
Abstract
Background
People with advanced cancer experience psychological distress due to physical symptoms, functional decline, and a limited prognosis. Difficult thoughts, feelings, and emotions may exacerbate distress and lead to avoidance of these experiences which is sometimes referred to as experiential avoidance (EA). Advanced cancer patients may be more likely to engage in EA especially when no obvious solutions to their problems exist. This study aims to examine the terms used to describe EA, the processes that might indicate EA, associations between EA and psychological distress, and to understand why individuals might engage in EA.
Methods
A mixed-methods review. Literature search of Medline, Embase, Psych INFO, and CINAHL 1980–October 2019. Inclusion: adults ≥ 18 years; advanced cancer not amenable to cure. Exclusion: no measures of EA or psychological distress. Risk of bias and study quality assessed. Evidence of statistical techniques collected. Themes coded, grouped, and developed based on meaning.
Results
Nineteen studies identified, 13 quantitative studies and 6 qualitative. The quantitative of which 6 compared early-stage cancers with advanced cancers and examined subscales of EA alongside mood, quality of life, and psychological distress. EA covers a range or terms of which ‘avoidant coping’ is the commonest. EA is manifest as cognitive, behavioural, and emotional avoidance. A thematic synthesis suggests the function of EA is to protect people from distress, and from confronting or expressing difficult emotions by avoiding communication about cancer, controlling negative information, and maintaining normality and hope and optimism.
Conclusions
EA may be beneficial in the short term to alleviate distress, but in the longer term, it can impair function and limit engagement in life. Greater clinical awareness of the complexity of EA behaviours is needed. Clinicians and researchers should define EA precisely and be aware of the function it may serve in the short and longer term. Future research studies may consider using specific measures of EA as a primary outcome, to assess the impact of psychological interventions such as ACT.
Similar content being viewed by others


Introduction
Improvements in medical treatments mean that people are living longer with advanced, non-curative cancers [1]. An uncertain prognosis, limited life expectancy, and an increasing symptom burden can make life difficult in advanced cancer and lead to psychological distress [2–4]. Distress is often multifactorial, an unpleasant emotional experience that is psychological, social, and/or spiritual in nature, which can interfere with the ability to cope [5]. Negative thoughts may exacerbate the problem and lead to avoidance of social and psychological issues [6]. Individuals with advanced cancer are challenged to engage fully in life whilst living with symptomatic disease and closeness to death [7]. Individuals challenged by a stressor beyond their resources may use cognitive, behavioural, and emotional strategies to manage internal and external demands [1]. Behaviours directed at avoiding the problem to prevent experiencing distress or to lessen emotional reactions are emotion focused and known as ‘avoidance coping’ [8]. Avoidance is identified as an important psychological response [9], and a link is made between avoidance and anxiety [10].
The link between avoidance and anxiety was first alluded to by Freud [11] in psychodynamic therapy, as he noticed that people were sometimes unable to remain in contact with upsetting material, and Freud suggested that as a result, people used repression as a way of coping with this distress [11]. Cognitive and dialectical therapy identified avoidance of unpleasant experiences and contexts in which they arose as a problematic way of dealing with distress [12]. Evidence exists in the literature of the association between avoidance and anxiety and maladaptive psychological functioning [12–18].
A wider definition of avoidance behaviours has developed in the psychological literature called experiential avoidance (EA) which consists of two related parts: (a) the unwillingness to remain in contact with troublesome experiences (including bodily sensations, emotions, thoughts, memories, and behavioural predispositions) and (b) action taken to alter these experiences or the events that elicit them which includes all forms of avoidance and escape [19].
EA encompasses different cognitive, behavioural, and emotional avoidance behaviours which over time have been identified, measured, and labelled in both the coping and psycho-oncology literature [20, 21]. The subscales of avoidance that are measured include escape, denial, behavioural and mental disengagement, and wishful thinking [22].
For the purposes of this review and for ease of use regarding definitions, we have categorised and defined avoidance in the following ways. Cognitive avoidance refers to attempts to suppress, avoid, disengage, and distract from thoughts and memories that may be intrusive and cause distress and worry [9, 23–25]. Behavioural avoidance refers to actions to physically distance, disengage, distract, and prevent contact with unwelcome experiences [26, 27]. Emotional avoidance refers to actions to alleviate or manage the distress difficult experiences may cause and includes denial, repression, wishful thinking, blunting—only attending to positive information—and using substances like alcohol or activities such as sleep to avoid or numb experiences [23, 24, 26, 27]. The different types of avoidance that make up EA are depicted in Fig. 1.

Types of avoidance in EA
EA is considered to be a core psychopathological process in various empirically based modern cognitive behavioural therapies, for example, in Acceptance Commitment Therapy (ACT) [28] where it is acknowledged that attempts at avoidance may help to reduce and alleviate distress in the short term, but paradoxically, if it is used consistently over the longer term, it may reinforce the strength and frequency of upsetting experiences and concomitant distress. This is because avoidance strategies are often under verbal control and so are likely to influence further cognitions [18, 29]. EA also consists of taking action to avoid and escape from situations in which unpleasant experiences are evoked, thus restricting peoples’ activities [14]. EA becomes particularly problematic when it becomes habitual and energy is expended to prevent exposure to unwanted experiences [14]. In this circumstance, the avoidance is critical in the development and maintenance of psychopathology [19] and it is likely to lead to a lower quality of life [30].
A link has been established between cognitive and behavioural avoidance and higher levels of anxiety [31] and depressive symptoms [32].
A longitudinal cancer study found avoidance coping at baseline predicted chronic and acute stressors 4 years later and depressive symptoms 10 years later [21]. In mixed cancers at different stages, those who used cognitive and behavioural escape avoidance experienced more emotional distress [20] and denial in prostate, breast, and colon cancer was associated with higher anxiety and depression as well as cancer-related worries [33].
Our own research in advanced cancer found a negative association between acceptance and psychological morbidity which generated our interest to explore EA further [34]. Whilst there is evidence that avoidance exists and may be a maladaptive response to distress in cancer [35], there is no consensus on the definition and meaning of EA. This lack of definition makes it difficult to reach conclusions about the reasons for EA and its association with psychological distress in the cancer population.
The concept of EA is the focus and frame of our review in the advanced cancer population where recognition of the phenomenon and timely clinical intervention may be critically important. We propose to explore how EA is formulated in the advanced cancer literature: what terms are used and what measures or proxy measures are used to evaluate the phenomenon. Also, we are interested to see how those with advanced cancer articulate their experiences of illness insofar as these shed light on EA.
There has been no previous systematic review in this area, and our quantitative and qualitative review aims to [1] identify how EA is described in the advanced cancer literature and the processes that might indicate EA, [2] explore associations between EA and psychological distress, and [3] explore reasons for engaging in EA.
Methods
The systematic review was registered on Prospero on 26th July 2019 (registration number CRD42019139700; https://www.crd.york.ac.uk/PROSPERO/) and follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses [36].
