
Abstract
Health inequalities still exist between people with a low socioeconomic status (SES) and people with a high SES. Combined lifestyle interventions (CLIs) could benefit the health of people with a low SES. However, it is unclear which CLI elements are effective for this group. Therefore, this study aimed to determine the effective elements X‑Fittt 2.0, a CLI for people with a low SES. Nine professionals and one participant of X‑Fittt 2.0 participated in a concept mapping (CM) process to develop an overview of the effective elements of X‑Fittt 2.0. CM consists of six steps: preparing, brainstorming, clustering, scoring, analysing, and discussing and interpreting. This process resulted in 72 effective elements, grouped in nine clusters, focused on monitoring (12), internal (7) and external (4) collaborations, structure and guidance (10), agreements with participants (5), sports options in the first 12 weeks (10), the sports environment (10), recruitment strategies (5) and the preconditions for X‑Fittt 2.0 (9). These results provide a valuable first overview of effective elements of CLIs for people with a low SES.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
As in the rest of the world, Dutch overweight (50%) and obesity (15%) levels are high and it is expected that they will rise, especially among those with a low socioeconomic status (SES) [1, 2]. While various interventions are used to decrease health inequalities between people with a low and a high SES, recent figures show that these inequalities are still a major concern with regard to public health. People with a high SES live approximately seven years longer than people with low SES, and also enjoy 18 more years of perceived good health as compared to people with a low SES [1].
These health inequalities may be caused by differences in lifestyle, such as physical activity (PA) and nutrition, between low and high SES citizens [3]. Regular PA has beneficial effects on health and in preventing various chronic diseases, such as diabetes, cancer, and cardiovascular disease [4, 5]. An opportunity to stimulate a healthy lifestyle lies in developing and implementing health improving initiatives, such as combined lifestyle interventions (CLIs) [6].
CLIs focus on improving health by targeting multiple health behaviours simultaneously (e.g., PA and diet). As a multi-pronged approach, CLIs offer intensive guidance with health professionals from different sectors, such as the sports sector and primary care [7]. Therefore, CLIs are considered to be more successful than single-behaviour and single-sector interventions [8, 9]. To date, however, insight is still lacking into which elements make CLIs effective for citizens with a low SES [10].
Researchers use different concepts to refer to effective elements, such as active ingredients [11, 12], core components [13], effective principles (translated from Dutch) [14], good practice characteristics [15], and principles for action [16]. We based our definition of effective elements on the definition of the Dutch National Institute for Public Health and the Environment:
Effective elements are the elements that make an intervention successful. These elements should be included when the intervention is implemented [17].
Effectivity is more likely to be caused by multiple elements in combination, rather than by one element alone [18].
Despite the increasing attention to CLIs, previous research has not yet focused on effective elements of CLIs for citizens with a low SES specifically. Earlier research identified the most important effective elements of CLIs for the general population [19] and the preconditions for lifestyle interventions—not CLIs—for citizens with a low SES [20]. Furthermore, for the general population, the good practice characteristics of diet and PA interventions have been researched [15], and the barriers and facilitators for adhering to PA programmes have been identified [21]—not CLIs. In practice, it appears that relatively few citizens with low a SES are reached by the current supply of CLIs [22, 23], which may indicate that CLIs do not sufficiently connect to target groups with low SES. Therefore, insights into the effective elements of CLIs for citizens with a low SES contribute to improving existing and to designing new CLIs to establish long-term health behaviour change among citizens with a low SES [24]. In this study we focus on the CLI X‑Fittt 2.0, by addressing the following research question: what are the effective elements of X‑Fittt 2.0?
