
Abstract
Introduction
Previous societal burden estimations for major depressive disorder (MDD) often fail to account for several hidden cost components. This study provides a comprehensive evaluation of societal costs for adults with MDD in the United States (USA) in 2019. The potential impact of a more effective, rapid-acting MDD therapy vs standard of care on the economic burden of MDD was estimated to illustrate the utility of such a framework in evaluating new interventions.
Methods
This study used a prevalence-based human capital approach. Incremental costs (2019 US dollars) per individual with MDD were derived from national survey inputs and published literature and included incremental healthcare costs and indirect costs. For each cost component, the societal costs were extrapolated by multiplying the per-patient costs by the number of individuals with MDD. The impact of a more effective, rapid-acting novel therapy on the economic burden of MDD was then simulated on the basis of these inputs.
Results
In 2019, the number of adults with MDD in the USA was estimated at 19.8 million (62.7% female; 32.9% severe MDD), and the incremental societal economic burden of MDD was estimated at $333.7 billion ($382.4 billion in 2023 US dollars), or $16,854 per adult with MDD. The primary cost drivers were healthcare costs ($127.3 billion; 38.1%), household-related costs ($80.1 billion; 24.0%), presenteeism ($43.3 billion; 13.0%), and absenteeism ($38.4 billion; 11.5%). In the simulated scenario, a hypothetical novel therapy with a 50.0% early response rate was associated with a 7.7% reduction in the economic burden of MDD relative to standard of care over 12 months.
Conclusions
The economic burden of MDD is substantial and extends beyond healthcare costs, underscoring the impact of MDD across multiple aspects of life. Such a broad societal perspective should be considered in assessing the impact of the advent of effective, rapid-acting MDD therapies.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Why carry out this study? |
The burden of major depressive disorder (MDD) is multifaceted, and a broad societal perspective should be considered in assessing the impact of MDD and external factors such as therapeutic innovations on the economic burden of the disorder. |
This study used up-to-date literature, refined methods, and novel cost components to assess the societal economic burden of adults with MDD in the USA in 2019 and simulated the potential impact of a more effective, rapid-acting MDD therapy on the economic burden of MDD. |
What was learned from the study? |
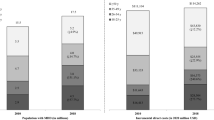
The study demonstrated the sizable incremental economic burden of MDD on adults in the USA in 2019 ($333.7 billion; $382.4 billion in 2023 US dollars). |
A hypothetical rapid-acting novel therapy with an early treatment response rate of 50.0% could reduce the incremental economic burden of MDD by 7.7% relative to the current standard of care. |
There is a need to improve MDD management given its large and increasing impact. |
Introduction
Major depressive disorder (MDD) is an episodic and recurrent condition that affects over 300 million people globally and is a leading cause of disability worldwide [1, 2]. The impact of MDD on an individual’s daily functioning can be severe, which may in turn worsen depressive symptoms, creating a downward spiral in the ability to fulfill family, work, and social responsibilities [2]. In the USA, MDD was shown to account for 2.7 million disability-adjusted life-years in 2016, representing the largest burden among all mental and behavioral health disorders [3]. Managing and treating MDD is often challenging because of its highly comorbid nature with other mental and physical conditions, which can impact patient adherence to treatment [4,5,6,7].
The economic burden of US adults with MDD has increased considerably over time, rising from $236 billion in 2010 to $326 billion in 2018 (2020 US dollars [USD]) [8]. In recent estimates [8], several cost components were incorporated to calculate the economic burden of MDD that were not part of earlier estimates, including healthcare costs, suicide-related costs, and workplace costs (i.e., absenteeism and presenteeism). While healthcare costs are traditionally considered core components in economic appraisals and value discussions for novel therapies, there has been growing recognition of the need to adopt a more holistic view of disease burden as proposed in the ISPOR value flower framework [9, 10]. Consideration of a broader range of cost components may allow for a more comprehensive assessment of costs to evaluate the potential economic implications of a condition on the individual affected as well as on their family/caregivers and society at large. Previous research has demonstrated that the burden of MDD is multifaceted and extends beyond direct costs [8], highlighting the importance of considering components such as productivity loss within as well as outside of the workplace (e.g., due to unemployment or premature mortality) when attempting to contextualize the societal impact of MDD. Furthermore, the spillover effect of the disease burden on families and households is not typically factored into economic and value estimates and is a cost component that has not yet been quantified in MDD to our knowledge [9, 11].
Constructing an impact model of MDD with a broad societal perspective in a systematic way not only helps quantify the disease-level burden but can also serve as a tool to quantify the potential impact of external factors that can increase (such as the COVID-19 pandemic) or decrease (such as therapeutic innovation) the burden. The current study sought to provide an updated estimate of the incremental economic burden of MDD in the USA from a societal perspective by expanding on prior analyses [8] and more comprehensively assessing the burden of MDD using up-to-date literature, refined methods, and incorporating several novel components (i.e., unemployment, all-cause mortality, and household-related costs). To illustrate the utility of such a model, the potential impact of a hypothetical therapy for MDD that is more effective and acts more rapidly than the current standard of care on the incremental economic burden of MDD was also simulated. Variations of this simulation could help contextualize the benefit of therapeutic innovations on the societal burden of MDD and provide unique insights beyond those captured by traditional approaches to value assessments to help inform decision- and policymakers.