We searched Embase, Medline, PsychINFO, CINAHL, conference abstracts, reference lists, and relevant reviews on the topic from January 1984 to October 2019. Our start date for the review was pegged to Lazarus and Folkman’s (1984) transactional theory of stress and coping [1], seminal work that established the link between coping and stress [37]. Search terms were generated using MeSH and subject headings to create the search term list for each database (Supplementary material 1). Terms were included for advanced cancer, experiential avoidance, and avoidance coping.
We included randomised controlled trials (RCTs) and non-randomised trials, observational studies, and qualitative and mixed-methods studies published in the English language. Studies in the advanced, recurrent, or metastatic adult [18 years and above] cancer population were included if participants were identified using recognised diagnostic criteria and/or participants were treated with palliative intent. Studies with a mix of early and late cancer stages III and IV were included if data were analysed separately. Studies were included if they used validated measures of EA or coping strategies—e.g. subscales of the COPE [27], or Brief COPE [38]—and measures of the effect on quality of life of psychological distress/mood disturbance.
One reviewer (SD) screened all titles and abstracts and selected relevant studies. SD completed a full text review of all the studies that met the inclusion criteria, and a second reviewer (MA) independently checked the included studies to ensure they met the criteria. Any disagreements between the two reviewers were resolved through discussion with the wider research team (AL/MS/JL). SD extracted data from included studies and was checked by MA.
Outcomes of Interest
Our primary outcome is EA. As very few measures exist that measure EA directly, studies that used outcomes that assessed coping with stress were included. Outcome measures included the Coping Orientation to Problems Experienced (COPE/Brief COPE) [27, 38] and the Impact of Events Scale (IES) [24]. These measures contain subscales of types of avoidance that bear similarities with EA (Table 1). Our second outcome is psychological distress as it is commonly measured in association with coping styles in the cancer population [39].
We used a broad approach to assess psychological distress that included measures of mood disturbance, and psychiatric morbidity, as well as subscales of quality-of-life measures that assessed emotional well-being such as the FACT G [40].
Quality Assessments
Two reviewers (SD and MA) independently assessed studies using the QualSyst tool [41], which was developed to standardise assessments of studies using different criteria to measure methodological quality and risk of bias at study and outcome level in both primary quantitative and qualitative research studies included in systematic reviews. The quantitative assessment consists of 14 items of which 11 items were applicable (no RCTs included). The qualitative assessment consists of 10 items of which all were applicable. Answers to questions in both assessments were categorised into one of three groups: fully, partially, or not answered. Study quality was assessed as good when the percentage of questions partially or fully answered combined exceeded 75%.
Analysis
Quantitative Data
Data were extracted on statistical techniques used to explain the data including effect sizes, standard deviations, means, and p values. We planned, if appropriate, to do a meta-analysis where identified studies were similar in design and the tools that they used.
Qualitative Data
An analysis of quotations extracted from qualitative studies followed Thomas and Harden’s stepwise method for the synthesis of qualitative research results in systematic reviews [42]. Results were coded line by line according to meaning, organised into relevant areas and analytic themes developed by SD, which were reviewed and discussed with MA. A draft summary of the thematically organised grouped codes was discussed by other researchers (MS, JL, AL) who commented on the draft until a final version was agreed upon.
Results
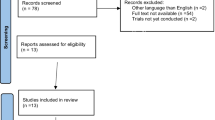
From the 1448 retrieved reports, 19 met the inclusion criteria and were included in the review (Fig. 2). Thirteen reported quantitative data and 6 reported qualitative data. Before presenting these results in two respective sections, we detail how EA is variously described in the advanced cancer literature.

Flow diagram of literature search
EA Descriptors
A range of different terms were used to describe EA. A word cloud of EA descriptors depicts the most common words (larger font) and different terms used (Fig. 3). Emotional avoidance was often used [39, 43–45], and frequently in combination with behavioural avoidance [45–48]. Cognitive avoidance was rarely used alone [49] but usually with behavioural avoidance [50, 51] and emotional avoidance [52]. ‘Avoidant coping’ was also used as a descriptor for types of EA, but studies used different tools to assess this [45, 46, 50], making it difficult to determine what it encompassed within the terms of an individual study. For example, in Kershaw et al. [45], 6 different types of behaviour were classified as ‘avoidant coping’ using the Brief COPE [38] which included self-distraction, venting, humour, denial, behavioural disengagement, and alcohol/drug use. Once identified, these behaviours were not referred to again individually, but only collectively as ‘avoidant coping’. Alternative terms have also been used to describe similar constructs, for example, cognitive avoidance [49] and mental disengagement [51], demonstrating that the nature of the type of avoidance is not always clearly described in studies.

Word cloud of EA descriptors
Different expressions of emotion were also described as ‘avoidant coping’. These included ‘venting’ [45, 46, 53] and ‘self-blame’ [44] which were found to be detrimental and associated with a negative appraisal of illness. Venting implies the process of dealing with emotions is problematic, and maladaptive [54]. It is less clear whether self-blame is a type of EA. In Nipp et al. [44], 38% of ex-smokers with lung cancer used self-blame whilst 28% used denial. Self-blame is linked with stigma and poor adjustment [55] and is also associated with shame and guilt. Guilt may render someone powerless and unable to galvanise themselves to actively cope with their disease, which may explain why it is included as a type of EA.
The descriptors found in the qualitative results included suppression of thoughts to protect themselves [56]. Distraction—to keep minds busy and provide relief from thoughts [2]. Distancing—to keep away from friends and family to avoid talking about cancer [2, 56], or only talking about normal things [57]. Blunting—helped to avoid negative information [58] or too much information [2]. Positive denial—helped people to feel positive and think optimistically [58] and to avoid negative thinking [57]. Conscious denial helped people refuse to think or acknowledge cancer [56, 59].
Quantitative Results
Study Characteristics
Thirteen studies had a total sample of 1568 patients with advanced cancer, with a median sample size of 120 (range 32–350). Fifty-three percent of the patients were male, and mean ages across the sample ranged from 34 to 70 years. The participants were recruited from single hospital sites, outpatient clinics, and an inpatient palliative care unit [43, 44, 48, 51–53] and from multiple hospital sites, cancer centres, and satellite clinics in the same area [39, 45–47, 49, 50]. One study did not provide details about the identification of participants but gave details of recruitment by post [60] (Table 2).
Six studies used a comparative design, whereby coping was compared between early- and late-stage cancer patients [49–52, 60], and in 1, a comparison was made between patients and carers [45]. The participants were still in receipt of cancer treatments (chemotherapy, radiotherapy, hormone therapy, and surgery) in 10 studies [39, 43–47, 49–52]. No reporting of treatment occurred in 2 studies [48, 53], and in 1, the participants received no treatment [60] (Table 2).
Six studies were longitudinal designs [43, 48–52] of which 1 focused specifically on denial [43] and another on cognitive avoidance [49]. The aim of most studies was not to specifically examine EA, but to look at the different coping strategies people used to ascertain if there were any associations with mood, quality of life, and psychological distress. Six of the cross-sectional studies [39, 44, 46, 47, 60] were observational, whereby patients completed self-report measures of coping, psychological distress, and quality of life. A cross-sectional study [53] adapted and modified coping strategies using a structured interview method [61] based on hypothetical situations to develop a theoretical framework [62]. A form of coping called blunting was identified related to EA whereby threatening information was avoided or treated less seriously (Table 2).