Methods
Study case
We have focused this study on X‑Fittt 2.0, which is the first Dutch CLI specifically developed for citizens with a low SES [25]. X‑Fittt 2.0 is being carried out in Arnhem, a municipality in the Netherlands. The municipality (Sports Service Arnhem) and a health insurer mutually funded X‑Fittt 2.0, which focuses on people with a minimum income or lower [26]. X‑Fittt 2.0 runs for two years, and starts with a 12-week intensive programme, consisting of: two weekly group sports sessions with a sports coach, one individual weekly sports session, dietary advice and monitoring by a dietitian, and four hours of lifestyle coaching by a lifestyle coach. After these twelve weeks, participants are encouraged to maintain the healthy lifestyle by receiving a total of six hours lifestyle coaching during the remainder of the programme (approximately 21 months). The first results of X‑Fittt 2.0 indicate that the programme has a positive impact on the participants in Arnhem, at least in the first twelve weeks, for instance in reducing weight and fat percentage, and improvements in quality of life and societal participation [26].
Methodology
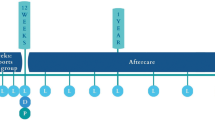
We used concept mapping (CM) to develop a comprehensive overview of the effective elements of X‑Fittt 2.0 [27]. CM is a type of structured conceptualisation, which can be used for groups. CM consists of six steps: preparing, brainstorming, clustering, scoring, analysing, and interpreting (Fig. 1).

Flow chart of the CM process to unravel the effective elements of X‑Fittt 2.0, based on Kane & Trochim (2007) [27]. For every step, the number of respondents and their professions are indicated
Step 1: preparing
We invited 22 people via email to participate in the CM process: all 17 public health practitioners of X‑Fittt 2.0 (Fig. 1) and five citizens with a low SES who participated in X‑Fittt 2.0 in Arnhem (the particular citizens were suggested by the lifestyle coaches). Eventually, 11 respondents (ten public health practitioners, one participant) agreed to participate (Fig. 1). The others did not answer the email invitation nor the reminder (n = 6), or did not want to participate for various reasons (n = 5).
As preparation, the respondents received a detailed research guide that described the steps of the CM process and our definition of effective elements, adapted for X‑Fittt 2.0:
By effective elements we mean the elements of X‑Fittt 2.0 that should definitely be included when implementing X‑Fittt 2.0 in another municipality. In other words, which elements of X‑Fittt 2.0 are necessary to make the programme a success?
Step 2: brainstorming
We conducted the brainstorming via an online form that was open for four weeks. We asked the respondents to write down everything they perceived to be an effective element of X‑Fittt 2.0. The respondents (9 public health practitioners, 1 participant) had to be as detailed and clear as possible, by using only short phrases or key words. Respondents received a reminder when they had not filled out the form after two weeks. Eventually, ten respondents (Fig. 1) filled out the form and came up with 135 effective elements.
Step 3 and 4: clustering and scoring
Two researchers deduplicated the 135 listed effective elements to 90 elements. We numbered each unique effective element and printed them on small cards. We combined the small cards with effective elements in one package with an instruction letter and twenty empty A4 sheets, and sent the packages to all respondents. The instruction letter explained that the respondents first had to cluster all effective elements using the small cards and empty A4 sheets. Instructions for clustering were:
-
a)
to cluster the elements in a way that made sense to them,
-
b)
to use every element only once,
-
c)
to cluster more than one element per cluster,
-
d)
to form more than one cluster, and
-
e)
to cluster all elements.
Respondents were requested to stick every cluster of effective elements to a separate A4 sheet, and to label each cluster. Finally, we asked respondents to score all effective elements as to importance using a scoring sheet containing a Likert-like scale (1 = not important at all, 5 = very important) for each element. Eventually, nine respondents (8 public health practitioners, 1 participant) sent the A4 sheets and the scorings back to us (Fig. 1).