Methods
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
The current study evaluated the economic burden of adults with MDD using a prevalence-based and human capital approach. A bottom-up method was used, whereby the average per-patient incremental costs were extrapolated to the national level by multiplying the per-patient costs by the number of individuals with MDD, estimated from the prevalence of MDD and census population data. Mutually exclusive cost components for assessing the economic burden of MDD included healthcare costs, unemployment, absenteeism, presenteeism, disability, mortality, and household-related costs (i.e., economic impact on adults without MDD living with an adult with MDD). Cost estimates for each component were stratified by gender and MDD severity, where available. Details of data sources and calculations are described in the following sections.
Estimation of the MDD Population
The 2019 prevalence of MDD among US adults accounting for persistence and duration of MDD, stratified by gender, was obtained from previously published estimates in the National Survey on Drug Use and Health (NSDUH) [12]. The definition of MDD was proxied from the NSDUH question asking if the respondent experienced a past-year major depressive episode (MDE) according to the criteria in the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) [12]. The prevalence of MDD stratified by MDD severity was obtained from the National Health and Nutrition Examination Survey (NHANES) on the basis of the proportion of respondents with moderate to severe depressive symptoms, which was defined using the Patient Health Questionnaire-9 (PHQ-9) categories of moderate (score 10–14) and severe (score ≥ 15) [13]. Of note, the population of adults with MDD was constructed with the objective of being representative of the general population with MDD, including initial onset MDE and chronic recurrent MDE, and to include adults with MDD regardless of whether they had sought healthcare services and received a formal diagnosis of MDD. However, to increase the specificity of the proxy estimate, the severity proportions were applied to the population of adults with MDD under the assumption that respondents with at least one MDE in the past year (definition in the NSDUH) were represented by individuals with PHQ-9 score of ≥ 10 (definition of moderate and severe MDD in the NHANES).
The total number of adults with MDD was estimated by multiplying the prevalence by the total US adult population in 2019 based on data from the US Census Bureau [14].
Estimation of Economic Burden of MDD
Healthcare Costs
The average annual adjusted incremental all-cause and MDD-related healthcare costs for an adult patient with MDD were obtained on the basis of previous claims-based studies comparing MDD versus non-MDD matched cohorts (matched 1:1 on age, sex, race, and Charlson Comorbidity Index) among commercial, Medicare, and Medicaid beneficiaries [15,16,17].
The weighted average annual incremental healthcare costs per adult with MDD were calculated by weighting the average incremental healthcare costs per health plan type by the population in each respective plan type based on data from the US Census Bureau [18]. For uninsured individuals whose medical costs were covered by federal, state, local institutions, or private sector, the uncompensated healthcare costs were calculated on the basis of a prior literature estimate for the overall US population [19] and adjusted using the ratio of the total annual healthcare costs incurred by the Medicaid-insured MDD versus non-MDD cohorts to account for the higher incremental costs of uninsured adult patients with MDD. The results were stratified by gender and severity of MDD; as a result of the absence of PHQ-9 data in the claims database, the definitions for the severity of MDD were based on the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) code F33.1 for moderate MDD and F33.2 or F33.3 for severe MDD.
The weighted average annual incremental healthcare costs per adult with MDD were then applied to the US adult population with MDD and adjusted for the proportion of patients who seek mental health treatment. The proportions of adults who seek mental health treatment were estimated on the basis of the NSDUH question asking if the respondent who reported a past-year MDE had received any mental health treatment in the past year, stratified by severity of MDD [12].
Unemployment, Absenteeism, Presenteeism, and Disability
Work-related costs associated with MDD included costs of unemployment as well as work productivity loss among those who are employed, comprising absenteeism due to missed days of work and presenteeism due to reduced productivity while at work, and disability.
The incremental costs of unemployment were estimated by multiplying the incremental rate of unemployment or underemployment associated with MDD by the population of adults with MDD and the median annual earnings in the USA, stratified by gender. The rate of employment (including full- and part-time status) was obtained from the 2019 NSDUH data [12]. Data on the median annual earnings by gender were obtained from the US Census Bureau [20].
Among the employed population, the incremental costs of absenteeism and presenteeism were estimated by multiplying the incremental workdays lost associated with MDD by the population of employed adults with MDD and the median annual earnings in the USA, stratified by gender [12, 20]. The number of workdays missed due to absenteeism associated with illness/injury and with not wanting to be at work were based on the 2019 NSDUH data [12]. The number of workdays missed due to presenteeism associated with reduced productivity while at work was based on prior literature estimates [21].
Among the employed population, the incremental costs of disability from work associated with MDD were estimated by multiplying the incremental costs of disability payments for individuals with MDD by the population of employed adults with MDD, stratified by gender. The incremental disability cost associated with MDD for employed individuals was estimated from disability claims in the OptumHealth Reporting and Insights administrative claims database among patients whose employers report disability claims; details of the database were described in Greenberg et al. [8]. The disability cost corresponded to the amount of salary replaced during the disability period for the time elapsed since the date of disability.
Mortality
The incremental costs of productivity loss due to all-cause premature mortality associated with MDD, including suicide, were estimated by applying the number of incremental all-cause mortality among adults with MDD to the average lifetime earnings and adjusted for the employment-to-population ratio per age group with a 5.0% discount rate, stratified by gender. The total number of deaths in the US population was obtained on the basis of data from the US Census Bureau [22]. The incremental number of deaths attributed to MDD was estimated on the basis of findings from a prior literature estimate [23]. The increased odds of suicide associated with MDD was obtained from an analysis of the National Comorbidity Survey [24]. To avoid double counting, suicide-related costs were not included as a separate cost component in the economic burden (i.e., death due to suicide was included in the count of incremental all-cause mortality). The employment-to-population ratio per age group was obtained on the basis of data from the US Census Bureau [25].