Measures of Coping and Psychological Distress
The most frequently used outcome measures were the Coping Orientation to Problems Experienced (COPE; [27, 46, 52]) and the Brief COPE [38] which was used in 4 studies [39, 44, 45, 47]. The COPE is designed to measure ways in which people respond to stress and contains subscales of EA. The Brief COPE has been validated in incurable cancer and shown to have good psychometric properties [63]. Another measure that was used is the Impact of Events Scale (IES) [24] which is a measure of stress-related symptoms of avoidance and intrusion, and the IES was used in 3 studies [46, 50, 52]. Definitions of EA are taken from subscales of outcome measures with examples to provide clarity (Table 1).
Measures of psychological distress included the Profile of Mood States (POMS) [64], the Hospital Anxiety and Depression Scale (HADS) [65], the Brief Symptom Inventory (BSI) [66], and the Beck Depression Inventory (BDI) [67], as well as various subscales of quality-of-life measures like the Short Form Survey (SF-12) [68] that assess mental well-being.
Quality Assessment of Quantitative Studies
We present our quality assessment of included quantitative studies using the QualSyst tool [41] in Table 3. Overall, the quality of the studies was good with some improvements needed in specific areas. Of the 13 quantitative studies, 6 used longitudinal survey methods [43, 48–52] and 4 of these had a comparison group [49–52]. Six studies used cross-sectional survey methods [39, 44–47, 60], and 2 of these had a comparison group [45, 60]. One study [53] used an interview method to gather data.
All 13 studies had clear overall objectives, which were achieved; analytic methods were justified and appropriate; and the conclusions of the studies were supported by the results. Study design was generally good with 9 studies having an appropriate design for their research. Three studies had some limitations [44, 45, 52], and in one study [53], the design was unclear.
Sample sizes of advanced cancer patients ranged from 32 to 350. Five of the studies [39, 51–53, 60] had relatively small sample sizes ranging from 32 to 59 participants.
Eleven studies provided full information about the measurement of outcomes with only 2 studies providing partial information [47, 53]. Results were reported in sufficient detail in 9 studies, 3 provided partial information [44, 47, 60], and only 1 did not supply enough information [43]. In almost all studies, analytic methods were well described, justified, and appropriate. In just 1 [53], however, it was unclear how interview data concerning coping behaviours was incorporated into a theoretical model of coping behaviour.
The main critique of the studies (n = 10) was the complete lack of variance reported. Partial information was provided in 3 studies [39, 43, 50] with only 1 providing full information [51]. The strength of the results therefore could not be properly assessed or statistically estimated due to chance [69]. Eight studies provided partial information about comparison variables and 5 provided full information [45, 49, 50, 53, 60]. No controls for confounding were found in 4 studies [43, 44, 49, 53], and limited information was provided in 1 other [46], which could have affected the validity of the results.
Types of Avoidance and Associations with Psychological Distress
Cognitive Avoidance
Four longitudinal studies assessed whether coping strategies were associated with psychological distress and quality of life [49–52]. Prostate cancer patients assessed as anxious at baseline who engaged in cognitive avoidance remained anxious at 1 year [49]. Distress was significantly predicted by anxiety, cognitive avoidance, and lower anxious pre-occupation [49]. A strong correlation was found at baseline between intrusive thoughts and distress. Behavioural attempts to avoid thoughts at 3 months related to psychological distress at 6 months, so avoidance acted as a mediator. Attrition at 6-month follow-up was high, which may represent a selection bias.
Two longitudinal studies compared women with early and advanced gynaecological cancers who had received extensive treatment [51, 52]. In Lutendorf et al. [51], although sample sizes were small (n ≤ 33), cognitive avoidance (mental disengagement) at baseline was significantly associated with a poor relationship with the doctor at 1 year and behavioural disengagement was associated with greater distress. Similarly, giving up attempts to cope were common and strong associations were found between cognitive, behavioural, and emotional avoidance strategies with greater anxiety and depressed mood [52]. However, despite data from this study being longitudinal, the analysis was cross-sectional.
Behavioural Avoidance
De-Faye et al. [53] found behavioural avoidance was used to cope with the social domain of stress. Distraction was used 53% of the time and diverting attention 58% of the time. No associations were found with psychological distress, but interview methods to categorise coping behaviours were unclear which may have reduced associations.
Three cross-sectional studies analysed the effects of coping strategies on mood [45, 47, 60] using the Brief COPE [38], in which avoidant coping was defined as self-distraction, denial, behavioural disengagement, self-blame, and venting. In Sumpio et al. [47], avoidant coping was associated with greater symptom distress, negative appraisal of illness, and greater mood disturbance. Van-Laarhoven et al. [60] compared curative and palliative patients and found behavioural disengagement and denial were positively associated with depression and hopelessness in the palliative group. Expression of negative emotions through venting had a negative predictive effect on emotional functioning in the group.
Kershaw et al. [45] found advanced breast cancer patients used both active and avoidant coping strategies. Small to medium correlations between coping strategies and physical and mental quality-of-life variables showed behavioural disengagement, denial, substances, and venting were significantly associated with more symptom distress and lower mental quality of life. Participants in this study were part of a large interventional randomised controlled trial, so they may not have been typically representative of this population.
Four different stages of treatment were examined in a cross-sectional study of coping in people diagnosed with head and neck cancer [46]. Patients engaged in behavioural disengagement, denial, and emotional ventilation frequently when undergoing treatment and up to < 6 months afterwards, which were associated with psychological distress.
Emotional Avoidance
Vos et al. [43] explored whether denial had an effect on mood and quality of life over time in lung cancer. The Denial of Cancer Interview (DCI) assessed levels of denial [70]. Moderate deniers compared to low deniers had significantly less anxiety and depression. Increasing deniers had more distress initially, which decreased later. In addition, moderate and increasing deniers had a better quality of life than low deniers.
Nipp et al. [44] used a cross-sectional study to evaluate the relationship between coping, mood, and quality of life in a large group (n = 350) of newly diagnosed participants with incurable lung and gastrointestinal cancers. Higher denial and self-blame (B = 0.580, SE = 0.1666, P < 0.001) were significantly correlated with higher depression and anxiety scores.
Although both Nipp [44] and Vos [43] employed samples of people newly diagnosed with advanced cancer, there are crucial differences in the definition and measurement of denial as well as the method used that limit comparison but may in part explain the differences in findings. For example, Vos [43] used a comprehensive 11-item scale the Denial of Cancer Interview (DCI) [71] based on Weisman and Hackett’s definition [72, 73]. Nine items were self-report and 2 were assessed by a clinician at 4 time points 8 weeks apart to provide longitudinal data. Nipp [44] only used a 2-item self-report subscale of the Brief COPE [38] to measure denial cross sectionally based on Lazarus and Folkman’s model of coping [1] and Carver and Scheier’s model of self-regulation [74].
Trevino et al. [39] investigated how a predominantly female (66%) sample of young adults [20–40 years] with heterogeneous cancers coped with a poor prognosis. ‘A factor analysis of subscales of the Brief COPE identified 6 coping factors of which Negative Expression was one. Denial, venting, and self-blame loaded onto the Negative Expression factor. After controlling for depression, anxiety, and other confounders coping by negative expression was directly related to grief and losses to cancer identified on the Prolonged Grief Disorder Scale (PG-12; [75].