Step 5: analysing
For the analysis, we used the steps as described by Kane & Trochim (2007) [27]. First, we entered the complete list of effective elements, and all clusters and scores received from the respondents into the Concept Systems Global MAX (CS Global MAX) software [28]. Then, the software created a point map using multidimensional scaling, locating every effective element as an individual point on a map. Elements closer to each other were more likely to be sorted together. After that, hierarchical cluster analysis grouped the individual elements into clusters of similar elements. Two researchers reduced the number of clusters from 20 to 4 within the software, evaluating every next merge of two clusters. Bridging scores per cluster indicated the level of homogeneity for each cluster (0 = homogenic, 1 = heterogenic). When a newly formed cluster after merging two clusters resulted in a too heterogenic cluster, indicating no more coherence, we stopped merging and reached the final cluster solution of nine 9 clusters. We then used the respondents’ importance scores to develop a cluster rating map, showing mean importance per cluster, and labelled each cluster (Fig. 2).

Cluster rating map as developed using Concept Systems Global MAX [28]
Step 6: discussing and interpreting
We invited the respondents for a two-hour group meeting, in which eventually four public health practitioners participated (Fig. 1). As preparation, they received the point map, a list of all effective elements as clustered in the final cluster solution, and the cluster rating map one week before the group meeting. Respondents discussed every individual cluster to determine whether there were any deviating effective elements, whether there was something missing, and whether they were correctly labelled. During this discussion, clusters were merged, added, and reformulated, and elements were moved, reformulated, removed, merged, and added. The group meeting has been recorded and the recording has been used in the processing of the results. After the group meeting, the researchers reformulated the cluster labels into guidelines that could be used in practice.
Results
After the analysis, it appeared that the clusters ‘sports options’ and ‘preconditions for X‑Fittt 2.0’ were least important, and that the clusters ‘structured monitoring’, ‘multidisciplinary collaboration’, and ‘integral approach’ were most important (Fig. 2). Elements that scored lowest on importance (3.11 out of 5) were element 3: ‘List to fill out all information from the physical test for left and right side of the body’ and element 18: ‘One sports coach and one intern on a group of 12 participants during the sports sessions (2 sets of eyes are better than 1)’ (Table 1). The highest importance score (4.89 out of 5) was given to element 41: ‘Combined lifestyle intervention: approach with sports/physical activity, diet, physical checks by physiotherapist’.
During the group meeting, the clusters of effective elements have changed due to merging, adding, and reformulating clusters, and moving, reformulating, removing, merging, and adding elements (Appendix, Table 2).
Adaptations to the clusters
The clusters ‘structured monitoring’ and ‘measurement of progression’ were merged into one cluster labelled ‘monitoring’, as these two clusters covered the same kind of elements. The respondents also created a new cluster ‘recruitment’ with five of the effective elements, to stress the importance of attention for recruitment in X‑Fittt 2.0.
The respondents relabelled some clusters when the label did not represent the content of the cluster. For instance, the cluster ‘multidisciplinary collaboration’ was relabelled ‘internal multidisciplinary collaboration (within X‑Fittt 2.0)’, because this cluster covers the collaboration within X‑Fittt 2.0 and should be distinguished from collaboration with stakeholders outside X‑Fittt 2.0.
Adaptations to the effective elements
For almost all clusters, elements were moved to another cluster. For instance, the respondents moved several elements to the cluster ‘preconditions for X‑Fittt 2.0’, such as element 54: ‘Separate room for intakes’. On the other hand, they relocated most of the elements from the original cluster ‘preconditions for X‑Fittt 2.0’ to other clusters. For instance, element 24: ‘Easy to read and complete information leaflet’ was moved to the cluster ‘monitoring’.
The respondents reformulated some elements to make them more specific. For instance, element 12: ‘Structure in the first 12 weeks’ was reformulated to ‘Structure in the first 12 weeks (sports sessions and appointments with professionals)’, and element 21: ‘Low costs’ into ‘Low costs for participants’. Element 59: ‘Safe environment’ could, according to the respondents, be interpreted in two ways:
-
1.
a physically safe environment with appropriate expertise to save someone’s life in case of an emergency, or
-
2.
a socially safe environment where people feel at ease and do not feel ashamed of their body.
