
Abstract
Desmoid tumors (DT) are rare, locally aggressive, fibroblastic soft-tissue tumors that are characterized by infiltrative growth and can affect organs and adjacent structures, resulting in substantial clinical burden impacting patients’ health-related quality of life. Searches of PubMed, Embase, Cochrane, and key conferences were conducted in November 2021 and updated periodically through March 2023 to identify articles describing the burden of DT. Of 651 publications identified, 96 relevant ones were retained. Diagnosis of DT is challenging because of its morphologic heterogeneity and variable clinical presentation. Patients visit multiple healthcare providers, often facing delays in correct diagnosis. The low incidence of DT (estimated 3–5 cases per million person-years) limits disease awareness. Patients with DT experience a high symptom burden: up to 63% of patients experience chronic pain, which leads to sleep disturbance (73% of cases), irritability (46% of cases), and anxiety/depression (15% of cases). Frequently mentioned symptoms are pain, limited function and mobility, fatigue, muscle weakness, and swelling around the tumor. Overall, quality of life in patients with DT is lower than in healthy controls. There is no treatment approved by the US Food and Drug Administration for DT; however, treatment guidelines reference available options, such as active surveillance, surgery, systemic therapy, and locoregional therapy. Choice of active treatment may depend on tumor location, symptoms, and risk of morbidity. The substantial burden of illness of DT is related to difficulties in timely and accurate diagnosis, high symptom burden (pain and functional limitations), and decreased quality of life. There is a high unmet need for treatments that specifically target DT and improve quality of life.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Desmoid tumors (DT), also known as desmoid-type fibromatosis or aggressive fibromatosis, are rare, soft-tissue tumors that can cause debilitating pain, deformity, and even life-threatening organ damage to patients. DT is locally aggressive and exhibits infiltrative growth and a tendency to recur after surgery. |
Patients with DT experience symptoms of pain and impaired mobility that can negatively impact their daily activities and overall quality of life. |
Because of the variable clinical presentation and low incidence (3–5 cases per million person-years) of DT, delayed or inaccurate diagnoses are common. |
Guidelines for DT recommend options such as active surveillance, locoregional treatments, and systemic treatments. |
Unmet needs in DT include early and accurate diagnosis and approved treatments indicated for patients with DT. |
Introduction
Desmoid tumors (DT)—also known as desmoid-type fibromatosis (DTF) or aggressive fibromatosis—are rare, locally aggressive, fibroblastic soft-tissue tumors that are characterized by infiltrative growth and tendency to recur [1,2,3]. Desmoid tumors do not metastasize but can arise in any part of the body: extra-abdominal (appear in the head and neck, chest, extremities), and abdominal wall or intra-abdominal (originating in tissue that connects abdominal organs) [1, 2, 4, 5]. Depending on their location, DT can cause debilitating pain and deformity and even life-threatening organ damage [2, 4, 5].
There are two types of DT: sporadic tumors, which form the majority of all DT (85–90%) and harbor somatic β-catenin (CTNNB1) gene mutations; the remainder of DT (10–15%) occur in patients with mutations in the adenomatous polyposis coli (APC) gene, including patients with familial adenomatous polyposis (FAP), a tumor predisposition syndrome [6, 7].
The exact mechanism of disease is unclear. Two pathways have been implicated in the canonical Wnt/β-catenin/APC pathway, in which CTNNB1 and APC mutations lead to β-catenin accumulation [1, 7, 8], and the Notch pathway, in which two cleavages at Notch receptors occur (one by ADAM10 in the extracellular domain and the other in the intracellular domain by gamma-secretase) [1]. The potential cross-talk between the Notch and Wnt pathways, as well as activation of the Notch pathway resulting from dysregulation of the Wnt pathway, are thought to be involved in the pathogenesis of DT [9,10,11,12,13,14].
The course of DT is unpredictable, as spontaneous regression, stable disease, and disease progression can all occur [2, 6, 15, 16]. Depending on the location and size of the tumor and other factors, the risk of recurrence after surgical treatment can be high [17,18,19,20].
Characterizing the burden of illness for rare diseases such as DT is difficult because of the inherent challenges associated with identification and evaluation of a small patient population. Recent reviews have focused on molecular pathogenesis, diagnosis, and management of DT [1, 8, 21,22,23]. To our knowledge, there is no published, comprehensive review on the burden of illness of DT. Here, we examine the burden of this disease, including its diagnostic challenges, clinical symptom burden, and impact on quality of life (QOL). Additionally, current management approaches and new treatments under investigation for DT are reviewed.
Methods
Data Sources and Search Strategy
Key terms related to the study topics were used to search relevant research articles in the PubMed, Embase, and Cochrane Library databases. The initial searches were conducted to identify only articles including human data and published in English from November 2011 to November 2021. (Details for search strategies in each database are provided in Supplementary Materials Tables S1–S4.) Conference abstracts published from 2015 to 2022 were also reviewed. In addition, the bibliographies of identified literature reviews and key studies were reviewed to identify additional seminal studies published before 2011. The searches were updated periodically through March 2023, using the same search strategy and criteria as those used in the original search, to obtain the most up-to-date literature since the previous search. This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Inclusion Criteria and Selection of Studies
Selection of studies was based on predefined inclusion and exclusion criteria (see Supplementary Materials Table S5) and was completed through two levels of study: at level 1, titles and abstracts of the identified studies were reviewed to evaluate the potential study relevance; at level 2, full texts of studies selected at level 1 were reviewed. The most recent and relevant studies describing the disease and its diagnosis, epidemiology, treatment, and clinical, humanistic, and economic burden were selected for inclusion. Data relevant to the study objectives were extracted by one reviewer and quality checked by a second reviewer.
Results
A total of 541 unique titles and abstracts were identified from the database searches; of these, 362 were excluded during level 1 (abstract/title) screening and 179 progressed to level 2 (full-text) screening. After desktop and conference searches, 65 sources met the inclusion criteria and form the evidence base for this review. The updated searches, conducted in December 2022 and March 2023, resulted in 110 additional titles and abstracts, of which 31 references were found to be relevant.
Epidemiology and Risk Factors
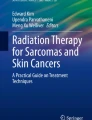
Five European sources [24,25,26,27,28] providing estimates on the incidence of DT were identified in the literature. No study evaluating the prevalence of DT was identified. Likewise, no epidemiological study of DT in the United States (US) was identified. All the primary studies are presented in Fig. 1. The most recently published study, Anneberg et al. [24], estimated 2.2 cases per million person-years in 2011 and 4.3 cases per million person-years in 2017 in Denmark, using the Danish Sarcoma Database and excluding patients aged 18 years and younger. Two population-based registry studies [25, 28] have reported incidence estimates of DT in the Netherlands: van Broekhoven et al. [28] estimated 2.10 and 5.36 cases per million person-years in 1993 and 2013, respectively, after excluding patients with intra-abdominal tumors, and Nieuwenhuis et al. [25] estimated an annual incidence of 3.42 cases per million person-years after reviewing cases from 1999–2009 and excluding patients aged 10 years and younger. In Finland [27], annual incidences of 2.4 and 4.3 cases per million person-years were estimated from pathology data collected between 1953 and 1964 and between 1968 to 1972, respectively. The Orphanet Report Series collects data on rare diseases from a number of different sources, including scientific literature, registries, national and international health institutes and agencies, and other reports from experts. The Orphanet Report Series [26] provides an average annual incidence of 3 cases of DT per million person-years in Europe. The epidemiological studies reveal that most DT cases appear in the age range of 20–44 years, with a female predominance, and female cases 2.2–3.9 times the number of male cases [24, 25, 27, 28]. No estimates of incidence of DT in children are available in the literature; there is a lack of data on DT in children younger than 11 years old.