Melanoma patients’ psychological adjustment, coping, and quality of life were examined over 2 years by Brown et al. [48]. Avoidant coping (distraction, eating, substances) had a significant negative effect on mood. In another study psychological adjustment to cancer as measured using the Psychological Adjustment to Cancer scale (PAC) [76] found people who isolated themselves and tried not to let people know about their cancer experienced significantly lower mood.
Qualitative Results
Study Characteristics
Six qualitative studies were identified. Of the total number of participants (n = 178), 136 had advanced cancer of which 109 were female. Characteristics of the included studies are summarised in Table 4. Different approaches to data analysis included phenomenology/interpretive phenomenological approach [56, 57], grounded theory [2, 58, 77], and qualitative descriptive thematic analysis [59].
Quality Assessment of Qualitative Studies
We present our quality assessment of included studies using the QualSyst tool [41] in Table 5. The quality of studies varied in relation to the amount of detail given of their sampling strategies. Four used purposive sampling [56, 57, 59, 77] and 2 adopted a consecutive approach [2, 58]. In 1 study, the researcher selected patients to participate [59], which could have introduced bias. Lam et al. [77] used a retrospective design that meant participants could have been subject to recall bias. Two studies in advanced breast cancer used participants already participating in longitudinal trials: 1 on effects of chemotherapy [56] and 1 on psychological distress following diagnosis [77].
Studies also lacked detail of time since diagnosis [2, 56, 57], and some patients may have been living with their cancer for longer and may have developed more adaptive coping strategies that included actively dealing with a problem by seeking information, enlisting instrumental support, problem solving and forward planning, positively reinterpreting difficulties, and willingly accepting experiences. The objectives of the studies and their design were well described, but scant detail was provided of the context and setting of the studies [2, 59, 77]. In addition, the majority of studies lacked a theoretical framework or disciplinary body of knowledge to inform their methods and research processes [2, 57–59, 77].
Most studies did not detail how findings may have been influenced by researcher bias apart from one in which the researcher selected patients [77]. Reflexivity of the researcher was only considered in two studies [57, 58] with consideration of how their researcher characteristics or methods could impact upon the research. Generally, a sufficient description of data analysis methods was provided, and the conclusions reached were supported by the results.
Thematic Synthesis
The aims of our thematic synthesis were first to explore participants’ coping strategies and identify EA and second to explore participants’ rationale for engaging in EA. EA was used to help mitigate the effects of cancer, and five themes were identified: [1] protection from distress, [2] preservation of identity, [3] maintenance of normality, [4] control of information, and [5] maintenance of optimism and hope.
Protection from Distress
People were anxious not to think or talk about their cancer [2, 56, 58, 59, 77] so used different cognitive and behavioural avoidance techniques to shield themselves from emotional distress. Suppression of thoughts was one technique to protect against experiencing uncomfortable or difficult thoughts.
I try not to think about it. It’s a way to protect myself that I refuse to think about it [56].
Distraction helped occupy peoples’ minds and provided temporary relief from negative thoughts, until they resurfaced:
I might just get in the car and do my shopping and it’s gone (thoughts) ….and I just put it away and I don’t want to think about it anymore until somethings else comes up [2].
Distancing helped people avoid social situations where they may be reminded of their illness. Patients with incurable lung cancer [59] who felt overwhelmed by their illness described distancing as a means of avoiding distress.
I’m afraid that I’ll go to pieces if I talk about my cancer with others [59].
By purposefully avoiding social contact, individuals side-stepped conversations that may require them to confront and express difficult emotions about their cancer.
Even though one participant recognised that avoiding her friends distressed her, she continued to do this:
I refuse to see any of my old friends, because I don’t want them to gossip about me and I don’t want to repeatedly answer their questions about cancer. This makes me sad [59].
Preservation of Identity
Participants with breast cancer [56] avoided talk about their cancer, as they suspected people would behave differently towards them if they knew of their diagnosis. One participant highlighted the reasons why:
I don’t want to tell anyone I’m like this. I don’t want to talk about it to strangers, cause I feel that people would start to feel sorry for me…..I don’t want any of that. I don’t think that I’ve changed that much as a person. I’m still the same person, even if I’ve got this disease. That’s probably why I don’t want to talk about it to anyone [56].
People did not wish their identity to be tainted by their cancer diagnosis, and they did not want to receive sympathy from strangers. Perceptions people with advanced cancer held about their illness challenged the way they thought about themselves and avoiding talking about it to strangers enabled some of the participants to preserve their identity so that their illness did not define them. Avoiding talking to people they knew maintained these relationships on their old terms, based on the person’s pre-cancer identity.
Maintaining Normality
One study investigated whether hospitalised advanced cancer patients wanted to talk about difficult emotions with their nurses [57]. Participants revealed that they preferred sometimes to talk about mundane things, or things that were part of everyday ‘normal’ life, rather than their illness:
I want to live as normally as possible. I want to talk about what I am doing at home. They (nurses) know much about me. I want to talk about ordinary things [57].
Crucially, the patient wants to be known as a person, valued as such, and with a life outside the hospital, not just as a cancer patient with specific needs.
Similar findings were reported in a study of how mixed cancer patients manage uncertainty. A participant was keen to circumscribe talk about her cancer so that it did not pervade her life:
I try to avoid talking about it as much as possible because you’ve got to focus on other things. And as much as friends and people say “how are you?” (I say) “I’m alright” …. you’re going, no, I don’t want to talk about this again [2].
Avoidance of talking about the disease not only helped the participant avoid potentially upsetting reminders but also helped to maintain and portray a semblance of normality with others.
Control of Information
Participants who were fearful of receiving negative information about their illness and prognosis sought to control information in various ways [2, 58]. A technique called ‘blunting’ [58] was used by women with gynaecological cancers to avoid exposure to negative information:
I have been non-interested in hearing about ovarian cancer stuff because I know how negative it is. So, I have not paid attention to it. I don’t particularly want to know anyway [58].
A participant who refused to listen to negative information likened the process to denial:
I think maybe it is part of the denial process in many ways; that you know you have got something really serious and you don’t really want to know how serious it is in some ways [58].
In a study of individuals with heterogenous cancers [2], participants were worried that too much information would make them feel worse, so tried to limit the amount of information they received:
I just want to know what I need to know, because I think for me too much information is not going to help me, it’s just going to make me more stressed [2].
and control the tenor of this:
I need to hear something that’s a bit confident, you know that gives me confidence, you know to keep going [2].
Maintenance of Optimism and Hope
Maintaining an optimistic outlook and not worrying about the future, despite being aware of their diagnosis, helped some people cope with the risks and realities of their illness [56–59].
Some engaged in positive denial whereby they counted on a return to their former health state before their cancer.
I feel very optimistic and very confident at this stage. I feel extremely positive myself and I think that makes a big difference as to how you handle things [58].
I don’t take the cancer seriously. I believe that I can be cured. I have not been thinking negative thoughts about illness. I try to be positive then it is much easier for me [57].