Household-Related Costs
The incremental household-related costs associated with MDD were estimated on the basis of the annual income lost among adults without MDD living with an adult with MDD in their households multiplied by the population of adults with MDD estimated to be living with an adult without MDD and the average number of other adults in their households. The inputs related to household-related costs were obtained from prior literature estimates [26, 27].
Simulation of the Economic Burden of MDD with a Novel Therapy
A simulation of a hypothetical scenario in which a rapid-acting novel therapy with an improved efficacy profile were to enter the market was performed, and the potential change in the overall economic burden of MDD in 2019 was assessed. The average rate of early response (defined as ≥ 50.0% improvement in the Hamilton Depression Rating Scale, 17 items [HAMD-17] at the end of week 2 after initiation of treatment) with current standard of care therapies was set to 19.8% based on prior literature [28]. The incremental proportion of adults with MDD who would achieve early response with a novel therapy was estimated on the basis of the proportion of adults with MDD treated with prescription medication for a mood disorder obtained from NSDUH 2019, and the assumed increased rate of early response with the novel therapy (i.e., a hypothetical rate of 50.0% within 2 weeks). The simulation assumed that all treated patients would have used the novel therapy rather than standard of care treatment and that the novel therapy would have the same safety and tolerability profile as the standard of care (i.e., no other changes were simulated beyond an increased rate of response). The simulation was constructed as a thought experiment to illustrate the usefulness of an economic burden of disease model in value assessments of an intervention (e.g., public health programming, novel therapy) in assessing the impact of a potential reduction in the severity and prevalence of MDD on the societal burden of disease.
Statistical Analyses
Cost estimates are presented in 2019 USD and were adjusted using the US Bureau of Labor Statistics Consumer Price Index inflation factor for all cost components; the total incremental costs are additionally presented in 2023 USD. To provide a range of the economic burden around the point estimates, sensitivity analyses were conducted by varying three cost inputs: MDD-related healthcare costs, household-related costs, and presenteeism costs. For lower bound estimates, MDD-related healthcare costs of adults with MDD who did not seek mental health treatment were assumed to be $0; and household-related costs were obtained from published literature that accounted for insurance type in cohort balancing [29]. For upper bound estimates, presenteeism costs were calculated by using a ratio of absenteeism days to presenteeism days, which was the previous method used in Greenberg et al. [8, 21]. Various total incremental economic burden of MDD was estimated by using a combination of base and sensitivity analysis estimates.
For the evaluation of the impact of a rapid-acting novel therapy on the disease burden, a scenario was evaluated by assuming a novel therapy with an early response rate of 50.0% compared to the standard of care rate of early response of 19.8% [28] under the assumption that all treated patients were treated with the novel therapy rather than the standard of care.
Results
Study Sample
The prevalence of MDD among US adults in 2019 was estimated at 7.8%, equivalent to 19.8 million adults with MDD, of which 67.1% had moderate and 32.9% had severe symptoms based on the self-report instrument PHQ-9. An estimated 62.7% (12.4 million) of the MDD population were female; the prevalence rate of MDD was 57.4% higher among women relative to men (9.6% vs 6.1%; Fig. 1).

MDD population in the USA in 2019a. MDD, major depressive disorder; MDE, major depressive episode; NHANES, National Health and Nutrition Examination Survey; NSDUH, National Survey on Drug Use and Health; PHQ-9, Patient Health Questionnaire-9. a The severity of MDD was based on the proportion of patients with moderate to severe depression symptoms, which was defined using the PHQ-9 categories of moderate (score 10–14) and severe (score ≥ 15). Of note, the severity proportions were applied to the population of adults with MDD under the assumption that patients with at least 1 MDE in the past year (definition in the NSDUH) are represented by patients with PHQ-9 score of ≥ 10 (definition of moderate and severe MDD in NHANES). Therefore, it was assumed that no patients with mild depressive symptoms (PHQ-9 score of < 10) would qualify for MDD
Economic Burden of MDD
The total incremental economic burden of adults with MDD in the USA in 2019 was estimated at $333.7 billion (equivalent to $382.4 billion in 2023 USD), or $16,854 per adult with MDD (Table 1); women with MDD accounted for 52.6% of the total burden. The total incremental economic burden of adults with MDD was largely driven by indirect costs ($206.4 billion; 61.9%), including work-related costs of the adult with MDD from presenteeism ($43.3 billion; 13.0%), absenteeism ($38.4 billion; 11.5%), unemployment ($30.3 billion; 9.1%), all-cause mortality ($9.6 billion; 2.9%), and disability ($4.6 billion; 1.4%), and work-related costs of adults without MDD living in a household with an adult with MDD ($80.1 billion; 24.0%; Fig. 2). The latter cost corresponded to 38.8% of all indirect costs associated with MDD (i.e., $80.1 of $206.4 billion) that were borne by adults without MDD living with an adult with MDD in their households. Table 2 summarizes the costs for each component described below; details of the calculations are also presented in the respective supplementary tables.