Incidence of DT in European Countries Reported in Primary Studies. DT desmoid tumor. Sources: 1 Reitamo et al. [27], 2 Nieuwenhuis et al. [25], 3 van Broekhoven et al. [28], 4 Anneberg et al. [24]. Data from the Orphanet report [26] is not included in this figure because the data represent an average of various primary sources
Regarding mortality, there is only one study [24] that has reported a 5-year mortality rate of 7 per 1000 [95% confidence interval (CI) 3–16] among Danish patients with DT as compared with 5 per 1000 (95% CI, 4–7) in a healthy matched cohort. The adjusted hazard ratio of dying was 1.3 (95% CI, 0.6–3.2) for patients with DT compared with the matched cohort. The authors state that most deaths occurred in patients with FAP, though they represented only 7% of patients in the DT cohort.
Several risk factors for the development of DT are cited in the literature:
-
Trauma: Up to 25% of DT cases have been associated with episodes of antecedent trauma; and for abdominal wall and intra-abdominal wall DT, 68–86% of cases are noted after abdominal surgery. Patients with FAP are at even greater risk for DT development following surgical trauma, with a reported 84% of cases of FAP-associated DT occurring within 5 years of abdominal surgery [2].
-
Estrogen and pregnancy: This disease has a high female predominance. Estrogen may influence tumor growth and spontaneous regression. In women of childbearing age, DT have a greater growth rate than those in males or in premenopausal or postmenopausal women; in addition, the frequency rate of DT increases during pregnancy and in women taking oral contraceptives; and cases of DT developed at the site of a prior cesarean section scar has been reported [3]. In particular, abdominal wall DT has been shown to occur more frequently in patients with a recent history of pregnancy, and the risk of progression or relapse of DT is twice as high in female patients with a recent pregnancy versus those without recent pregnancy [29]. Spontaneous regression has been observed during menopause, after tamoxifen treatment, and after oral contraceptive use in some cases [2, 3].
-
APC gene mutations are associated with development of FAP-related DT as well as 10–15% of sporadic DT [3, 7, 16, 30].
Diagnostic Challenges
The diagnosis of DT requires medical history review and physical examination, imaging, and biopsy and histopathology evaluation [31]. A definitive diagnosis of DT can be made via histopathologic analysis of a biopsy sample of the tumor [8, 32] Although immunohistochemical analysis can be used to detect an additional diagnostic marker—the nuclear overexpression of β-catenin—in tumor cells this marker is not specific to DT and is not positive in all cases [6, 7]. Genetic testing may identify the presence of mutated CTNNB1 or APC, which can be specific to DT [7]. The use of a diagnostic imaging method may depend on tumor location: for example, computed tomography is the method of choice for intra-abdominal DT, whereas magnetic resonance imaging is the preferred imaging technique for extra-abdominal tumors. Ultrasound is often used for pregnant women and DT located in the extremities or the abdominal wall [8]. Because of its morphologic heterogeneity and variable characteristics, patients with DT face multiple diagnostic challenges:
-
Delays in diagnosis: patient-related delays can result from the inability to recognize the importance of symptoms, whereas healthcare provider–related delays can result from practice settings in which providers lack specific expertise in DT, potential for incorrect referral, and multiple healthcare provider visits prior to a correct diagnosis [4]. In a study to explore health-related quality-of-life (HRQOL) challenges faced by patients with DT [4], most of the patients interviewed reported delays in diagnosis. They experienced a long diagnostic trajectory within primary and secondary healthcare and were transferred from “hospital to hospital to hospital” to receive the correct diagnosis of DT. Patients were frustrated by lack of continuity and differing opinions offered by clinicians at each hospital appointment.
-
Misdiagnosis: misdiagnosis is common in rare diseases such as DT [4, 6, 33]. Based on pathologic similarities with other myofibroblastic diseases (e.g., sarcoma, gastrointestinal stromal tumor, nodular fasciitis, leiomyoma) and the low incidence of DT, 30–40% of DT cases are reported to be misdiagnosed following histologic analysis [33,34,35]. A French nationwide survey demonstrated that one-third of DT are misdiagnosed (the most challenging differential diagnoses are nodular fasciitis and low-grade fibromyxoid sarcoma) [33]. In a focus group study [4], several patients were initially given a diagnosis of “cancer” or “malignant sarcoma” and were informed that the anticipated prognosis was bleak, which caused emotional distress.
Clinical Burden
The morbidity and mortality associated with DT largely depend on the tumor location, as this determines the adjacent structures that the DT will infiltrate or compress. Depending on their location, DT tend to infiltrate adjacent organs, extend along fascial planes, compress blood vessels and nerves, erode bones, or obstruct organs such as the bowel. Muscle, nerve, and vessel involvement may cause debilitating symptoms, including pain, restricted mobility, or deformity [2]. For example, tumors affecting extremities may restrict joint movements and consequently cause limping or difficulty in moving arms or legs [5].
The clinical course of the disease varies, and data suggest that an initial tumor growth phase is followed by a long period of growth arrest and even regression. According to estimates, approximately 10–28% of DT will resolve spontaneously without treatment (22% for extra-abdominal tumors to 28% for abdominal tumors) [2, 36, 37], 30% will cycle through progression and resolution, 50% will remain stable after diagnosis, and 10% will progress rapidly [2].
Recurrence rates can also be influenced by tumor location. Tumors on extremities are believed to be locally aggressive and have recurrence rates ranging from 24% to 77% [2]. Local recurrence rates of intra-abdominal tumors in patients with FAP are higher than those for extra-abdominal tumors and reported to be 57–86% [2]. Recurrence rates can be exacerbated by trauma, such as trauma from surgery (and there is a high risk of local recurrence after surgery), and range from approximately 25% to 60% at 5 years [15].
Overall, the clinical burden of patients with DT is considerable because of the pain and physical limitations resulting from the chronic infiltrative nature of this disease, in addition to the functional impacts resulting from surgical interventions. Furthermore, because of the low estimated prevalence of DT (due to low incidence rate), approaches to disease management are often hampered by misdiagnosis or delayed diagnosis, reduced public awareness, lack of expertise outside specialist centers, and treatment uncertainty.