Maintenance of optimism and hope was nuanced across the studies as people adopted different strategies. Conscious denial [56, 59] occurred when people actively refused to think about or acknowledge their cancer, to reassure themselves they were going to be alright:
I try not to think about it. It’s a way to protect myself that I refuse to think about it. …If I start thinking about this illness, I’m lost and I haven’t got anything left in life than this awful disease [56].
Another participant draws on their imagination to deny the reality of their cancer and perhaps derives some relief from this:
I just try to not think about my illness. I tell myself I am okay, and my disease is gone [59].
Discussion
This systematic review of quantitative and qualitative research examined the nomenclature of EA in advanced cancer and the processes that might indicate EA, and explored associations between EA and psychological distress and reasons for engagement in EA. EA is a broad term that covers a variety of coping strategies in the psycho-oncological literature [19, 20]. We have defined and classified the terminology used to describe EA; this covers cognitive, behavioural, and emotional avoidance, and includes the term ‘avoidant coping’ [54]. Although a range of terms are used for EA, no specific scales are used to measure it. EA in advanced cancer patients may be associated with an exacerbation of psychological distress and behaviours which perpetuate emotional problems, thus preventing psychological adjustment, although in a small number of people, it may be helpful in the short term.
Association Between EA and Psychological Distress
There is evidence of an association between EA and psychological distress. However, as no studies in advanced cancer have specifically examined EA as a primary outcome, definitive conclusions need to be treated with caution. There are no standardised methods to study EA in advanced cancer. Trials to date cover a range of cancers, use a range of methodologies, and lack standardised outcomes. Furthermore, despite the research being rated of good quality due to a low risk of bias, limitations included a lack of detailed reporting of information, a lack of variance and controls for confounders, and research processes that were not always based on a theoretical framework or a body of knowledge. Measures to assess coping were also often not complete [44–46, 49, 51, 52, 60]. Although existing measures have been adapted for assessing EA, only the Brief COPE has had its psychometric properties evaluated in incurable cancer [63]. Livneh [22] suggests that despite an association between avoidant coping and poorer psychosocial adaptation in chronic illness (including cancer), studies need to be strengthened with respect to reporting illness severity and sociodemographic details, and using psychometrically tested scales [22].
The relationship between the cancer type, stage, and EA and its impact on mood is uncertain [39, 44–47, 60]. In two studies, it was suggested that EA is the mediator between anxiety and distress [49, 50]. By contrast, EA did not appear detrimental as a short-term strategy [50]. Differences in EA were found which may be accounted for by tumour groups. Higher levels of distress are present in breast, gynaecological, prostate, and head and neck cancers [78]. High levels of denial (emotional avoidance) [43, 44] are associated with increased anxiety and depression, and symptoms of distress [45, 47] and grief [39], as well as a poorer quality of life [44]. By contrast, Vos et al. [43] found that as denial increased distress decreased [43].
A more recent study found that older patients used more denial than younger patients and denial was weakly correlated with problem-based coping [79]. These coping strategies appear contradictory and imply people may fluctute in their choice of coping strategy or combine contrasting strategies. Overall, denial appears to be associated with increased distress, but it is difficult to be sure of the direction of this relationship.
Reasons Why People with Advanced Cancer Engage in EA
Numerous factors affect the way people cope with advanced cancer: cancer type; extent of disease; physical symptoms and function; emotional well-being; available resources; and environment [80]. Progression of disease and its diagnosis and treatment can cause repetitive and cumulative trauma leading to anxiety, depression, and post-traumatic stress disorder [81, 82]. EA may be used to reduce or regulate distress experienced in cancer particularly when a person feels overwhelmed and not able to cope [83]. EA can be adaptive if used in the short term to give people some respite from distress and help them to gather resources [84]. Continued avoidance of difficult experiences rather than direct contact, however, is maladaptive, if used over time, as it requires a large allocation of resources [14] and impairs functioning [85]. Acceptance of experiences as they occur without defence is more adaptive as functioning is preserved.
A review found disengagement and avoidance helped people to minimise cancer; control the illness experience; express emotions; and create meaning [86]. Pooling of qualitative data from our review found similar results, as EA was primarily used to protect people from distress and having to confront or express difficult emotions [2, 56, 58, 59, 77]. Avoiding communicating about cancer as well as reminders of it helped protect people’s previous relationships and preserve identity [56], as well as maintain normality [2, 57]. A reluctance to face difficult emotions meant people tried to control the information they received to avoid exposure to negative information [2, 58]. Positive denial enabled people to only pay attention to positive information and ignore any negative information about the seriousness of cancer or extent of disease which helped them to maintain hope and optimism about the future [56–59]. This bears similarities to elements of adaptive coping in the oncology literature when people positively reframe their thoughts by looking for something good in what is happening to help them cope which can enhance mood and quality of life [87].
Strengths and Limitations
This is the first systematic review to describe EA in advanced cancer and suggests an association between EA and psychological distress. Although the literature search was completed in October 2019 an updated search only revealed 1 more relevant paper [79]. Due to the complex nature of the topic, both quantitative and qualitative data were synthesised to provide an exhaustive account of EA in advanced cancer. Our use of broad search terms covering different types of cognitive, behavioural, and emotional avoidance has contributed to an elucidation of EA in the advanced cancer population. However, this review only included peer-reviewed published papers in English. Grey literature may have revealed additional findings on this topic.
A limitation of the work in this field is the heterogeneity of constructs and lack of a clear definition of EA in advanced cancer making the comparison of studies difficult.
Clinical and Research Implications
In the clinical setting, interventions are needed to assist advanced cancer patients to be more willing to accept uncomfortable or difficult feelings. Conventional therapies such as cognitive behavioural therapy have struggled to address patients’ anxieties because they relate to numerous rational stressors experienced at this stage [88]. ACT states that some psychological pain is inevitable in cancer and forms part of the experience of being human which cannot be avoided, but the suffering that may result from avoiding experiences is optional and can be addressed [89, 90].
ACT [28] focuses on the relationship between behaviours and all three types of avoidance, (cognitive, emotional, and behavioural), and may be a particularly well-suited intervention in advanced cancer. Research on the implications of EA in the aetiology and maintenance of diverse forms of psychopathology has grown considerably over the last 10 years, yet the contribution of EA to cancer-related distress has received very little attention in the advanced cancer population. A reason for this could be due to a lack of a comprehensive and standardised definition of EA in cancer.
We therefore define EA as behaviours whose function is to reduce the person’s contact with unwanted internal experiences. The distortion of facts such as wishful thinking, denial, and blunting is incorporated within this definition as their function is to alter the internal experience the person is in contact with, but EA does not incorporate self-blame or venting as their function is not to avoid unwanted internal experiences.
Greater clinical awareness of the complexity of EA behaviours is needed, and clinicians and researchers need to define EA precisely and be aware of its function in the short and long term.
The Acceptance and Action Questionnaire (AAQ) [30] and the (AAQ-II) [91] have traditionally been used to assess EA amongst cancer survivors [34, 92–96], but these have not been validated in advanced cancer. The AAQ-II [91] is limited, because it does not solely measure EA but measures psychological inflexibility instead which includes acceptance as well as EA [91, 97, 98]. The Multi-Dimensional Experiential Avoidance Questionnaire (MEAQ) [99] has been developed as a more comprehensive measure of EA, designed to assess six different elements of EA [100, 101]. However, future research needs to test and validate this measure in an advanced cancer population.