Percentage breakdown of cost components ($US, billion)
On the basis of sensitivity analyses, the total economic burden of MDD in 2019 was estimated to range from $254.4 billion to $418.6 billion (see Table 3 for details of inputs used for the sensitivity analyses). The sensitivity analysis with the largest impact on the estimated total incremental economic burden of MDD was the upper bound sensitivity for the presenteeism component, which increased the estimated burden by 25.4% with all other sensitivities held constant.
Healthcare Costs
The adjusted incremental healthcare costs per adult with MDD covered by different health plan types or those uninsured, stratified by gender and MDD severity, are presented in Supplementary Table S1.
Extrapolating the weighted average annual incremental per-adult with MDD healthcare costs to the overall US population with MDD, the annual incremental healthcare costs of MDD in the population were estimated at $127.3 billion ($6429 per adult with MDD; Supplementary Table S2).
Unemployment
An estimated 65,302 incremental adults with MDD were unemployed and 623,306 incremental adults with MDD were part-time employed in 2019. The incremental costs of unemployment associated with MDD were estimated at $30.3 billion ($1530 per adult with MDD; Supplementary Table S3), which was driven by unemployment among men with MDD ($31.5 billion) while the incremental costs of unemployment among women with MDD was negative (– $1.2 billion).
Work Productivity Loss
An estimated 1 in 13 adults in the workforce (i.e., 12.1 million) had MDD. Female and male employees with MDD missed an excess of 13.6 and 9.2 workdays per year, respectively, due to illness/injury and 7.5 and 10.0 workdays per year, respectively, due to not wanting to be at work, translating to an annual incremental cost of $38.4 billion ($1940 per adult with MDD) associated with absenteeism among adults with MDD (Supplementary Table S4). Female and male employees with MDD also lost an estimated excess of 23 workdays per year due to reduced productivity while at work, translating to an annual incremental cost of $43.3 billion ($2188 per adult with MDD) associated with presenteeism among adults with MDD (Supplementary Table S5). The incremental costs of disability for employed individuals with MDD were estimated at $4.6 billion ($233 per adult with MDD; Supplementary Table S6).
Mortality
In 2019, there were an estimated 30,899 incremental deaths among adults with MDD in the USA, of which 15,272 were estimated to be due to suicide, accounting for one-third of all suicides that year. The incremental costs of all-cause mortality associated with MDD was estimated at $9.6 billion ($485 per adult with MDD), with suicide-related incremental costs estimated at $7.9 billion ($401 per adult with MDD; Supplementary Table S7).
Household-Related Costs
An estimated 17 million adults without MDD live in a household with an adult with MDD and the total incremental loss in annual income among these individuals was estimated at $80.1 billion ($4048 per adult with MDD; Supplementary Table S8).
Simulation of the Economic Burden of MDD with a Novel Therapy
On the basis of the simulation scenario with a rapid-acting novel therapy evaluating a change in the rate of early response from 19.8% with the current standard of care to a hypothetical rate of 50.0% with a novel therapy that would be used by all treated patients with MDD, the resulting incremental economic burden of MDD in 2019 was $308.0 billion, corresponding to a reduction of 7.7% in incremental economic burden relative to the standard of care.
Discussion
The current study provides a comprehensive and updated assessment of the societal economic burden of adults with MDD as of 2019, with a simulation demonstrating the potential impact of a more effective, rapid-acting novel therapy for MDD. The total incremental costs associated with MDD in 2019 amounted to $333.7 billion (equivalent to $382.4 billion in 2023 USD), or $16,854 per adult with MDD, which was driven by indirect costs (61.9%), including work-related costs of adults with MDD (37.8%; presenteeism, 13.0%; absenteeism, 11.5%; unemployment, 9.1%; all-cause mortality, 2.9%; disability, 1.4%) and work-related costs of adults without MDD living in a household with an adult with MDD (24.0%). As a result of the heterogeneity in the data sources used to obtain the estimate of the economic burden of MDD, it is possible that some cost components were underestimated or overestimated. Therefore, the sensitivity analyses provide an important range of the economic burden of MDD during 2019 of $254.4 to $418.6 billion.
Almost two-thirds of the economic burden of MDD being attributed to indirect costs is consistent with previously published findings [8] and highlights the importance of government agencies and employer groups in adopting strategies for managing MDD.
The current estimate of total incremental costs of MDD in 2019 represents a 3.5% increase in the burden compared with a prior estimate in 2018 (when standardized to 2019 values), with 36.0% of the total incremental costs of MDD in 2019 coming from novel components not previously included in the prior estimate (i.e., unemployment, all-cause mortality, household-related costs) [8]. These costs likely increased in the subsequent time period as a result of the COVID-19 pandemic, which had a substantial impact on the daily functioning and mental health of societies worldwide, including the USA [30, 31]. The global recession resulting from the COVID-19 pandemic also led to job loss among millions of people, producing a substantial economic impact on the USA that is expected to have long-term effects [32].
When comparing the components included in the 2018 and present study, the updated estimates show a 12.8% increase in healthcare costs and a 56.5% reduction in productivity loss (i.e., absenteeism, presenteeism, and disability) compared to the prior year estimates. Compared to previous methods, the current study used the NSDUH data for assessing absenteeism days and US median daily wages to convert workdays lost into costs, which was a more conservative approach than in the prior work which used a commercial database for both workdays missed and associated lost wages given that commercially insured individuals generally have higher income than the general population. In addition, the previous work used a ratio approach of absenteeism to presenteeism workdays lost, which may have overestimated presenteeism-related costs, as shown by the relatively high importance of the sensitivity analysis on the presenteeism-related costs. Therefore, the current study used the ratio of absenteeism to presenteeism in an upper bound sensitivity analysis and a more conservative approach of reported presenteeism days from the literature as the base case analysis. With the use of updated input estimates and improvements in methodology, the overall incremental economic burden of MDD estimated in the current study remained higher as a result of the increasing MDD prevalence, the inclusion of several additional cost components (i.e., unemployment, all-cause mortality, and household-related costs), as well as the use of more recent sources for some cost component estimates.