Impact of DT Disease Burden on the Patient’s Quality of Life
Patients can experience compromised QOL due to diagnostic challenges and the high clinical burden of DT, including severe pain, impaired physical function and mobility, and high recurrence rates. This can limit their everyday activities and lead to deterioration in physical, social, and emotional functioning (Table 1) [4, 38,39,40]. In addition, patients with DT may receive treatments that are also used for patients with metastatic cancers and therefore may experience treatment toxicities that decrease their overall QOL. Among all symptoms experienced by patients with DT, pain is the most debilitating and has a large impact on the patient’s QOL. In the survey conducted among the active members of the French patient advocacy group (SOS Desmoïde), pain was present in 63% of cases [41]. In a focus group study by Husson et al. [4], dependency on painkillers was a significant concern for several patients, and others found that pain was unresponsive to analgesics. According to data from the French nationwide prospective database ALTITUDES, at diagnosis (and up to 6 months post-diagnosis), occurrence of pain significantly increased with DT in the neck and shoulder [odds ratio (OR), 3.0; 95% CI, 1.2–7.1) but not in DT in the abdominal wall (OR, 0.5; 95% CI, 0.3–0.8) or intra-abdominal wall (OR, 0.4; 95% CI, 0.2–0.8) compared with other sites (P < 0.001). Large DT (> 50 mm) were significantly associated with increased pain (OR, 1.8; 95% CI, 1.2–2.8; P = 0.011). Furthermore, presence of pain at diagnosis was associated with worse prognosis irrespective of first-line treatment (hazard ratio, 2.0; 95% CI, 1.3–2.9; P = 0.006) [42]. The presence of pain was associated with lower performance status (P = 0.024) and functional impairment (P = 0.001). The 3-year event-free survival probability in the absence of baseline pain was 72.2% (95% CI, 65.1–78.1) and in the presence of baseline pain 53.9% (95% CI, 43.3–63.4) [43]. In a phase 3 trial of an investigational agent, nirogacestat (DeFi trial, n = 142), 41% of patients with progressing DT had uncontrolled pain at baseline, defined as average worst pain intensity score of > 4 as measured using the Brief Pain Inventory-Short Form (range 0–10, with higher scores indicating worse pain) [44]. The pain severity and associated burden of disease can lead to anxiety and depression in many patients [4, 43, 45].
The HRQOL burden of patients with DT has been assessed using a number of non–DT-specific instruments such as the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire–Core Module (EORTC QLQ-C30), Generalized Anxiety Disorder scale-7 (GAD-7), Patient Health Questionnaire-9 (PHQ-9), Edmonton Symptom Assessment System-revised (ESAS-r), Distress Assessment and Response Tool (DART), and Child Health Questionnaire (Table 1) [4, 39, 46, 47].
Recently, a DT-specific HRQOL instrument (the Desmoid-type fibromatosis Quality of Life Questionnaire [DTF-QOL]) was developed and has been shown to cover the spectrum of DT-specific HRQOL issues and can be used alongside the EORTC QLQ-C30 [48]. The impact scales of the DTF-QOL instrument cover various DTF-specific HRQOL issues that are not covered by other generic or cancer-generic questionnaires, including unpredictable disease trajectory of DT or the impact of DT on relationships [49]. In a cross-sectional study, both EORTC QLQ-C30 and DTF-QOL were used to assess the impact of sociodemographic and clinical characteristics on DT-specific HRQOL [50]. The study found that female patients, patients with more than 2 comorbidities, or patients who received treatment other than only active surveillance or surgery (such as systemic therapy or a combination of active treatments, such as surgery, systemic therapy, or local therapy) scored significantly worse on the subscales of both the EORTC QLQ-C30 and the DTF-QOL. It may be that patients on systematic or combination therapy had a more aggressive disease course, explaining the association with worse HRQOL scores. In addition, patients ≥ 40 years of age had worse scores on the physical functioning scale (EORTC QLQ-C30) and patients aged between 18 and 39 years scored significantly worse on several of the DTF-QOL impact scales [50]. Using DTF-QOL and a generic instrument may help clinicians provide better and more personalized care to patients with DT. Another DT-specific instrument—the Gounder/Desmoid Tumor Research Foundation (DTRF) Desmoid Symptom/Impact Scale (GODDESS) patient-reported outcome instrument—assesses symptoms (GODDESS Desmoid Tumor Symptom Scale [GODDESS DTSS]; 11 items, such as pain and fatigue) and impacts (GODDESS Desmoid Tumor Impact Scale [GODDESS DTIS]; 17 items, such as difficulty moving and trouble falling asleep), and was developed on the basis of prospective, concept elicitation, and cognitive interviews of patients with localized or multifocal DT (n = 46) [51]. The scale is being used in several clinical trials (NCT03785964, NCT04871282, and NCT04195399) and has now been validated in the phase 3 DeFi trial [52]. In this trial, GODDESS symptom and impact scores were internally consistent at baseline and at cycles 4 and 7 (Cronbach’s α > 0.70). The test–retest reliability after 2 months was also consistent and had an intraclass correlation coefficient > 0.85. GODDESS symptom and impact scores showed moderate to high correlation with other patient-reported outcomes (PRO) tools, including BPI-SF and EORTC QLQ-C30 [52] In the DeFi trial, baseline values for GODDESS DTSS total symptom scores (SD) in the nirogacestat and placebo groups were 3.4 (2.3) and 3.5 (2.6), respectively, and the GODDESS DTIS physical functioning domain scores (SD) were 2.8 (1.1) and 2.7 (1.2) [53].
Additional instruments that have been used to assess patient burden (HRQOL, anxiety, and depression) include the EORTC QLQ-C30, GAD-7, and PHQ-9. Assessment of patient QOL using these instruments has indicated significantly lower global health status and significantly higher symptom burden of fatigue, pain, insomnia, and financial difficulties in patients with DT (vs. healthy controls) (Table 1). Anxiety and depression have been reported in 39.22% and 50% of patients with DT, respectively, and rates of mild, moderate, and severe anxiety and depression are higher in patients with DT compared with healthy controls [45].
Economic Burden
No studies evaluating direct or indirect costs of patients with DT were identified in the literature. However, a recent study by Anneberg et al. [24] has evaluated healthcare resource utilization of patients with DT treated at two sarcoma centers in Denmark from 2009 to 2018. Data were obtained from the Danish Sarcoma Database. A comparison cohort was randomly selected from the general population to match the patient cohort. Healthcare resource utilization of patients with DT was substantially higher than that in the comparison cohort, both 1 and 3 years after the diagnosis. Within 3 years after the index date, patients with DT had, on average, 1 inpatient and 7.1 outpatient visits as well as 7.5 days in the hospital compared with an average of 0.8 inpatient and 0.1 outpatient visits and 0.8 days in the hospital in the comparison cohort. The median duration of hospitalization for DT-related surgery was 5 days (interquartile range, 3–7).
Studies [4, 41] assessing the impact of DT on employment and job productivity have reported that patients experience a negative impact on their employment due to their disease and find it frustrating being unable to work (26% stopped working and 10% worked part- time; see Table 1). In addition, financial difficulty resulting from loss of employment and hospital travel expenses may be a significant concern for some patients [4]. No monetary costs from loss of employment and hospital travel expenses were reported in these studies.
A cost-analysis by Johns et al. [54] of sorafenib treatment versus placebo based on efficacy data from a phase 3 randomized, double-blind, placebo-controlled trial [55] analyzed patients with DT and disease progression as follows: both clinical and radiologic progression and radiologic progression alone. Total cost of sorafenib was estimated for 1- and 2-year treatment durations based on absolute risk reduction (ARR) and number needed to treat (NNT). At 1 year of treatment, sorafenib was associated with a 43.2% ARR of clinical and radiologic progression. This resulted in an NNT of 2.3 patients per year, which translates to a cost of US$259,406 to prevent one clinical and radiologic progression. When only patients with radiologic progression as defined by Response Evaluation Criteria in Solid Tumors (RECIST version 1.1) were evaluated, those treated with sorafenib experienced ARR of 13.9% with NNT of 7.2 patients per year and estimated costs of $812,052 at 1 year.