Furthermore, future qualitative research focused on exploring EA can build on these findings and explore the nuances of how people engage in EA and the perceived impact of this.
Conclusion
People with advanced cancer engage in EA which may increase psychological distress if used rigidly and repeatedly [102]. Qualitative data suggests EA may be beneficial in the short term to those who feel overwhelmed, as it helps people continue to function through control of information, maintenance of normality, and an optimistic outlook, but in the longer term, it can impair function and limit engagement in life. A greater awareness of EA perpetuating emotional problems and preventing psychological adjustment is needed amongst clinicians.
Future work into EA should define the advanced cancer diagnosis and the time from diagnosis, and assess the type of EA with a standardised measure to enable treatment to target elements of EA.
References
Lazarus RS, Folkman S. Stress, appraisal, and coping: Springer publishing company; 1984.
Lobb EA, Lacey J, Kearsley J, Liauw W, White L, Hosie A. Living with advanced cancer and an uncertain disease trajectory: an emerging patient population in palliative care? BMJ Support Palliat Care. 2015;5(4):352–7.
Mitchell AJ, Chan M, Bhatti H, Halton M, Grassi L, Johansen C, et al. Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: a meta-analysis of 94 interview-based studies. Lancet Oncol. 2011;12(2):160–74.
Miovic M, Block S. Psychiatric disorders in advanced cancer. Cancer. 2007;110(8):1665–76.
Holland JC, Alici Y. Management of distress in cancer patients. J Support Oncol. 2010;8(1):4.
Hopkins K, Tookman A. Rehabilitation and specialist palliative care. Int J Palliat Nurs. 2000;6(3):123–30.
Colosimo K, Nissim R, Pos AE, Hales S, Zimmermann C, Rodin G. “Double awareness” in psychotherapy for patients living with advanced cancer. J Psychother Integr. 2018;28(2):125.
Roth S, Cohen LJ. Approach, avoidance, and coping with stress. Am Psychol. 1986;41(7):813.
Watson M, Law MG, Santos Md, Greer S, Baruch J, Bliss J. The Mini-MAC: further development of the mental adjustment to cancer scale. J Psychosoc Oncol. 1994;12(3):33–46.
Lepore SJ, Helgeson VS. Social constraints, intrusive thoughts, and mental health. J Soc Clin Psychol. 1998;17(1).
Freud S. Remembering, repeating, and working through. Standard edition (Vol. 12). London: Hogarth Pres. 1914.
Chawla N, Ostafin B. Experiential avoidance as a functional dimensional approach to psychopathology: An empirical review. J Clin Psychol. 2007;63(9):871–90.
Foa EB, Steketee G, Young MC. Agoraphobia: phenomenological aspects, associated characteristics, and theoretical considerations. Clin Psychol Rev. 1984;4(4):431–57.
Kashdan TB, Barrios V, Forsyth JP, Steger MF. Experiential avoidance as a generalized psychological vulnerability: comparisons with coping and emotion regulation strategies. Behav Res Ther. 2006;44(9):1301–20.
Bardeen JR, Fergus TA, Orcutt HK. Experiential avoidance as a moderator of the relationship between anxiety sensitivity and perceived stress. Behav Ther. 2013;44(3):459–69.
Mahoney CT, Segal DL, Coolidge FL. Anxiety sensitivity, experiential avoidance, and mindfulness among younger and older adults: age differences in risk factors for anxiety symptoms. Int J Aging Hum Dev. 2015;81(4):217–40.
Eustis EH, Cardona N, Nauphal M, Sauer-Zavala S, Rosellini AJ, Farchione TJ, et al. Experiential avoidance as a mechanism of change across cognitive-behavioral therapy in a sample of participants with heterogeneous anxiety disorders. Cogn Ther Res. 2020;44(2):275–86.
Wenzlaff RM, Wegner DM. Thought suppression. Annu Rev Psychol. 2000;51(1):59–91.
Hayes SC, Wilson KG, Gifford EV, Follette VM, Strosahl K. Experiential avoidance and behavioral disorders: a functional dimensional approach to diagnosis and treatment. J Consult Clin Psychol. 1996;64(6):1152.
Dunkel-Schetter C, Feinstein LG, Taylor SE, Falke RL. Patterns of coping with cancer. 1999.
Holahan CJ, Moos RH, Holahan CK, Brennan PL, Schutte KK. Stress generation, avoidance coping, and depressive symptoms: a 10-year model. J Consult Clin Psychol. 2005;73(4):658.
Livneh H. The use of generic avoidant coping scales for psychosocial adaptation to chronic illness and disability: a systematic review. Health psychology open. 2019;6(2):2055102919891396.
Greer S, Morris T, Pettingale KW. Psychological response to breast cancer: effect on outcome. The Lancet. 1979;314(8146):785–7.
Horowitz M, Wilner N, Alvarez W. Impact of event scale: a measure of subjective stress. Psychosom Med. 1979;41(3):209–18.
Borkovec TD, Alcaine O, Behar E. Avoidance theory of worry and generalized anxiety disorder. Generalized anxiety disorder: advances in research and practice. 2004;2004:77–108.
Folkman S, Lazarus RS. If it changes it must be a process: study of emotion and coping during three stages of a college examination. J Pers Soc Psychol. 1985;48(1):150.
Carver CS, Scheier MF, Weintraub JK. Assessing coping strategies: a theoretically based approach. J Pers Soc Psychol. 1989;56(2):267.
González-Fernández S, Fernández-Rodríguez C. Acceptance and commitment therapy in cancer: review of applications and findings. Behav Med. 2019;45(3):255–69.
Batten S. Essentials of acceptance and commitment therapy: Sage Publications; 2011.
Hayes SC, Strosahl K, Wilson KG, Bissett RT, Pistorello J, Toarmino D, et al. Measuring experiential avoidance: a preliminary test of a working model. The psychological record. 2004;54(4):553–78.
Barlow DH. Anxiety and its disorders: the nature and treatment of anxiety and panic. Guilford press; 2004.
Ottenbreit ND, Dobson KS. Avoidance and depression: the construction of the Cognitive-Behavioral Avoidance Scale. Behav Res Ther. 2004;42(3):293–313.
Deimling GT, Wagner LJ, Bowman KF, Sterns S, Kercher K, Kahana B. Coping among older‐adult, long‐term cancer survivors. Psycho‐Oncology: J Psychol, Social and Behav Dimensions Cancer. 2006;15(2):143–59.
Low J, Davis S, Drake R, King M, Tookman A, Turner K, et al. The role of acceptance in rehabilitation in life-threatening illness. J Pain Symptom Manage. 2012;43(1):20–8.
O’Brien CW, Moorey S. Outlook and adaptation in advanced cancer: a systematic review. Psychooncology. 2010;19(12):1239–50.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. 2010;8(5):336–41.
Biggs A, Brough P, Drummond S. Lazarus and Folkman’s psychological stress and coping theory. The handbook of stress and health: a guide to research and practice. 2017:351–64.