Indeed, one of the key differentiators of the current study from previous estimations of the economic burden of MDD [8, 33, 34] was the consideration of household-related costs. The spillover costs of MDD to adults living with individuals with MDD may be due to a variety of reasons, including the fact that household members (e.g., adult children or spouse) tend to be primary caregivers for those with mental health conditions [35, 36]. The reduced annual income of adults living in a household with an individual with MDD that was used in this study is in line with the literature that caregivers tend to have reduced employment and work productivity because of their caregiving roles [35, 37,38,39]. As the burden of MDD typically goes beyond the direct impact on the individual with MDD [11], the current study adds to the literature by including the household-related cost component that is often overlooked in societal economic appraisals. Adopting a more holistic view in the assessment of burden of disease is especially important for recognizing the far-reaching impact of a condition on the individuals as well as their family members and caregivers.
In the current estimates of the economic burden of MDD in 2019, incremental costs of unemployment for women were negative. It is important to note that association does not imply causation, and there may be multiple factors that influence the employment rates of women with and without MDD. For instance, previous studies have suggested that individuals with MDD are less likely to get married and on average have fewer children [40, 41]; the reduced responsibilities for childcare, which still largely lie with women, may partially explain the slightly lower unemployment costs for women with MDD compared to women without MDD. Furthermore, it may also be possible that the employment rate among women with MDD is influenced by other demographic or socioeconomic factors such as education status if women with MDD are more likely to have higher education levels or be employed in professions that are less affected by economic downturns, which could contribute to higher employment rates.
The incremental costs of all-cause mortality associated with MDD were estimated at $9.6 billion ($485 per adult with MDD). A third of the total count of suicides in the USA in 2019 (30,899 out of 45,861 suicides) were attributed to MDD, which accounted for 50% of the excess all-cause deaths among adults with MDD in 2019. Despite the large humanistic burden of premature mortality, the resulting economic burden accounted for a relatively low proportion of the total economic burden of MDD (2.9%) given that the opportunity costs of premature mortality were estimated to be attributable to a relatively small proportion of the MDD population (0.2%). On the basis of the current estimates, the economic burden of MDD appears to be substantial and above that of some other mental health conditions (e.g., anxiety [$89 billion], attention-deficit/hyperactivity disorder [ADHD; $123 billion], posttraumatic stress disorder [PTSD; $232 billion], bipolar disorder [$130 billion], schizophrenia [$187 billion]; all 2018 USD), as well as chronic physical health conditions (e.g., coronary heart disease [$199 billion]; 2018 USD) that have also been associated with a sizeable societal burden [42]. Given that MDD is highly comorbid with other mental and physical health conditions [7, 43], which may exert reciprocal impacts on disease severity and management, the burden of MDD is likely partially embodied in the economic assessments of other mental and physical health conditions. In essence, MDD is a costly condition, and its impacts may complicate the burden assessments of other conditions that are commonly comorbid with MDD.
The hypothetical simulation scenario associated with a rapid-acting novel therapy presented in this study demonstrates the potential for advancements in the treatment landscape of MDD to play a crucial role in alleviating the economic burden of MDD. On the basis of the study assumptions, such a novel therapy could reduce 7.7% of the incremental economic burden of MDD relative to the current standard of care, corresponding to approximately $1300 of cost savings per adult with MDD per year, or $2500 per treated adult with MDD. While the exact amount of cost savings would depend on market access, treatment utilization, and the efficacy and safety profile of such a therapy if it were to become available, it is worth noting that the availability of a more effective, rapid-acting therapy for MDD may increase the overall number of patients seeking treatment; thus, the current simulation scenario is potentially an underestimate of the impact of such a novel therapy by assuming that the number of treated patients stays constant. Meanwhile, although the simulation was hypothetical, by improving treatment of MDD, providing improved options, and increasing access to mental health care services, we may be able to reduce the number of people affected by MDD and improve the quality of life, functioning, and productivity for those who suffer from it. This would not only benefit individuals with MDD and their families but would also have the potential to reduce the societal and economic burden of the disorder. Although a rapid-acting novel therapy was simulated in this study, the same methodologies could be applied to assess the potential impact of any public health intervention (e.g., improved mental health professional training, workplace accommodation and health promotion programs, health insurance expansion, and increased mental health research funding [44, 45]). Given work-related components were estimated to contribute to a large proportion of the incremental economic burden of MDD in this study, there should be increased public awareness around labor laws (e.g., the Americans with Disabilities Act and the Family and Medical Leave Act) that aim to improve employment opportunities and protect the rights of individuals with mental or physical impairment. Employer groups may also consider interventions that may help to reduce the strain on employees with MDD, which may ultimately improve work-related metrics and alleviate the associated economic burden.