As respondents felt that the latter applied to this element, they reformulated element 59 to ‘Socially safe environment’.
Some elements were not really suitable for the target population of citizens with a low SES, so the respondents removed them from the final list of effective elements. For instance, element 25: ‘An information meeting (optional)’ was removed, as the target population is not interested in an information meeting, according to the respondents.
Some elements were merged. For instance, element 28: ‘First intake with lifestyle coach, then intakes with physiotherapist and dietitian’ and element 35: ‘Intake (acquaintance)’ were merged and then reformulated into element 92: ‘First meeting/intake with lifestyle coach, then intakes with physiotherapist and dietitian, to make sure all questions have been answered’.
The respondents added one effective element to the final list, namely element 97: ‘Fixed coordinator/contact person within X‑Fittt 2.0’, as they considered it to be important that someone should coordinate and take the lead within the intervention. This person is the main contact person for all public health practitioners involved in X‑Fittt 2.0. No importance score is available for this element, as it was not part of step 4 of the CM process.
Overview of clusters and active elements
Due to the adjustments of the respondents to the clusters and elements (Appendix, Table 2), the group meeting resulted in slightly different clusters, containing 72 effective elements (Table 1). The cluster labels were reformulated into definitive labels that contain guidelines that can be used in practice (Table 1). For instance, the cluster ‘preconditions for X‑Fittt 2.0’ was reformulated into ‘make sure the preconditions for X‑Fittt 2.0 are established’.
Discussion
In this case study, we used CM to unravel the effective elements of the Dutch CLI X‑Fittt 2.0. This resulted in 72 effective elements clustered into nine meaningful clusters, which are presented as guidelines that can be useful for practice. Our clusters of effective elements show similarities with previous research findings [15, 19,20,21], but differ from earlier findings by focusing on CLIs for citizens with a low SES, being more comprehensive and usable in practice, and by indicating the importance of the different elements.
Our study has been the first to indicate the effective elements of a CLI for citizens with a low SES. In one other study, a Delphi study, Nagelhout et al. (2018) investigated the preconditions of more general lifestyle interventions for people with a low SES [20]. These preconditions are similar to some of the effective elements found in our study, such as the costs and location of the intervention, as well as elements concerning guiding participants within the intervention.
Furthermore, our overview of effective elements is more comprehensive than previous overviews. For instance, the Knowledge Centre for Sport Netherlands identified 12 effective elements of CLIs for the general population [19], compared to the 72 effective elements in our research. Another study, by Morgan et al. (2016), listed inactive adults’ barriers to and facilitators for adhering to exercise referral schemes [21]. These are more or less similar to our effective elements focusing on tackling barriers to and stimulating facilitators for being physically active, especially in our clusters ‘offer structure and sufficient guidance throughout X‑Fittt 2.0’, ‘offer a pleasant and accessible sports environment’, and ‘offer a suitable physical activity programme in the first 12 weeks’. Additionally, our list also includes clusters of elements concerning the organisation of X‑Fittt 2.0, such as clusters on recruitment, preconditions, and collaborations. Our overview is also more extensive and detailed than the checklist of good practice characteristics of diet and PA interventions as proposed by Horodyska et al. (2015) [15]. For instance, one of the characteristics of Horodyska and colleagues is ‘ongoing support from stakeholders secured’, compared to our more precise element 86: ‘long-term guidance by lifestyle coach (2 year)’. Another result that our research adds to existing literature is our cluster ‘make well-defined agreements for participation in X‑Fittt 2.0’. X‑Fittt 2.0 public health practitioners stressed that a contract between participants and public health practitioners is important to ensure that everyone knows what to expect from each other and to know what the consequences are for non-compliant and early drop-out participants. They experienced that many participants are not compliant to X‑Fittt 2.0 and drop out of the programme early, a problem other researchers studying lifestyle interventions for citizens with a low SES also encountered [29, 30].