Carver CS. You want to measure coping but your protocol’s too long: consider the brief COPE. Int J Behav Med. 1997;4(1):92.
Trevino KM, Maciejewski PK, Fasciano K, Greer J, Partridge A, Kacel EL, et al. Coping and psychological distress in young adults with advanced cancer. J Support Oncol. 2012;10(3):124–30.
Cella DF, Tulsky DS, Gray G, Sarafian B, Linn E, Bonomi A, et al. The Functional Assessment of Cancer Therapy scale: development and validation of the general measure. J Clin Oncol. 1993;11(3):570–9.
Kmet LM, Cook LS, Lee RC. Standard quality assessment criteria for evaluating primary research papers from a variety of fields. 2004.
Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008;8(1):45.
Vos MS, Putter H, van Houwelingen HC, de Haes HC. Denial and social and emotional outcomes in lung cancer patients: the protective effect of denial. Lung Cancer. 2011;72(1):119–24.
Nipp RD, El-Jawahri A, Fishbein JN, Eusebio J, Stagl JM, Gallagher ER, et al. The relationship between coping strategies, quality of life, and mood in patients with incurable cancer. Cancer. 2016;122(13):2110–6.
Kershaw T, Northouse L, Kritpracha C, Schafenacker A, Mood D. Coping strategies and quality of life in women with advanced breast cancer and their family caregivers. Psychol Health. 2004;19(2):139–55.
Sherman AC, Simonton S, Adams DC, Vural E, Hanna E. Coping with head and neck cancer during different phases of treatment. Head and Neck. 2000;22(8):787–93.
Sumpio C, Jeon S, Northouse LL, Knobf MT. Optimism, symptom distress, illness appraisal, and coping in patients with advanced-stage cancer diagnoses undergoing chemotherapy treatment. Oncol Nurs Forum. 2017;44(3):384–92.
Brown JE, King MT, Butow PN, Dunn SM, Coates AS. Patterns over time in quality of life, coping and psychological adjustment in late stage melanoma patients: an application of multilevel models. Quality of Life Research: An International Journal of Quality of Life Aspects of Treatment, Care & Rehabilitation. 2000;9(1):75.
Couper JW, Love AW, Duchesne GM, Bloch S, Macvean M, Dunai JV, et al. Predictors of psychosocial distress 12 months after diagnosis with early and advanced prostate cancer. The Medical journal of Australia. 2010;193(5 Suppl).
Manne S, Glassman M, Du Hamel K. Intrusion, avoidance, and psychological distress among individuals with cancer. Psychosom Med. 2001;63(4):658–67.
Lutgendorf SK, Anderson B, Ullrich P, Johnsen EL, Buller RE, Sood AK, et al. Quality of life and mood in women with gynecologic cancer: a one year prospective study. Cancer. 2002;94(1):131–40.
Costanzo ES, Lutgendorf SK, Rothrock NE, Anderson B. Coping and quality of life among women extensively treated for gynecologic cancer. Psycho Oncology. 2006;15(2):132–42.
De Faye BJ, Wilson KG, Chater S, Viola RA, Hall P. Stress and coping with advanced cancer. Palliat Support Care. 2006;4(3):239–49.
Karekla M, Panayiotou G. Coping and experiential avoidance: unique or overlapping constructs? J Behav Ther Exp Psychiatry. 2011;42(2):163–70.
Else-Quest NM, LoConte NK, Schiller JH, Hyde JS. Perceived stigma, self-blame, and adjustment among lung, breast and prostate cancer patients. Psychol Health. 2009;24(8):949–64.
Luoma ML, Hakamies-Blomqvist L. The meaning of quality of life in patients being treated for advanced breast cancer: a qualitative study. Psychooncology. 2004;13(10):729–39.
Kvale K. Do cancer patients always want to talk about difficult emotions? A qualitative study of cancer inpatients communication needs. Eur J Oncol Nurs. 2007;11(4):320–7.
Power J, Brown L, Ritvo P. A qualitative study examining psychosocial distress, coping, and social support across the stages and phases of epithelial ovarian cancer. Health Care Women Int. 2008;29(4):366–83.
Liao YC, Liao WY, Sun JL, Ko JC, Yu CJ. Psychological distress and coping strategies among women with incurable lung cancer: a qualitative study. Support Care Cancer. 2018;26(3):989–96.
Van Laarhoven HWM, Schilderman J, Bleijenberg G, Donders R, Vissers KC, Verhagen CAHHVM, et al. Coping, quality of life, depression, and hopelessness in cancer patients in a curative and palliative, end-of-life care setting. Cancer Nursing. 2011;34(4):302–14.
Stone AA, Neale JM. New measure of daily coping: development and preliminary results. J Pers Soc Psychol. 1984;46(4):892.
Cheng C, Hui W-M, Lam S-K. Perceptual style and behavioral pattern of individuals with functional gastrointestinal disorders. Health Psychol. 2000;19(2):146.
Hagan TL, Fishbein JN, Nipp RD, Jacobs JM, Traeger L, Irwin KE, et al. Coping in patients with incurable lung and gastrointestinal cancers: a validation study of the Brief COPE. J Pain Symptom Manage. 2017;53(1):131–8.
McNair DM. Manual profile of mood states: Educational & Industrial testing service; 1971.
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–70.
Derogatis LR, Spencer P. Brief symptom inventory: BSI: Pearson Upper Saddle River, NJ; 1993.
Beck AT, Steer RA, Carbin MG. Psychometric properties of the Beck Depression Inventory: twenty-five years of evaluation. Clin Psychol Rev. 1988;8(1):77–100.
Ware Jr JE, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Medical Care. 1996:220–33.
Sullivan GM, Feinn R. Using effect size—or why the P value is not enough. J Grad Med Educ. 2012;4(3):279.
Vos MS, de JCJM. Denial in cancer patients, an explorative review. Psycho-Oncology. 2007;16(1):12.
Vos MS, Putter H, Leurs A, Rooijmans HG, de Haes HC, van Houwelingen HC. The denial of cancer interview: development and first assessment of psychometric properties in lung cancer patients. Patient Educ Couns. 2007;67(1–2):224–34.
Weisman AD, Sobel HJ. Coping with cancer through self-instruction: a hypothesis. J Hum Stress. 1979;5(1):3–8.
Hackett T, Cassem N. Development of a quantitative rating scale to assess denial. J Psychosom Res. 1974;18(2):93–100.
Carver CS, Scheier M. Principles of self-regulation: action and emotion. The Guilford Press; 1990.
Prigerson HG, Horowitz MJ, Jacobs SC, Parkes CM, Aslan M, Goodkin K, et al. Prolonged grief disorder: psychometric validation of criteria proposed for DSM-V and ICD-11. PLoS Med. 2009;6(8): e1000121.
Dunn SM, Welch GW, Butow PN, Coates AS. Refining the measurement of psychological adjustment in cancer. Aust J Psychol. 1997;49(3):144–51.
Lam WWT, Yoon SW, Sze WK, Ng AWY, Soong I, Kwong A, et al. Comparing the meanings of living with advanced breast cancer between women resilient to distress and women with persistent distress: a qualitative study. Psycho Oncology. 2017;26(2):255–61.