Finally, it is worth noting that the estimated prevalence of MDD among US adults in 2019 was 7.8%, which was an increase from the previous estimate of 7.1% in 2018 [8]. Results from a recent web survey in 2023 have also suggested that the lifetime prevalence of US adults diagnosed with MDD has increased by 10 percentage points since 2015 [46]. As it was not possible in the current study to identify the factors associated with the rising prevalence of MDD over time, further studies are warranted to monitor trends of MDD and its associated economic burden, especially in light of the COVID-19 pandemic. The pandemic has brought fundamental changes to the lifestyle, work routine, and social relationships of the US population, and there could be long-lasting effects even after the pandemic subsides [47]. Future studies should assess the potential persistence in mental health impacts and associated economic consequences of the pandemic, particularly among vulnerable populations like those with MDD and their families.
Limitations
The current study should be interpreted in light of several limitations. The incremental economic burden of MDD was estimated on the basis of the differential between inputs for adults with MDD and adults without MDD, and therefore should be interpreted as associations rather than causation without an attempt at establishing directionality in terms of the natural history of MDD and associated outcomes. Although the healthcare cost analyses were adjusted for demographic and comorbidity differences between adults with MDD and adults without MDD, the remaining inputs rely on the unadjusted differential between adults with MDD and adults without MDD stratified by gender. Owing to the absence of a single data source for calculating all cost components associated with MDD, the study methodology relies on multiple literature-based estimates; hence, the quality and accuracy of the cost estimates is limited by the available data, which may have resulted in the underestimation or overestimation of certain cost components. The prevalence of MDD was based on findings from the NSDUH, which was designed to generate a national probability sample of the US general population. However, using MDE data from NSDUH as a proxy for MDD and the possibility of self-report bias such as underreporting of depressive symptoms [48] may have affected the true prevalence estimates. In addition, individuals with mild depressive symptoms (PHQ-9 score < 10) were assumed to not qualify for MDD in this study, but there may be mild cases of clinically diagnosed MDD within this spectrum, in which case the associated economic burden would not be captured. Finally, the rapid-acting novel therapy scenario was an exercise based on a hypothetical rate of early response within 2 weeks after initiation of treatment and only considered the immediate impact of increased rate of response/remission without adjustment for long-term societal reductions in the burden of MDD from a life-course perspective (e.g., lower rates of MDD leading to higher rates of education and subsequent employment over time). The assumption that all patients currently receiving a standard of care treatment would transition to a novel therapy is a modelling simplification and does not reflect the reality of treatment market access or the complexity of the management of MDD care and therefore likely represents an idealistic scenario. The novel therapy scenario was intended to illustrate the potential benefit of such therapy on the economic burden of MDD to highlight the importance of management of MDD and the capacity to reduce the societal burden of disease but should not be extrapolated beyond that objective.
Conclusions
MDD exerts a substantial societal economic burden in the USA, underscoring its impact across multiple aspects of life. The economic burden of MDD comprises considerable incremental indirect costs due to loss of workforce and reduced productivity through absenteeism and presenteeism, and almost 40% of the incremental indirect costs of MDD were borne by household members of adults with MDD. The findings of this study provide insight into how the impact of external factors on the economic burden, such as the use of more effective and rapid-acting novel therapies, can be simulated to help inform healthcare decision-making or health-related policy. Given the large and increasing impact of MDD, these results emphasize the need to implement strategies to reduce key cost drivers and improve MDD management to help alleviate its broad economic burden.
References
World Health Organization (WHO). Depression and other common mental disorders: global health estimates. 2017. Report number: WHO/MSD/MER/2017.2. Available from: https://apps.who.int/iris/bitstream/handle/10665/254610/WHO-MSD-MER-2017.2-eng.pdf.
World Health Organization (WHO). Depression fact sheet 2021 [updated September 13, 2021]. https://www.who.int/news-room/fact-sheets/detail/depression. Accessed 2023 Mar 4.
Mokdad AH, Ballestros K, US Burden of Disease Collaborators, et al. The state of US health, 1990–2016: burden of diseases, injuries, and risk factors among US states. JAMA. 2018;319(14):1444–72.
Colman I, Ataullahjan A. Life course perspectives on the epidemiology of depression. Can J Psychiatry. 2010;55(10):622–32.
Ford DE. Optimizing outcomes for patients with depression and chronic medical illnesses. Am J Med. 2008;121(11 Suppl 2):S38-44.
Grenard JL, Munjas BA, Adams JL, et al. Depression and medication adherence in the treatment of chronic diseases in the United States: a meta-analysis. J Gen Intern Med. 2011;26(10):1175–82.
Hasin DS, Sarvet AL, Meyers JL, et al. Epidemiology of adult DSM-5 major depressive disorder and its specifiers in the United States. JAMA Psychiat. 2018;75(4):336–46.
Greenberg PE, Fournier AA, Sisitsky T, et al. The economic burden of adults with major depressive disorder in the United States (2010 and 2018). Pharmacoeconomics. 2021;39(6):653–65.
Lakdawalla DN, Doshi JA, Garrison LP Jr, et al. Defining elements of value in health care—a health economics approach: an ISPOR Special Task Force report [3]. Value Health. 2018;21(2):131–9.
Garrison LP Jr, Neumann PJ, Willke RJ. Reflections on the ISPOR Special Task Force on U.S. value frameworks: Implications of a health economics approach for managed care pharmacy. J Manag Care Spec Pharm. 2019;25(11):1185–92.
National Collaborating Centres for Infectious Disease (NCCID). More than just numbers: exploring the concept of “burden of disease”. 2016. Available from: https://nccid.ca/wp-content/uploads/sites/2/2016/07/ExploringBoD_E.pdf.
