13:88–97
Urai H, Murase S, Mizumura K (2013) Decreased nerve-growth factor upregulation is a mechanism for reduced mechanical hyperalgesia after the second bout of exercise in rats. Scand J Med Sci Sports 23:e96–101
Itoh K, Okada K, Kawakita K (2004) A proposed experimental model of myofascial trigger points in human muscle after slow eccentric exercise. Acupunct Med 22:2–12
Lau WY, Blazevich AJ, Newton MJ, Wu SS, Nosaka K (2015) Changes in electrical pain threshold of fascia and muscle after initial and secondary bouts of elbow flexor eccentric exercise. Eur J Appl Physiol 115:959–968
Tesarz J, Hoheisel U, Wiedenhofer B, Mense S (2011) Sensory innervation of the thoracolumbar fascia in rats and humans. Neuroscience 194:302–308
Taguchi T, Yasui M, Kubo A, Abe M, Kiyama H, Yamanaka A et al (2013) Nociception originating from the crural fascia in rats. Pain 154:1103–1114
Chen HL, Nosaka K, Pearce AJ, Chen TC (2012) Two maximal isometric contractions attenuate the magnitude of eccentric exercise-induced muscle damage. Appl Physiol Nutr Metab 37:680–689
Chen HL, Nosaka K, Chen TC (2011) Muscle damage protection by low-intensity eccentric contractions remains for 2 weeks but not 3 weeks. Eur J Appl Physiol 112:555–565
Chen TC, Tseng WC, Huang GL, Chen HL, Tseng KW, Nosaka K (2013) Low-intensity eccentric contractions attenuate muscle damage induced by subsequent maximal eccentric exercise of the knee extensors in the elderly. Eur J Appl Physiol 113:1005–1015
Urakawa S, Takamoto K, Nakamura T, Sakai S, Matsuda T, Taguchi T, Mizumura K, Ono T (2015) Manual therapy ameliorates delayed-onset muscle soreness and alters muscle metabolites in rats. Physiol Rep 3(2):e12279
Farr T, Nottle C, Nosaka K, Sacco P (2002) The effects of therapeutic massage on delayed-onset muscle soreness and muscle function following downhill walking. J Sci Med Sport 5:297–306
Author information
Authors and Affiliations
Corresponding author
About this article

Cite this article
Mizumura, K., Taguchi, T. Delayed onset muscle soreness: Involvement of neurotrophic factors. J Physiol Sci 66, 43–52 (2016). https://doi.org/10.1007/s12576-015-0397-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12576-015-0397-0