Zabora J, BrintzenhofeSzoc K, Curbow B, Hooker C, Piantadosi S. The prevalence of psychological distress by cancer site. Psycho‐Oncology. 2001;10(1):19–28.
Jabbarian LJ, Korfage IJ, Červ B, van Delden JJ, Deliens L, Miccinesi G, et al. Coping strategies of patients with advanced lung or colorectal cancer in six European countries: insights from the ACTION Study. Psychooncology. 2020;29(2):347–55.
Greer JA, Applebaum AJ, Jacobsen JC, Temel JS, Jackson VA. Understanding and addressing the role of coping in palliative care for patients with advanced cancer. J Clin Oncol. 2020;38(9):915–25.
Yehuda R. Post-traumatic stress disorder. N Engl J Med. 2002;346(2):108–14.
Rodin G. From evidence to implementation: the global challenge for psychosocial oncology. Psychooncology. 2018;27(10):2310–6.
Skinner EA, Edge K, Altman J, Sherwood H. Searching for the structure of coping: a review and critique of category systems for classifying ways of coping. Psychol Bull. 2003;129(2):216.
Suls J, Fletcher B. The relative efficacy of avoidant and nonavoidant coping strategies: a meta-analysis. Health Psychol. 1985;4(3):249.
Fernández-Rodríguez C, Paz-Caballero D, González-Fernández S, Pérez-Álvarez M. Activation vs. experiential avoidance as a transdiagnostic condition of emotional distress: an empirical study. Front Psychol. 2018:1618.
Thomsen TG, Rydahl-Hansen S, Wagner L. A review of potential factors relevant to coping in patients with advanced cancer. J Clin Nurs. 2010;19(23–24):3410–26.
Nipp RD, Greer JA, El-Jawahri A, Moran SM, Traeger L, Jacobs JM, et al. Coping and prognostic awareness in patients with advanced cancer. J Clin Oncol. 2017;35(22):2551.
Greer JA, Park ER, Prigerson HG, Safren SA. Tailoring cognitive-behavioral therapy to treat anxiety comorbid with advanced cancer. J Cogn Psychother. 2010;24(4):294–313.
Hayes SC, Strosahl KD, Wilson KG. Acceptance and commitment therapy: the process and practice of mindful change: Guilford Press; 2011.
Strosahl K, Kseib K. 'Pain is inevitable, but suffering is optional'. PSYCHOLOGIST. 2016 Aug 1;29(8):632-3.
Bond FW, Hayes SC, Baer RA, Carpenter KM, Guenole N, Orcutt HK, et al. Preliminary psychometric properties of the Acceptance and Action Questionnaire–II: a revised measure of psychological inflexibility and experiential avoidance. Behav Ther. 2011;42(4):676–88.
Feros DL, Lane L, Ciarrochi J, Blackledge JT. Acceptance and Commitment Therapy (ACT) for improving the lives of cancer patients: a preliminary study. Psychooncology. 2013;22(2):459–64.
Hawkes AL, Patrao TA, Baade P, Lynch BM, Courneya KS. Predictors of physical activity in colorectal cancer survivors after participation in a telephone-delivered multiple health behavior change intervention. J Cancer Surviv. 2015;9(1):40–9.
Arch JJ, Mitchell JL. An Acceptance and Commitment Therapy (ACT) group intervention for cancer survivors experiencing anxiety at re-entry. Psychooncology. 2016;25(5):610–5.
Swash B, Bramwell R, Hulbert-Williams NJ. Unmet psychosocial supportive care needs and psychological distress in haematological cancer survivors: the moderating role of psychological flexibility. J Contextual Behav Sci. 2017;6(2):187–94.
Han Y, Hu D, Liu Y, Lu C, Luo Z, Zhao J, et al. Coping styles and social support among depressed Chinese family caregivers of patients with esophageal cancer. Eur J Oncol Nurs. 2014;18(6):571.
Wolgast M. What does the Acceptance and Action Questionnaire (AAQ-II) really measure? Behav Ther. 2014;45(6):831–9.
Schaeuffele C, Knaevelsrud C, Renneberg B, Boettcher J. Psychometric properties of the German Brief Experiential Avoidance Questionnaire (BEAQ). Assessment. 2021:10731911211010955.
Gámez W, Chmielewski M, Kotov R, Ruggero C, Watson D. Development of a measure of experiential avoidance: the Multidimensional Experiential Avoidance Questionnaire. Psychol Assess. 2011;23(3):692.
Gámez W, Chmielewski M, Kotov R, Ruggero C, Suzuki N, Watson D. The brief experiential avoidance questionnaire: development and initial validation. Psychol Assess. 2014;26(1):35.
Vázquez-Morejón Jiménez R, León Rubio JM, Martín Rodríguez A, Vázquez Morejón AJ. Validation of a Spanish version of the Brief Experiential Avoidance Questionnaire (BEAQ) in clinical population. Psicothema. 2019.
Hayes-Skelton SA, Eustis EH. Experiential avoidance. 2020.
Weisman AD, Worden JW. The existential plight in cancer: Significance of the first 100 days. Int J Psychiatry Med. 1977 Mar;7(1):1–5.
Priestman TJ, Baum M. Evaluation of quality of life in patients receiving treatment for advanced breast cancer. Lancet. 1976 Apr 24;307(7965):899–901.
Hürny C, Bernhard J, Joss R, Schatzmann E, Cavalli F, Brunner K, Alberto P, Senn HJ, Metzger U. “Fatigue and malaise” as a quality-of-life indicator in small-cell lung cancer patients. Support Care Cancer. 1993 Nov;1(6):316–20.
Watson M, Law MG, Santos MD, Greer S, Baruch J, Bliss J. The Mini-MAC: further development of the mental adjustment to cancer scale. J Psychosoc Oncol. 1994 Oct 31;12(3):33–46.
Ware Jr JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection. Med Care. 1992 Jun 1:473–83.
Derogatis LR, Melisaratos N. The brief symptom inventory: an introductory report. Psychol Med. 1983 Aug;13(3):595–605.
Beck AT, Ward C, Mendelson M, Mock J, Erbaugh JJ. Beck depression inventory (BDI). Arch Gen Psychiatry. 1961 Jun;4(6):561–71.
Veit CT, Ware JE. Mental health inventory. Psychol Assess. 1983.
Cohen SR, Mount BM, Strobel MG, Bui F. The McGill Quality of Life Questionnaire: a measure of quality of life appropriate for people with advanced disease. A preliminary study of validity and acceptability. Palliat Med. 1995 Jul;9(3):207–19.
Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, Filiberti A, Flechtner H, Fleishman SB, de Haes JC, Kaasa S. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993 Mar 3;85(5):365–76.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Statement Regarding Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Statement Including Informed Consent
Informed consent was obtained from all individual participants included in this study.
Statement Regarding the Welfare of Animals, Studies with No Animal Subjects
This article does not contain any studies with animals performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Davis, S., Serfaty, M., Low, J. et al. Experiential Avoidance in Advanced Cancer: a Mixed-Methods Systematic Review. Int.J. Behav. Med. 30, 585–604 (2023). https://doi.org/10.1007/s12529-022-10131-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12529-022-10131-4