Guidelines and Current Treatments
Table 2 summarizes common therapies used for the management of DT. There are currently no US Food and Drug Administration (FDA)–approved treatment options specifically indicated for patients with DT; however, 2 treatment guidelines provide recommendations on the management of DT: the NCCN Clinical Practice Guidelines In Oncology (NCCN Guidelines®) [31], and guidelines from the Desmoid Tumor Working Group (DTWG) [16].
A period of active surveillance is recommended by the NCCN Guidelines and the DTWG guidelines as the preferred front-line approach [6, 16, 31] for managing tumors that are asymptomatic or mildly symptomatic and not progressing or morbid. If there is ongoing progression of the tumor, an increase of symptoms, or higher risk of disease morbidity, the guidelines recommend treatment options depending on the anatomic location of the tumor and its potential morbidity. Surgery is limited to specific scenarios (e.g., for abdominal wall tumors) and when the morbidity of surgery is low. According to the NCCN Guidelines, in general, surgery is not considered a first-line treatment option, except in certain situations if agreed upon by a multidisciplinary tumor board. If surgery is considered, the goal should be to try to preserve function [8]. The risk of recurrence after surgery may be high in certain patients, depending on their age, tumor location, and size [18, 56,57,58]. Adjuvant radiotherapy is considered for surgery with positive margins for abdominal wall and extra-abdominal DT. Radiotherapy can also be considered for DT where recurrence would be technically challenging to resect and would lead to significant morbidity. Locoregional therapy modalities, such as cryoablation, are used to treat small- and moderate-sized extra-abdominal DT. Antihormonal therapies, such as tamoxifen and toremifene, have also been used as treatments for DT but are no longer recommended by the NCCN Guidelines or the DTWG guidelines. Systemic therapy, including low-dose chemotherapy, conventional chemotherapy, or tyrosine kinase inhibitors (sorafenib, imatinib, pazopanib, sunitinib) is used for patients with rapidly growing and symptomatic unresectable tumors or advanced disease. Treatment selection depends on how aggressive the tumor is and the need for a faster response to treatment (e.g., conventional chemotherapy will be used when a fast response is needed) [1].
Tyrosine kinase inhibitors have been evaluated in phase 2 and 3 studies, with response rates ranging from 2.6% to 10% for imatinib [59,60,61] (study population: n = 38 [60], n = 40 [61], and n = 51 [59]), 26.3–77% for sunitinib [62, 63] (study population: n = 19 [62] and n = 22 [63]), 33% for sorafenib [55] (n = 87), and 37% for pazopanib [64] (n = 72). One-year PFS rates were 66% for imatinib [59], 89% for sorafenib [55], and 86% for pazopanib [64]. Sides effects of tyrosine kinase inhibitors include neutropenia, rash, fatigue, hypertension, and abdominal pain [55, 59,60,61, 64].
Among the new agents currently under investigation for the treatment of DT, two are being evaluated in phase 3 trials. First, nirogacestat, an oral gamma-secretase inhibitor (DeFi trial, NCT03785964), has met its primary endpoint of improving progression-free survival and key secondary endpoints in patients aged ≥ 18 years with progressing or symptomatic disease, not amenable to surgery [44]. Compared with placebo, nirogacestat led to a statistically significant and clinically meaningful improvement in PFS as determined via blinded independent central review [hazard ratio for disease progression or death, 0.29 (95% CI, 0.15–0.55)] and a significantly higher rate of objective response (41%, including 7% complete response, with nirogacestat vs. 8% with placebo; P < 0.001). Improvements in PFS in favor of nirogacestat were observed across subgroups defined by tumor location (intra-abdominal and extra-abdominal), genetic mutation status (including APC), treatment status (treatment naïve and refractory/recurrent), prior tyrosine kinase inhibitor treatment, and prior surgery. Significant between-group differences were also observed in favor of nirogacestat compared with placebo for PROs including pain, disease-specific symptom burden, physical functioning, role functioning, and HRQOL. The most common adverse events in the nirogacestat group included diarrhea, nausea, fatigue, hypophosphatemia, and maculopapular rash; most adverse events were low grade [44]. And, second, oral gamma-secretase inhibitor, AL102, is being evaluated in a phase 2/3 study (RINGSIDE; NCT04871282) in patients aged ≥ 12 years (part B) with progressive DT [65].
Ongoing phase 2 trials include an open-label phase 2 study of nirogacestat (NCT04195399) in pediatric participants (aged 12 months to 18 years) with progressive unresectable DT who have failed at least 1 prior line of systemic therapy; a phase ½ study (NCT04851119) of Tegavivint (BC-2059) in patients with recurrent or refractory solid tumors, including lymphomas and DT; a phase 2 study (NCT02834013) of the combination of nivolumab and ipilimumab in patients affected by rare cancers, including DT; and a phase ½ study (NCT03802084) of the combination of vactosertib and imatinib in patients with advanced DT. Although not classified as phase 2, one study (NCT05490667) is evaluating anlotinib combined with chemotherapy in the treatment of unresectable advanced DT in Chinese patients.
Unmet Need
Few epidemiological studies providing incidence estimates of DT were identified in the literature; all these studies were conducted in European countries, and no study provided prevalence estimates. In addition, no incidence or prevalence data on children are available. Because all the epidemiological data are from European populations, a US population-based study will be necessary to compare incidence estimates between Europe and the US.
Although DT have a considerable impact on patients’ HRQOL, few studies are evaluating this aspect. Two patient-reported outcome tools (DTF-QOL and GODDESS) have recently been validated for DT [48, 52]. Additional data on the impact of DT on HRQOL are needed. In a survey of patients with DT, patients expressed that they did not want to feel like a burden on their partner or family, but there is no study evaluating caregiver burden for patients with DT.
Furthermore, two old studies [66, 67] and one recent study [44] report the functional outcomes of patients following surgery and other treatments; there is a need for additional and recent studies describing the functional outcomes of patients undergoing current treatments. We identified few real-world studies describing treatment patterns of patients with DT, but most of these studies do not clearly describe the disease outcomes after each treatment. Only two US studies [68, 69] evaluating treatment patterns in the real world were identified. One study [70] of European physician preferences for treatment of DT was published in 2018. In that study, the first-choice systemic therapy for advanced DT was antihormonal + nonsteroidal anti-inflammatory drugs (NSAIDs), for which the 2020 DTWG guidelines [16] have indicated there is no clear evidence to use as treatment of DT; few physicians (~ 7%) selected tyrosine kinase inhibitors as their first-choice. Because new data from randomized trials of sorafenib and pazopanib have been recently published, there is a need for recent real-world studies, especially in the US, that can shed light on the current most common treatments used for DT and, in particular, progressive or refractory DT.
In summary, further research is needed, preferably an international, population-based study that will integrate patient-reported outcome data with objective clinical examination, radiological findings, and, potentially, molecular characteristics. This will allow greater insight into potential prognostic factors and treatment efficacy from the patients’ perspective.