Substance Abuse and Mental Health Services Administration (SAMHSA). National Survey on Drug Use and Health (NSDUH), 2019, Crosstab Creator from SAMHSA's public online data analysis system (PDAS) Rockville, MD: Center for Behavioral Health Statistics and Quality; 2019. https://pdas.samhsa.gov/#/survey/NSDUH-2019-DS0001/crosstab/?results_received=false&run_chisq=false&weight=ANALWTQ1Q4_C. Accessed 2022 Jan 18.
National Center for Health Statistics Division of Health and Nutrition Examination Surveys. National Health and Nutrition Examination Survey (NHANES), 2017–2018: Centers for Disease Control and Prevention; 2018. https://wwwn.cdc.gov/nchs/nhanes/continuousnhanes/overview.aspx?BeginYear=2017. Accessed 2022 Jan 18.
United States Census Bureau. Monthly postcensal civilian noninstitutionalized population, July 2019 and July 2020. https://www.census.gov/programs-surveys/popest/technical-documentation/research/evaluation-estimates/2020-evaluation-estimates/2010s-national-detail.html. Accessed 2022 Jan 18.
Namjoshi M, Huang MY, Suthoff E, et al. Epidemiology and economic burden associated with major depressive disorder in a United States Medicaid Population. In: AMCP Nexus; October 11–14, 2022; National Harbor, MD.
Suthoff E, Huang MY, Namjoshi M, et al. Epidemiology and economic burden associated with major depressive disorder in a United States medicare population. In: AMCP Nexus; October 11–14, 2022; National Harbor, MD.
Zhu L, Ferries E, Suthoff E, et al. Economic burden and antidepressant treatment patterns among patients with major depressive disorder in the United States. J Manag Care Spec Pharm. 2022;28(11-a Suppl):S2–13.
United States Census Bureau. 2019 American Community Survey 2020. https://www.census.gov/data/tables/time-series/demo/health-insurance/acs-hi.html. Accessed 2022 Apr 22.
Agency for Healthcare Research and Quality. Mean expenditure per person with expense by insurance coverage, United States, 2017. https://meps.ahrq.gov/mepstrends/hc_use/. Accessed 2020 May 13.
United States Census Bureau. Work experience-people 15 years old and over, by total money earnings, age, race, Hispanic origin, sex, and disability status. https://www.census.gov/data/tables/time-series/demo/income-poverty/cps-pinc/pinc-05.html#par_textimage_0. Accessed 2022 Jan 18.
Stewart WF, Ricci JA, Chee E, et al. Cost of lost productive work time among US workers with depression. JAMA. 2003;289(23):3135–44.
Xu J, Murphy SL, Kochanek KD, et al. National Vital Statistics Reports - deaths: final data for 2019. US Department of Health & Human Services, Centers for Disease Control and Prevention.
Wicke FS, Ernst M, Otten D, et al. The association of depression and all-cause mortality: explanatory factors and the influence of gender. J Affect Disord. 2022;15(303):315–22.
Kessler RC, Borges G, Walters EE. Prevalence of and risk factors for lifetime suicide attempts in the National Comorbidity Survey. Arch Gen Psychiatry. 1999;56(7):617–26.
United States Census Bureau. Employment status 18 years and over by veteran status, age, and period of service, 2018 annual averages. https://www.bls.gov/cps/cps_htgm.htm. Accessed 2022 Jan 18.
Chitnis A, O’Callaghan L, Fournier AA, et al. Impact of living with an adult with major depressive disorder among households in the United States. In: AMCP 2023; March 21–24, 2023; San Antonio, TX.
Chitnis A, O’Callaghan L, Fournier AA, et al. Sociodemographic indicators and quality of life impact of major depressive disorder in the United States using the Medical Expenditure Panel Survey. In: ISPOR 2023; May 7–10, 2023; Boston, MA.
Voller C, Hickey C, Tan R, et al. Assessing the onset of efficacy and tolerability of pharmacological treatments in major depressive disorder: a systematic literature review and descriptive analysis. [unpublished manuscript]. 2023.
Chitnis A, O’Callaghan L, Fournier AA, et al. Impact of living with an adult with major depressive disorder among households in the United States. J Affect Disord. 2023. (in press).
Bhattacharjee B, Acharya T. The COVID-19 pandemic and its effect on mental health in USA—a review with some coping strategies. Psychiatr Q. 2020;91(4):1135–45.
Pfefferbaum B, North CS. Mental health and the Covid-19 pandemic. N Engl J Med. 2020;383(6):510–2.
Chetty R, Friedman JN, Stepner M, et al. National Bureau of Economic Research Working Paper 27431-the economic impacts of COVID-19: evidence from a new public database built using private sector data [updated April 2023]. https://www.nber.org/papers/w27431. Accessed 11 May 2023.
Chow W, Doane MJ, Sheehan J, et al. Clinical brief. Economic burden among patients with major depressive disorder: an analysis of healthcare resource use, work productivity, and direct and indirect costs by depression severity. Am J Manag Care. 2019. (Supplements and Featured Publications. February 2019). https://www.ajmc.com/view/economic-burden-mdd.
Jain S, Gupta S, Li VW, et al. Humanistic and economic burden associated with depression in the United States: a cross-sectional survey analysis. BMC Psychiatry. 2022;22(1):542.