A final difference as compared to previous studies is the scoring of individual elements on importance (from 1: least important, to 5: most important), which determined the final clusters’ importance scores. The importance scores varied somewhat between clusters, ranging between 4.04 for the cluster ‘make sure the preconditions for X‑Fittt 2.0 have been established’ and 4.44 for the cluster ‘offer proper monitoring’. During the group meeting, however, the respondents indicated that the lowest scoring cluster ‘make sure the preconditions for X‑Fittt 2.0 have been established’ was most important, as the preconditions are essential to start a CLI. As in previous research [31, 32], the scores thus helped to gain insight into nuances concerning the results, since it facilitated the discussion on importance of the different clusters.
Strengths & limitations
Our study identified effective elements of a CLI for citizens with a low SES, using the CM method. Due to the individual participation of respondents during steps 2, 3 and 4 in the CM process, the final product reflects the individual input of all respondents. This has the advantage that the contribution of all respondents was equal. Although CM was useful for our research aim, a few methodological issues regarding the bridging scores emerged, related to the group meeting and the use of the CM results.
After analysis, the bridging scores give an indication of the degree of heterogeneity within a cluster. Five of the nine clusters, including the three most important ones (“offer proper monitoring”, “develop internal multidisciplinary collaboration (within X‑Fittt 2.0)” and “develop external intersectoral collaboration (within the municipality)”), had a fairly high score (> 0.5) prior to the group meeting, indicating higher heterogeneity. However, these scores were not used in this study to determine the number of clusters in the cluster map. We found that applying the bridging scores did not add value to our approach to the CM method, in which we discussed and adapted the cluster map with clusters and elements during the group meeting. During the group meeting, the respondents reflected on the analysis’ cluster solution to ensure that the overview of effective elements of X‑Fittt 2.0 represents the ideas of the respondents. We used the results from the analysis (multidimensional scaling and hierarchical cluster analysis) as input for the group meeting to start the discussion. Our respondents merged and reformulated clusters, formed a new cluster, and moved, reformulated, removed, merged, and added effective elements when they felt that would improve the overview of the effective elements of X‑Fittt 2.0. According to Kane & Trochim (2007), respondents can change or rearrange the cluster map during the group meeting until it makes sense to them [27]. In contrast to our study, other studies show limited changes during this step: deciding on the number of clusters, naming clusters, and/or identifying regions of related clusters [33,34,35,36,37].
In the group meeting, also in-depth insight into the meaning and importance of elements became clear. For instance, element 59: ‘safe environment’ could be interpreted in different ways, which might have influenced the clusters of the individual respondents in step 3. Some respondents interpreted this element as a physically safe environment, while most other respondents, interpreted this element as a socially safe environment. Since formulations of effective elements always run the risk of diverse interpretations, this might need some extra attention while revising the brainstorming list in future research. The group meeting provided the opportunity to make an inventory of these diverse interpretations and to reach consensus, which has been valuable and has created a more precise overview. We recommend including such an extensive group meeting in future research.
As this study is a case study, the results cannot be blindly copied to any CLI for citizens with a low SES. What works for X‑Fittt 2.0 in Arnhem might not automatically work in other municipalities, as the context is different [14, 18]. Furthermore, the number of respondents was small (n = 10, group meeting: n = 4) and, besides the nine public health practitioners, only one X‑Fittt 2.0 participant participated. Except for the dietitians, every discipline within X‑Fittt 2.0 (coordinators, sports coaches, physiotherapists and lifestyle coaches) was represented during the CM process and in the group meeting. However, because only one participant of X‑Fittt 2.0 partially participated in the research, the question is whether the results sufficiently reflect the citizens with a low SES. The X‑Fittt 2.0 participant had an ‘perspective from experience’ and emphasised what helped him/her during X‑Fittt 2.0. The public health practitioners had more of an ‘organisational’ perspective and emphasised mainly practical matters. In follow-up research it is therefore recommended to involve more participants with a low SES.