Discussion
The current review provides the first comprehensive summary of the burden of illness of DT, including clinical burden (e.g., diagnostic challenges), epidemiology, impact of disease burden on patients’ HRQOL and economic burden, treatments, and guidelines. Other reviews [1, 8, 15, 21, 71,72,73] have either focused on the diagnosis and description of the disease or provided deep summaries of the treatment options in this disease. Based on our findings, DT is a rare disease that can have a negative impact on patients, particularly in symptoms (e.g., pain, impaired mobility, disfigurement), functioning (e.g., physical, emotional, and social), and overall QOL [4]. The global incidence of DT is approximately 3–5 cases per million person-years. Desmoid tumors are typically diagnosed in young adults (highest frequency of cases between 20 and 44 years) and more frequently in women [24,25,26,27,28]. The studies also show that the incidence estimate has increased in more recent years, which may be related to an improvement in diagnostic techniques. Because of the low incidence of this disease, patients are confronted with delays in diagnosis and misdiagnosis that can cause distress due to the uncertainty and affect the clinical course of the disease [4, 6]. In addition, misdiagnosis leads to errors in management and treatment. Awareness of this disease among the clinical community is important for prompt diagnosis and timely and appropriate management.
Among symptoms experienced by patients, pain is highly prevalent (63% of patients in a survey had pain [41]) and can cause significant socio-familial and economic impact on patients, leading to loss of employment, irritability, and anxiety [41]. The emotional distress level of patients with DT was compared with that of patients with sarcoma, also a malignant connective tissue disorder [39].
No information on direct or indirect costs of DT was found in the literature; only one study has reported higher healthcare resource utilization in patients with DT than in a healthy matched cohort [24]. Studies evaluating direct medical costs and other out-of-pocket costs, as well as financial data on the impact of DT in a patient’s employment and job productivity, are needed.
Treatment modalities have evolved during the last 10 years. For most patients, surgery is no longer the preferred primary treatment and has been replaced by active surveillance or alternative treatments, such as systemic therapy. Several studies [36, 37, 74, 75] have reported spontaneous regression in patients with DT under active surveillance. Therefore, the NCCN Guidelines and DTWG guidelines recommend an initial period of active surveillance with continuous monitoring for asymptomatic tumors that do not lead to functional limitations. Antihormonal treatments and NSAIDs that used to be common first-line treatment among physicians [70] are no longer recommended by the NCCN Guidelines and DTWG guidelines. Because the use of surgery or radiation in patients with progressive, morbid, or symptomatic tumors may be associated with poor long-term functional outcomes [76], systemic therapy (chemotherapy or tyrosine kinase inhibitors) is recommended for these cases. However, none of these systemic therapies have demonstrated a statistically significant improvement in patient symptom burden, functioning, or overall QOL or have been FDA-approved specifically to treat DT. In a phase 3 trial, the investigational agent nirogacestat demonstrated significant improvements in PFS and ORR as well as in pain, disease-specific symptom severity and impact, physical functioning, role functioning, and global health status/QOL [44].
Because of the highly variable presentation and symptoms of DT, treatment requires a highly individualized approach [2,3,4, 6]. Thus, it is important that patients be evaluated by a multidisciplinary team with expertise and experience in sarcoma to optimize management. Given the limited mortality associated with DT, treatment goals should not solely focus on clinical markers, such as progression-free survival, but also consider patient-relevant endpoints, such as a reduction in DT-specific symptom burden (e.g., pain) and its impact on patients’ lives, improvement in functioning with daily activities, and overall QOL [4, 40, 41, 46, 47, 51].
Limitations
We aimed to present a current comprehensive review of DT, and therefore we conducted our key searches for the last 10 years, reviewing bibliographies of review articles to identify other key articles published before our cut-off date (e.g., epidemiological studies). However, there may be additional publications not identified in this review that provide important data for the burden of DT (e.g., articles published after the date that our search was conducted). We identified several gaps in the literature: for example, the number of publications on epidemiology, impact of disease on patients’ QOL, and economic burden was limited, which considerably impaired the assessment for burden of the disease. Specifically, no epidemiological study in the US was identified, and no study evaluating the direct or indirect costs of patients with DT was identified, which reflects the low incidence of disease. Few studies evaluating the impact of the disease on HRQOL have been published, but no study evaluating caregiver burden was identified.
Conclusions
This review characterizes the burden of illness of DT. Patients with DT face many challenges, including delayed diagnosis or misdiagnosis due to lack of awareness by patients and providers; unpredictable disease course; treatment uncertainty; treatment-related side effects; debilitating symptoms such as pain, which can limit physical and psychosocial functioning; decreased QOL; disfigurement; disability; and financial distress due to loss of employment and hospital travel costs. Due to the rarity of DT, educational gaps remain regarding the management of these tumors. There are no approved treatment options for patients with DT. For most patients, surgery is no longer the preferred first treatment option after active surveillance. It is, therefore, important that patients be evaluated by a multidisciplinary team with expertise and experience in sarcoma. This can help optimize patient management and make possible the treatment goals of clinical efficacy (e.g., progression-free survival) and improvement in patient symptom burden, functioning with daily activities, and overall QOL.
References
Napolitano A, Mazzocca A, Spalato Ceruso M, et al. Recent advances in desmoid tumor therapy. Cancers (Basel). 2020;12(8):2135. https://doi.org/10.3390/cancers12082135.
Constantinidou A, Scurr M, Judson I, Litchman C. Clinical presentation of desmoid tumors. In: Litchman C, editor. Desmoid tumors. Dordrecht, the Netherlands: Springer; 2012. p. 5–16.
Kasper B, Ströbel P, Hohenberger P. Desmoid tumors: clinical features and treatment options for advanced disease. Oncologist. 2011;16(5):682–93. https://doi.org/10.1634/theoncologist.2010-0281.
Husson O, Younger E, Dunlop A, et al. Desmoid fibromatosis through the patients’ eyes: time to change the focus and organisation of care? Support Care Cancer. 2019;27(3):965–80. https://doi.org/10.1007/s00520-018-4386-8.
MedlinePlus. National Library of Medicine. Desmoid tumor. 18 August 2020. https://medlineplus.gov/genetics/condition/desmoid-tumor/. Accessed 13 December 2021.
Kasper B, Baumgarten C, Garcia J, et al. An update on the management of sporadic desmoid-type fibromatosis: a European Consensus Initiative between Sarcoma Patients EuroNet (SPAEN) and European Organization for Research and Treatment of Cancer (EORTC)/Soft Tissue and Bone Sarcoma Group (STBSG). Ann Oncol. 2017;28(10):2399–408. https://doi.org/10.1093/annonc/mdx323.
Penel N, Chibon F, Salas S. Adult desmoid tumors: biology, management and ongoing trials. Curr Opin Oncol. 2017;29(4):268–74. https://doi.org/10.1097/CCO.0000000000000374.
Garcia-Ortega DY, Martín-Tellez KS, Cuellar-Hubbe M, et al. Desmoid-type fibromatosis. Cancers (Basel). 2020;12(7):1851. https://doi.org/10.3390/cancers12071851.
Kim HA, Koo BK, Cho JH, et al. Notch1 counteracts WNT/β-catenin signaling through chromatin modification in colorectal cancer. J Clin Invest. 2012;122(9):3248–59. https://doi.org/10.1172/jci61216.