Reinhard SC, Young HM, Levine C, et al. Home alone revisited: family caregivers providing complex care. American Association of Retired Persons (AARP) Public Policy Institute; 2019.
Riffin C, Van Ness PH, Wolff JL, et al. Multifactorial examination of caregiver burden in a national sample of family and unpaid caregivers. J Am Geriatr Soc. 2019;67(2):277–83.
Lilly MB, Laporte A, Coyte PC. Labor market work and home care’s unpaid caregivers: a systematic review of labor force participation rates, predictors of labor market withdrawal, and hours of work. Milbank Q. 2007;85(4):641–90.
Liu Y, Dokos M, Fauth EB, et al. Financial strain, employment, and role captivity and overload over time among dementia family caregivers. Gerontologist. 2019;59(5):e512–20.
Skalicky AM, Rentz AM, Liu Z, et al. Economic burden, work, and school productivity in individuals with tuberous sclerosis and their families. J Med Econ. 2018;21(10):953–9.
Breslau J, Miller E, Jin R, et al. A multinational study of mental disorders, marriage, and divorce. Acta Psychiatr Scand. 2011;124(6):474–86.
Golovina K, Elovainio M, Hakulinen C. Association between depression and the likelihood of having children: a nationwide register study in Finland. Am J Obstet Gynecol. 2023;228(2):211e1–11.
Davis LL, Schein J, Cloutier M, et al. The economic burden of posttraumatic stress disorder in the United States from a societal perspective. J Clin Psychiatry. 2022;83(3):21m14116. https://doi.org/10.4088/JCP.21m14116
Iosifescu DV, Nierenberg AA, Alpert JE, et al. The impact of medical comorbidity on acute treatment in major depressive disorder. Am J Psychiatry. 2003;160(12):2122–7.
Castillo EG, Chung B, Bromley E, et al. Community, public policy, and recovery from mental illness: emerging research and initiatives. Harv Rev Psychiatry. 2018;26(2):70–81.
Centers for Disease Control and Prevention (CDC). Workplace health strategies - depression: Division of Population Health, National Center for Chronic Disease Prevention and Health Promotion; 2020. https://www.cdc.gov/workplacehealthpromotion/health-strategies/depression/index.html. Accessed 2023 Jul 3.
Witters D. U.S. Depression rates reach new highs: Gallup, Inc.; 2023. https://news.gallup.com/poll/505745/depression-rates-reach-new-highs.aspx. Accessed 11 May 2023.
Ornell F, Schuch JB, Sordi AO, et al. “Pandemic fear” and COVID-19: mental health burden and strategies. Braz J Psychiatry. 2020;42(3):232–5.
Hunt M, Auriemma J, Cashaw AC. Self-report bias and underreporting of depression on the BDI-II. J Pers Assess. 2003;80(1):26–30.
Ettman CK, Abdalla SM, Cohen GH, et al. Prevalence of depression symptoms in US adults before and during the COVID-19 pandemic. JAMA Netw Open. 2020;3(9):e2019686.
Acknowledgements
Author Contribution
Paul Greenberg, Jessica Maitland, Patrick Gagnon-Sanschagrin, and Andree-Anne Fournier contributed to study conception and design, collection and assembly of data, and data analysis and interpretation. Abhishek Chitnis, Derek Louie, Ellison Suthoff, Shih-Yin Chen, and Ronald C Kessler contributed to study conception and design, data analysis and interpretation. All authors reviewed and approved the final content of this manuscript.
Funding
Sponsorship for this study and Rapid Service Fee were funded by Biogen Inc. (Cambridge, MA) and Sage Therapeutics, Inc. (Cambridge, MA). The study sponsor was involved in several aspects of the research, including the study design, interpretation of data, writing of the manuscript, and decision to submit the manuscript for publication.
Medical Writing/Editorial Assistance
The authors would like to thank Lasair O'Callaghan, MPH, an employee of Sage Therapeutics, Inc., for her contribution to the development of this study. Medical writing assistance was provided by professional medical writer, Flora Chik, PhD, MWC, an employee of Analysis Group, Inc., a consulting company that has provided paid consulting services to Biogen Inc. and Sage Therapeutics, Inc., which funded the development and conduct of this study and manuscript. Logistical support was also provided by Boston Strategic Partners, Inc. (funded by Biogen Inc. and Sage Therapeutics, Inc.).
Data Availability
The data supporting the findings of this study are available within the article and its supplementary materials.
Ethical Approval
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Conflict of Interest
Paul Greenberg, Jessica Maitland, Patrick Gagnon-Sanschagrin, and Andree-Anne Fournier are employees of Analysis Group, Inc. Abhishek Chitnis and Shih-Yin Chen are employees of Biogen Inc and may hold stock. Derek Louie and Ellison Suthoff are employees of Sage Therapeutics, Inc., and may hold stock and/or stock options. Ronald C Kessler has been a consultant for Cambridge Health Alliance, Canandaigua VA Medical Center, Holmusk, Partners Healthcare, Inc., RallyPoint Networks, Inc., and Sage Therapeutics, Inc., and has stock options in Cerebral Inc., Mirah, PYM, Roga Sciences and Verisense Health.
Author information
Authors and Affiliations
Corresponding author
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Greenberg, P., Chitnis, A., Louie, D. et al. The Economic Burden of Adults with Major Depressive Disorder in the United States (2019). Adv Ther 40, 4460–4479 (2023). https://doi.org/10.1007/s12325-023-02622-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-023-02622-x