To obtain more results that can be generalised, the recommendation is to repeat the research with a larger group of respondents involved in different CLIs for citizens with a low SES, thereby broadening the focus of the research. This could be useful to obtain a broad and more general view on the effective elements of CLIs for citizens with a low SES. This in turn can also be used for other CLIs, such as BeweegKuur and SLIMMER, as these are not specifically developed for citizens with a low SES [10].
Conclusions
The main goal of this study was to gain insight into the effective elements of CLIs for people with a low SES. We did this using the CLI X‑Fittt 2.0 as a case study and using the CM method. This resulted in an overview of 72 effective elements of X‑Fittt 2.0, which were clustered into nine meaningful clusters:
-
1.
‘offer proper monitoring’;
-
2.
‘develop internal multidisciplinary collaboration (within X‑Fittt 2.0)’;
-
3.
‘develop external intersectoral collaboration (within the municipality)’;
-
4.
‘offer structure and sufficient guidance throughout X‑Fittt 2.0’;
-
5.
‘make well-defined agreements for participation in X‑Fittt 2.0’;
-
6.
‘offer a suitable physical activity programme in the first 12 weeks’;
-
7.
‘offer a pleasant and accessible sports environment’;
-
8.
‘use sufficient and proper recruitment strategies’;
-
9.
‘make sure the preconditions for X‑Fittt 2.0 have been established’.
According to our respondents, the preconditions of a CLI, such as a proper location with proper equipment, are most important to start the programme. For the continuity of healthy behaviours, long term guidance by a lifestyle coach and useful tools to prevent relapse are most important. Using CM to unravel the effective elements of X‑Fittt 2.0 was useful and structured. It is recommended to use this method in future research focusing on a group of respondents that has a broader view of CLIs. The overview of active elements presented in this study provides a first exploration of the active elements of a CLI for citizens with low SES. This provides a valuable basis for follow-up research into the effective elements of CLIs for citizens with low SES.
References
RIVM. Volksgezondheid Toekomst Verkenning 2018: Trendscenario Gezondheidsverschillen. Utrecht: RIVM; 2018. https://www.vtv2018.nl/gezondheidsverschillen. Last access: 9 Oct 2019.
RIVM. Beweegrichtlijnen naar opleiding. Utrecht: RIVM; 2018. https://www.volksgezondheidenzorg.info/onderwerp/bewegen/cijfers-context/huidige-situatie#node-beweegrichtlijnen-naar-opleiding. Last access: 9 Oct 2019.
RIVM. Overgewicht volwassenen. Utrecht: RIVM; 2019. https://www.volksgezondheidenzorg.info/onderwerp/overgewicht/cijfers-context/huidige-situatie#node-overgewicht-volwassenen. Last access: 9 Oct 2019.
Warburton DER, Nicol CW, Bredin SSD. Health benefits of physical activity: the evidence. Can Med Assoc J. 2006;174(6):801–9.
Miller CT, Fraser SF, Levinger I, Straznicky NE, Dixon JB, Reynolds J, et al. The effects of exercise training in addition to energy restriction on functional capacities and body composition in obese adults during weight loss: a systematic review. PLoS ONE. 2013;8(11):e81692.
Loketgezondleven.nl.. Gecombineerde Leefstijlinterventie. Utrecht: RIVM; 2015. https://www.loketgezondleven.nl/leefstijlinterventies/gecombineerde-leefstijlinterventie. Last access: 9 Oct 2019.
Storm I, Aarts MJ, Harting J, Schuit AJ. Opportunities to reduce health inequalities by ‘Health in All Policies’ in the Netherlands: an explorative study on the national level. Health Policy. 2011;103(2–3):130–40.
Lion A, Vuillemin A, Thornton JS, Theisen D, Stranges S, Ward M. Physical activity promotion in primary care: a Utopian quest? Health Promot Int. 2019;34(4):877–86.