Peignon G, Durand A, Cacheux W, et al. Complex interplay between β-catenin signalling and Notch effectors in intestinal tumorigenesis. Gut. 2011;60(2):166–76. https://doi.org/10.1136/gut.2009.204719.
Ungerbäck J, Elander N, Grünberg J, Sigvardsson M, Söderkvist P. The Notch-2 gene is regulated by Wnt signaling in cultured colorectal cancer cells. PLoS One. 2011;6(3): e17957. https://doi.org/10.1371/journal.pone.0017957.
Rodilla V, Villanueva A, Obrador-Hevia A, et al. Jagged1 is the pathological link between Wnt and Notch pathways in colorectal cancer. Proc Natl Acad Sci U S A. 2009;106(15):6315–20. https://doi.org/10.1073/pnas.0813221106.
Fre S, Pallavi SK, Huyghe M, et al. Notch and Wnt signals cooperatively control cell proliferation and tumorigenesis in the intestine. Proc Natl Acad Sci U S A. 2009;106(15):6309–14. https://doi.org/10.1073/pnas.0900427106.
Shang H, Braggio D, Lee YJ, et al. Targeting the Notch pathway: a potential therapeutic approach for desmoid tumors. Cancer. 2015;121(22):4088–96. https://doi.org/10.1002/cncr.29564.
Skubitz KM. Biology and treatment of aggressive fibromatosis or desmoid tumor. Mayo Clin Proc. 2017;92(6):947–64. https://doi.org/10.1016/j.mayocp.2017.02.012.
DTWG. Desmoid Tumor Working Group. The management of desmoid tumours: a joint global consensus-based guideline approach for adult and paediatric patients. Eur J Cancer. 2020;127:96–107. https://doi.org/10.1016/j.ejca.2019.11.013.
Penel N, Le Cesne A, Bonvalot S, et al. Surgical versus non-surgical approach in primary desmoid-type fibromatosis patients: a nationwide prospective cohort from the French Sarcoma Group. Eur J Cancer. 2017;83:125–31. https://doi.org/10.1016/j.ejca.2017.06.017.
He XD, Zhang YB, Wang L, et al. Prognostic factors for the recurrence of sporadic desmoid-type fibromatosis after macroscopically complete resection: analysis of 114 patients at a single institution. Eur J Surg Oncol. 2015;41(8):1013–9. https://doi.org/10.1016/j.ejso.2015.04.016.
Tsagozis P, Stevenson JD, Grimer R, Carter S. Outcome of surgery for primary and recurrent desmoid-type fibromatosis. A retrospective case series of 174 patients. Ann Med Surg (Lond). 2017;17:14–9. https://doi.org/10.1016/j.amsu.2017.03.023.
van Broekhoven DL, Verhoef C, Elias SG, et al. Local recurrence after surgery for primary extra-abdominal desmoid-type fibromatosis. Br J Surg. 2013;100(9):1214–9. https://doi.org/10.1002/bjs.9194.
Zhang Z, Shi J, Yang T, Liu T, Zhang K. Management of aggressive fibromatosis. Oncol Lett. 2021;21(1):43. https://doi.org/10.3892/ol.2020.12304.
Riedel RF, Agulnik M. Evolving strategies for management of desmoid tumor. Cancer. 2022;128(16):3027–40. https://doi.org/10.1002/cncr.34332.
Federman N. Molecular pathogenesis of desmoid tumor and the role of γ-secretase inhibition. NPJ Precis Oncol. 2022;6(1):62. https://doi.org/10.1038/s41698-022-00308-1.
Anneberg M, Svane HML, Fryzek J, et al. The epidemiology of desmoid tumors in Denmark. Cancer Epidemiol. 2022;77: 102114. https://doi.org/10.1016/j.canep.2022.102114.
Nieuwenhuis MH, Casparie M, Mathus-Vliegen LM, Dekkers OM, Hogendoorn PC, Vasen HF. A nation-wide study comparing sporadic and familial adenomatous polyposis-related desmoid-type fibromatoses. Int J Cancer. 2011;129(1):256–61. https://doi.org/10.1002/ijc.25664.
Orphanet Report Series. Prevalence and incidence of rare diseases: bibliographic data. January 2019. http://www.orpha.net/orphacom/cahiers/docs/GB/Prevalence_of_rare_diseases_by_diseases.pdf. Accessed 3 January 2022.
Reitamo JJ, Häyry P, Nykyri E, Saxén E. The desmoid tumor. I. Incidence, sex-, age- and anatomical distribution in the Finnish population. Am J Clin Pathol. 1982;77(6):665–73. https://doi.org/10.1093/ajcp/77.6.665.
van Broekhoven DL, Grünhagen DJ, den Bakker MA, van Dalen T, Verhoef C. Time trends in the incidence and treatment of extra-abdominal and abdominal aggressive fibromatosis: a population-based study. Ann Surg Oncol. 2015;22(9):2817–23. https://doi.org/10.1245/s10434-015-4632-y.
Debaudringhien M, Blay JY, Bimbai AM, et al. Association between recent pregnancy or hormonal contraceptive exposure and outcome of desmoid-type fibromatosis. ESMO Open. 2022;7(5): 100578. https://doi.org/10.1016/j.esmoop.2022.100578.
Sinha A, Tekkis PP, Gibbons DC, Phillips RK, Clark SK. Risk factors predicting desmoid occurrence in patients with familial adenomatous polyposis: a meta-analysis. Colorectal Dis. 2011;13(11):1222–9. https://doi.org/10.1111/j.1463-1318.2010.02345.x.
Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Soft Tissue Sarcoma V.1.2023. © National Comprehensive Cancer Network, Inc. 2023. All rights reserved. Accessed March 20, 2023. To view the most recent and complete version of the guideline, go online to NCCN.org.
Gounder M. The Desmoid Tumor Research Foundation. Diagnosis and treatment. 2021. https://dtrf.org/diagnosis-and-treatment/. Accessed 13 December 2021.
Penel N, Coindre JM, Bonvalot S, et al. Management of desmoid tumours: a nationwide survey of labelled reference centre networks in France. Eur J Cancer. 2016;58:90–6. https://doi.org/10.1016/j.ejca.2016.02.008.
Huss S, Nehles J, Binot E, et al. β-Catenin (CTNNB1) mutations and clinicopathological features of mesenteric desmoid-type fibromatosis. Histopathology. 2013;62(2):294–304. https://doi.org/10.1111/j.1365-2559.2012.04355.x.
Mercier K, Hernandez L, Braggio D, Lucas A. Update on diagnostic data from the Desmoid Tumor Research Foundation. Presented at the National Organization for Rare Disorders (NORD) Breakthrough Summit; 8–9 October 2020. Virtual.
Colombo C, Miceli R, Le Péchoux C, et al. Sporadic extra abdominal wall desmoid-type fibromatosis: surgical resection can be safely limited to a minority of patients. Eur J Cancer. 2015;51(2):186–92. https://doi.org/10.1016/j.ejca.2014.11.019.
Bonvalot S, Ternès N, Fiore M, et al. Spontaneous regression of primary abdominal wall desmoid tumors: more common than previously thought. Ann Surg Oncol. 2013;20(13):4096–102. https://doi.org/10.1245/s10434-013-3197-x.
