
Abstract
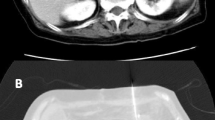
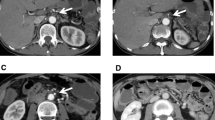
Gastric ischemia is extremely rare and its endoscopic findings appear similar to those of malignant tumors, which makes accurate diagnosis difficult. We present the case of a 41-year-old woman who was admitted to our hospital for severe abdominal pain and vomiting. Laboratory data at the time of admission indicated high serum levels of C-reactive protein, fibrin/fibrinogen degradation products and D-dimer. An abdominal computed tomography (CT) scan revealed a massive dilatation of the stomach and descending portion of the duodenum, which abruptly narrowed at the portion between the superior mesenteric artery and the aorta, indicating massive gastric and duodenal dilatation due to superior mesenteric artery syndrome. Decompression of the upper gastrointestinal tract using a nasogastric tube was started immediately. An esophagogastroduodenoscopy revealed a massive, irregular ulcerative lesion with ill-defined boundaries located in the posterior wall along the greater curvature of the stomach. Although this lesion mimicked a malignant lesion, the biopsy findings revealed a benign gastric ulcer, indicating that the lesion was gastric ischemia caused by the increased intragastric pressure resulting from the massive dilatation. The gastric ischemia healing process was successfully observed through repeated endoscopic examinations of the upper gastrointestinal tract. The patient’s abdominal symptoms disappeared within 10 days and she was discharged from the hospital 23 days after the abdominal episode. This case highlights gastric ischemia associated with an acute massive gastric dilatation resulting in increased intragastric pressure caused by superior mesenteric artery syndrome.






Similar content being viewed by others

References
Uberti G, Goldblum JR, Allende DS. Ischemic enterocolitis and its differential diagnosis. Semin Diagn Pathol. 2014;31:152–64.
Sharma A, Mukewar S, Chari ST, et al. Clinical features and outcomes of gastric ischemia. Dig Dis Sci. 2017;62:3550–6.
Lanciault G, Jacobson ED. The gastrointestinal circulation. Gastroenterology. 1976;71:851–73.
Turan M, Sen M, Canbay E, et al. Gastric necrosis and perforation caused by acute gastric dilatation: report of a case. Surg Today. 2003;33:302–4.
Luncă S, Rikkers A, Stănescu A. Acute massive gastric dilatation: severe ischemia and gastric necrosis without perforation. Rom J Gastroenterol. 2005;14:279–83.
Powell JL, Payne J, Meyer CL, et al. Gastric necrosis associated with acute gastric dilatation and small bowel obstruction. Gynecol Oncol. 2003;90:200–3.
Kerstein MD, Goldberg B, Panter B, et al. Gastric infarction. Gastroenterology. 1974;67:1238–9.
Abdu RA, Garritano D, Culver O. Acute gastric necrosis in anorexia nervosa and bulimia Two case reports. Arch Surg. 1987;122:830–2.
Adson DE, Mitchell JE, Trenkner SW. The superior mesenteric artery syndrome and acute gastric dilatation in eating disorders: a report of two cases and a review of the literature. Int J Eat Disord. 1997;21:103–14.
Tang SJ, Daram SR, Wu R, et al. Pathogenesis, diagnosis, and management of gastric ischemia. Clin Gastroenterol Hepatol. 2014;12:246–52.
Acknowledgements
The authors would like to thank Mrs. Jennifer Holmes for her excellent medical editing of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Yoichi Sakurai, Futoshi Hirai, Michikazu Abe, Tomohisa Okaya, and Hirofumi Suzuki, Isamu Sugano declare that all authors have no conflict of interest.
Human/animal rights
All procedures followed have been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Informed consent
Informed consent was obtained from patient for being included in this case report.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Sakurai, Y., Hirai, F., Abe, M. et al. A case of gastric ischemia caused by massive gastric dilatation due to superior mesenteric artery syndrome. Clin J Gastroenterol 13, 1066–1069 (2020). https://doi.org/10.1007/s12328-020-01192-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12328-020-01192-7