Beenackers MA, Nusselder WJ, Oude Groeniger J, van Lenthe FJ. Het terugdringen van gezondheidsachterstanden: een systematisch overzicht van kansrijke en effectieve interventies. Rotterdam: Erasmus MC Universitair Medisch Centrum; 2015.
Mulderij L, Verkooijen K, Wagemakers A. Gecombineerde leefstijlinterventies voor mensen met een lage SES? Tijdschr Gezondheidswet. 2019;97(1):9–10.
Goodwin L, Ostuzzi G, Khan N, Hotopf MH, Moss-Morris R. Can we identify the active ingredients of behaviour change interventions for coronary heart disease patients? A systematic review and meta-analysis. PLoS ONE. 2016;11(4):e153271.
Dombrowski SU, Sniehotta FF, Avenell A, Johnston M. Identifying active ingredients in complex behavioural interventions for obese adults with obesity-related co-morbidities or additional risk factors for co-morbidities: a systematic review. Health Psychol Rev. 2012;6(1):7–32.
Blase K, Fixsen D. Core intervention components: identifying and operationalizing what makes programs work. ASPE Research Brief. US Dep Heal Hum Serv. 2013. pp. 2–21.
Wartna J, Vaandrager LL, Wagemakers A, Koelen M. ‘Er is geen enkel werkzaam principe dat altijd werkt.’ Een eerste verkenning van het begrip werkzame principes. Wageningen: Wageningen University; 2012. http://edepot.wur.nl/212691. Last access: 9 Oct 2019.
Horodyska K, Luszczynska A, van den Berg M, Hendriksen M, Roos G, De Bourdeaudhuij I, et al. Good practice characteristics of diet and physical activity interventions and policies: an umbrella review. BMC Public Health. 2015;15(1):1–16.
Herens M, Wagemakers A, Vaandrager L, Koelen M. Exploring participant appreciation of group-based principles for action in community-based physical activity programs for socially vulnerable groups in the Netherlands. Bmc Public Health. 2015;15(1):1173.
Loketgezondleven.nl.. Werkzame elementen. Utrecht: RIVM; 2019. https://www.loketgezondleven.nl/leefstijlinterventies/werkzame-elementen. Last access: 9 Oct 2019.
Kok MO, Vaandrager L, Bal R, Schuit J. Practitioner opinions on health promotion interventions that work: opening the ‘black box’ of a linear evidence-based approach. Soc Sci Med. 2012;74:715–23.
Preller L, Schaars D. Generieke werkzame elementen van Gecombineerde leefstijlinterventies en duurzame uitvoerbaarheid. Ede: Kenniscentrum Sport; 2016. https://www.kenniscentrumsport.nl/publicatie/?generieke-werkzame-elementen-van-gecombineerde-leefstijlinterventies-en-duurzame-uitvoerbaarheid&kb_id=21788. Last access: 9 Oct 2019.
Nagelhout GE, Verhagen D, Loos V, de Vries H. Belangrijke randvoorwaarden bij de ontwikkeling van leefstijlinterventies voor mensen met een lage sociaaleconomische status: een Delphi-onderzoek. Tijdschr Gezondheidswet. 2018;96(1):37–45.
Morgan F, Battersby A, Weightman AL, Searchfield L, Turley R, Morgan H, et al. Adherence to exercise referral schemes by participants—what do providers and commissioners need to know? A systematic review of barriers and facilitators. BMC Public Health. 2016;16:227.
Bukman AJ, Teuscher D, Feskens EJM, van Baak MA, Meershoek A, Renes RJ. Perceptions on healthy eating, physical activity and lifestyle advice: opportunities for adapting lifestyle interventions to individuals with low socioeconomic status. MC Public Heal. 2014;14(1):1036.