Esplen MJ, Berk T, Butler K, Gallinger S, Cohen Z, Trinkhaus M. Quality of life in adults diagnosed with familial adenomatous polyposis and desmoid tumor. Dis Colon Rectum. 2004;47(5):687–96. https://doi.org/10.1007/s10350-003-0121-7.
Ingley KM, Klein R, Theobalds N, et al. High prevalence of persistent emotional distress in desmoid tumor. Psychooncology. 2020;29(2):311–20. https://doi.org/10.1002/pon.5250.
Timbergen MJM, van de Poll-Franse LV, Grünhagen DJ, et al. Identification and assessment of health-related quality of life issues in patients with sporadic desmoid-type fibromatosis: a literature review and focus group study. Qual Life Res. 2018;27(12):3097–111. https://doi.org/10.1007/s11136-018-1931-3.
Rigaux P, Lefebvre-Kuntz D, Penel N. Pain burden in desmoid tumor patients: a survey of the French advocacy group SOS desmoid. Bull Cancer. 2015;102(3):213–6. https://doi.org/10.1016/j.bulcan.2015.02.001.
Penel N, Bonvalot S, Bimbai AM, et al. 1512P Pain in patients with desmoid fibromatosis (DF). Ann Oncol. 2022;33(Suppl 7):S1238. https://doi.org/10.1016/j.annonc.2022.07.1615.
Penel N, Bonvalot S, Le Deley MC, et al. Pain in desmoid-type fibromatosis: prevalence, determinants, and prognosis value. Int J Cancer. 2023. https://doi.org/10.1002/ijc.34493.
Gounder M, Ratan R, Alcindor T, et al. Nirogacestat, a gamma-secretase inhibitor for desmoid tumors. N Engl J Med. 2023;388(10):898–912. https://doi.org/10.1056/NEJMoa2210140.
Garg V, Rastogi S, Kalra K, et al. Health-related quality of life (HRQoL), anxiety, and depression in patients with desmoid type fibromatosis. Support Care Cancer. 2022;30(12):10089–98. https://doi.org/10.1007/s00520-022-07445-0.
Duhil de Bénazé G, Vigan M, Corradini N, et al. Functional analysis of young patients with desmoid-type fibromatosis: initial surveillance does not jeopardize long term quality of life. Eur J Surg Oncol. 2020;46(7):1294–300. https://doi.org/10.1016/j.ejso.2020.02.028.
Garg V, Rastogi S, Barwad A, Panday R, Bhoriwal SK, Dhamija E. Patient reported outcomes in patients with desmoid type fibromatosis. J Clin Oncol. 2021;39(15 Suppl):11574. https://doi.org/10.1200/JCO.2021.39.15_suppl.11574.
Schut A, Timbergen M, Lidington E, et al. The evaluation of health related quality of life issues experienced by patients with desmoid type fibromatosis: the QUALIFIED study. P227. Presented at the Connective Tissue Oncology Society; 10–13 November 2021. Virtual.
Schut AW, Lidington E, Timbergen MJM, et al. Development of a disease-specific health-related quality of life questionnaire (DTF-QoL) for patients with desmoid-type fibromatosis. Cancers (Basel). 2022;14(3):709. https://doi.org/10.3390/cancers14030709.
Schut AW, Lidington E, Timbergen MJM, et al. Unraveling desmoid-type fibromatosis-specific health-related quality of life: who is at risk for poor outcomes. Cancers (Basel). 2022;14(12):2979. https://doi.org/10.3390/cancers14122979.
Gounder MM, Maddux L, Paty J, Atkinson TM. Prospective development of a patient-reported outcomes instrument for desmoid tumors or aggressive fibromatosis. Cancer. 2020;126(3):531–9. https://doi.org/10.1002/cncr.32555.
Gounder M, Atkinson TM, Bell T, et al. Psychometric properties and meaningful change thresholds (MCT) of the Gounder/desmoid tumor research foundation desmoid symptom/impact scale (GODDESS) as assessed in the phase 3 DeFi trial (Paper 81). Presented at the Connective Tissue Oncology Society (CTOS) Annual Meeting; 16–19 November 2022. Vancouver, Canada.
Gounder M, Ratan R, Alcindor T, et al. Supplementary appendix. Nirogacestat, a γ-secretase inhibitor for desmoid tumors. N Engl J Med. 2023;388(10):898–912. https://doi.org/10.1056/NEJMoa2210140.
Johns MS, Merritt WT 3rd, Rhodes L, et al. A cost analysis of sorafenib for desmoid tumors. J Oncol Pharm Pract. 2022. https://doi.org/10.1177/10781552221077927.
Gounder MM, Mahoney MR, Van Tine BA, et al. Sorafenib for advanced and refractory desmoid tumors. N Engl J Med. 2018;379(25):2417–28. https://doi.org/10.1056/NEJMoa1805052.
Peng PD, Hyder O, Mavros MN, et al. Management and recurrence patterns of desmoids tumors: a multi-institutional analysis of 211 patients. Ann Surg Oncol. 2012;19(13):4036–42. https://doi.org/10.1245/s10434-012-2634-6.
Seinen JM, Niebling MG, Bastiaannet E, Pras B, Hoekstra HJ. Four different treatment strategies in aggressive fibromatosis: a systematic review. Clin Transl Radiat Oncol. 2018;12:1–7. https://doi.org/10.1016/j.ctro.2018.03.001.
Yang T, Liu H, Liao Z, Zhang C, Xiang L, Yang J. Postoperative adjuvant radiotherapy can delay the recurrence of desmoid tumors after R0 resection in certain subgroups. Front Surg. 2021;8: 697793. https://doi.org/10.3389/fsurg.2021.697793.
Chugh R, Wathen JK, Patel SR, et al. Efficacy of imatinib in aggressive fibromatosis: results of a phase II multicenter Sarcoma Alliance for Research through Collaboration (SARC) trial. Clin Cancer Res. 2010;16(19):4884–91. https://doi.org/10.1158/1078-0432.Ccr-10-1177.
Kasper B, Gruenwald V, Reichardt P, et al. Imatinib induces sustained progression arrest in RECIST progressive desmoid tumours: final results of a phase II study of the German Interdisciplinary Sarcoma Group (GISG). Eur J Cancer. 2017;76:60–7. https://doi.org/10.1016/j.ejca.2017.02.001.
Penel N, Le Cesne A, Bui BN, et al. Imatinib for progressive and recurrent aggressive fibromatosis (desmoid tumors): an FNCLCC/French Sarcoma Group phase II trial with a long-term follow-up. Ann Oncol. 2011;22(2):452–7. https://doi.org/10.1093/annonc/mdq341.
Jo JC, Hong YS, Kim KP, et al. A prospective multicenter phase II study of sunitinib in patients with advanced aggressive fibromatosis. Invest New Drugs. 2014;32(2):369–76. https://doi.org/10.1007/s10637-013-0059-0.
Miano ST, Francini G, Civitelli S, Petrioli R, Francini E. Clinical outcomes of sunitinib (Su) for patients (pts) with desmoid tumors (DT). J Clin Oncol. 2019;37(15 Suppl):11052. https://doi.org/10.1200/JCO.2019.37.15_suppl.11052.