Formupgrade. Eindverslag ZonMw. BeweegKuur voor allochtonen vrouwen in Arnhem. Projectnummer 524003049. Den Haag: ZonMw; 2016.
van Dale D, Lanting L, van Delden J. Werkzame elementen, is dat de toekomst? Tijdschr Gezondheidswet. 2015;93(6):199–201.
Loketgezondleven.nl.. Erkende interventies – volwassenen, lage SES. Utrecht: RIVM; 2018. https://interventies.loketgezondleven.nl/interventieoverzicht1?leeftijd=volwassen&lage_ses=1. Last access: 9 Oct 2019.
Wagemakers A, Mulderij LS, Verkooijen KT, Groenewoud S, Koelen MA. Care-physical activity initiatives in the neighbourhood: study protocol for mixed-methods research on participation, effective elements, impact, and funding methods. BMC Public Health. 2018;18(812):1–14.
Kane M, Trochim WMK. Concept mapping for planning and evaluation. Vol. 50. Thousand Oaks: SAGE; 2007.
Kane M. CS Global MAXTM. Ithaca, New York: Concept Systems Incorporated; 2019. https://conceptsystems.com/home. Last access: 9 Oct 2019.
Teuscher D. A lifestyle intervention study targeting individuals with low socioeconomic status of different ethnic origins: needs of the target group and research demands. Maastricht: Maastricht University; 2017.
Roumen C, Feskens EJM, Corpeleijn E, Mensink M, Saris WH, Blaak EE. Predictors of lifestyle intervention outcome and dropout: the SLIM study. Eur J Clin Nutr. 2011;65(10):1141–7.
Wagemakers A, Koelen MA, Lezwijn J, Vaandrager L. Coordinated action checklist: a tool for partnerships to facilitate and evaluate community health promotion. Glob Health Promot. 2010;17(3):17–28.
Wagemakers A, van Husen G, Barrett JB, Koelen MA. Amsterdam’s STI/HIV programme: an innovative strategy to achieve and enhance the participation of migrant community-based organisations. Health Educ J. 2014;74(4):411–23.
Roeg D, van de Goor I, Garretsen H. Towards quality indicators for assertive outreach programmes for severely impaired substance abusers: concept mapping with Dutch experts. Int J Qual Health Care. 2005;17(3):203–8.
Nabitz U, van den Brink W, Jansen P. Using concept mapping to design an indicator framework for addiction treatment centres. Int J Qual Health Care. 2005;17(3):193–201.
Lebel A, Cantinotti M, Pampalon R, Thériault M, Smith LA, Hamelin AM. Concept mapping of diet and physical activity: uncovering local stakeholders perception in the Quebec City region. Soc Sci Med. 2011;72(3):439–45.
Tubbing L, Harting J, Stronks K. Unravelling the concept of integrated public health policy: concept mapping with Dutch experts from science, policy, and practice. Health Policy. 2015;119(6):749–59.
van Bon-Martens MJH, Achterberg PW, van de Goor IAM, van Oers HA. Towards quality criteria for regional public health reporting: concept mapping with Dutch experts. Eur J Public Health. 2012;22(3):337–42.
Funding
This research was funded by ZonMw (project number 50-53110-98-003).
Author information
Authors and Affiliations
Corresponding author
Additional information
Original article: Mulderij, L.S., Verknoeien, K.T., Koelen, M. A. et al. De werkzame elementen van een gecombineerde leefstijlinterventie voor mensen met een lage sociaaleconomische status. Een concept mappen-caseonderzoek. TSG Tijdschrift Gezondheidswet. 2019;97:139–52. https://doi.org/10.1007/s12508-019-00243-w
Appendix
Appendix
The CS global MAX cluster solution
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mulderij, L.S., Verkooijen, K.T., Koelen, M.A. et al. Effective elements of a combined lifestyle intervention for people with low socioeconomic status. A concept mapping case study. TSG Tijdschr Gezondheidswet 100, 64–75 (2022). https://doi.org/10.1007/s12508-022-00333-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12508-022-00333-2