Toulmonde M, Pulido M, Ray-Coquard I, et al. Pazopanib or methotrexate-vinblastine combination chemotherapy in adult patients with progressive desmoid tumours (DESMOPAZ): a non-comparative, randomised, open-label, multicentre, phase 2 study. Lancet Oncol. 2019;20(9):1263–72. https://doi.org/10.1016/s1470-2045(19)30276-1.
Gounder M, Robin RL, Chugh R, et al. Initial results of RINGSIDE, a phase 2/3 trial of AL102 for the treatment of desmoid tumors. Presented at the Connective Tissue Oncology Society (CTOS) Annual Meeting; 16–19 November 2022. Vancouver, BC, Canada.
Catton CN, O’Sullivan B, Bell R, Cummings B, Fornasier V, Panzarella T. Aggressive fibromatosis: optimisation of local management with a retrospective failure analysis. Radiother Oncol. 1995;34(1):17–22. https://doi.org/10.1016/0167-8140(94)01483-j.
Gaposchkin CG, Bilsky MH, Ginsberg R, Brennan MF. Function-sparing surgery for desmoid tumors and other low-grade fibrosarcomas involving the brachial plexus. Neurosurgery. 1998;42(6):1297–301. https://doi.org/10.1097/00006123-199806000-00058. (discussion 301–303).
Jagosky M, Anderson C, Squires M, et al. Clinical features and treatment outcomes of patients with desmoid tumors: a large single institution retrospective series. Presented at the Connective Tissue Oncology Society (CTOS) Annual Meeting; 16–19 November 2022. Vancouver, Canada.
Testa S, Bui NQ, Charville GW, et al. Management of patients with newly diagnosed desmoid tumors in a first-line setting. Cancers (Basel). 2022. https://doi.org/10.3390/cancers14163907.
Schöffski P, Requilé A, van Cann T. Assessment of physician’s systemic treatment preferences for patients with advanced desmoid-type fibromatosis: experience-based medicine in the absence of high-level evidence. Oncol Res Treat. 2018;41(4):214–9. https://doi.org/10.1159/000486514.
Martínez Trufero J, Pajares Bernad I, Torres Ramón I, Hernando Cubero J, Pazo CR. Desmoid-type fibromatosis: who, when, and how to treat. Curr Treat Options Oncol. 2017;18(5):29. https://doi.org/10.1007/s11864-017-0474-0.
Penel N, Kasper B, van Der Graaf WTA. Desmoid-type fibromatosis: toward a holistic management. Curr Opin Oncol. 2021;33(4):309–14. https://doi.org/10.1097/cco.0000000000000743.
Pandrowala S, Jones RL, Gupta S, Gulia A. Desmoid fibromatosis: is the current picture changing? Future Oncol. 2021;17(25):3397–408. https://doi.org/10.2217/fon-2021-0003.
Schut AW, Timbergen MJM, van Broekhoven DLM, et al. A nationwide prospective clinical trial on active surveillance in patients with non-intra-abdominal desmoid-type fibromatosis: the GRAFITI trial. Ann Surg. 2022. https://doi.org/10.1097/sla.0000000000005415.
Colombo C, Fiore M, Grignani G, et al. A prospective observational study of active surveillance in primary desmoid fibromatosis. Clin Cancer Res. 2022. https://doi.org/10.1158/1078-0432.Ccr-21-4205.
Newman ET, Lans J, Kim J, et al. PROMIS function scores are lower in patients who underwent more aggressive local treatment for desmoid tumors. Clin Orthop Relat Res. 2020;478(3):563–77. https://doi.org/10.1097/corr.0000000000000918.
Timbergen MJM, Schut AW, Grünhagen DJ, Sleijfer S, Verhoef C. Active surveillance in desmoid-type fibromatosis: a systematic literature review. Eur J Cancer. 2020;137:18–29. https://doi.org/10.1016/j.ejca.2020.06.022.
Smith K, Desai J, Lazarakis S, Gyorki D. Systematic review of clinical outcomes following various treatment options for patients with extraabdominal desmoid tumors. Ann Surg Oncol. 2018;25(6):1544–54. https://doi.org/10.1245/s10434-018-6408-7.
Kim Y, Rosario MS, Cho HS, Han I. Factors associated with disease stabilization of desmoid-type fibromatosis. Clin Orthop Surg. 2020;12(1):113–9. https://doi.org/10.4055/cios.2020.12.1.113.
Fiore M, Crago A, Gladdy R, Kasper B. The landmark series: desmoid. Ann Surg Oncol. 2021;28(3):1682–9. https://doi.org/10.1245/s10434-020-09395-5.
Turner B, Alghamdi M, Henning JW, et al. Surgical excision versus observation as initial management of desmoid tumors: a population based study. Eur J Surg Oncol. 2019;45(4):699–703. https://doi.org/10.1016/j.ejso.2018.09.015.
Mueller C, Croner R, Klein P, Grützmann R, Vassos N. Primary and recurrent sporadic desmoids: prognostic factors influencing recurrence-free survival after complete gross resection. Int J Surg. 2016;31:63–70. https://doi.org/10.1016/j.ijsu.2016.05.068.
Janssen ML, van Broekhoven DL, Cates JM, et al. Meta-analysis of the influence of surgical margin and adjuvant radiotherapy on local recurrence after resection of sporadic desmoid-type fibromatosis. Br J Surg. 2017;104(4):347–57. https://doi.org/10.1002/bjs.10477.
Krieg AH, Wirth C, Lenze U, et al. Extra-abdominal desmoid tumours—further evidence for the watchful waiting policy. Swiss Med Wkly. 2019;149:w20107. https://doi.org/10.4414/smw.2019.20107.
Ratan R, Roland CL, Bishop AJ. Desmoid fibromatosis: management in an era of increasing options. Curr Oncol Rep. 2021;23(4):41. https://doi.org/10.1007/s11912-021-01026-w.
Bishop AJ, Zarzour MA, Ratan R, et al. Long-term outcomes for patients with desmoid fibromatosis treated with radiation therapy: a 10-year update and re-evaluation of the role of radiation therapy for younger patients. Int J Radiat Oncol Biol Phys. 2019;103(5):1167–74. https://doi.org/10.1016/j.ijrobp.2018.12.012.
Redifer Tremblay K, Lea WB, Neilson JC, King DM, Tutton SM. Percutaneous cryoablation for the treatment of extra-abdominal desmoid tumors. J Surg Oncol. 2019;120(3):366–75. https://doi.org/10.1002/jso.25597.
Ghanouni P, Dobrotwir A, Bazzocchi A, et al. Magnetic resonance-guided focused ultrasound treatment of extra-abdominal desmoid tumors: a retrospective multicenter study. Eur Radiol. 2017;27(2):732–40. https://doi.org/10.1007/s00330-016-4376-5.
Shi Y, Huang Y, Zhou M, Ying X, Hu X. High-intensity focused ultrasound treatment for intra-abdominal desmoid tumors: a report of four cases. J Med Ultrason (2001). 2016;43(2):279–84. https://doi.org/10.1007/s10396-015-0682-9.
Ilaslan H, Schils J, Joyce M, Marks K, Sundaram M. Radiofrequency ablation: another treatment option for local control of desmoid tumors. Skeletal Radiol. 2010;39(2):169–73. https://doi.org/10.1007/s00256-009-0807-6.
Azzarelli A, Gronchi A, Bertulli R, et al. Low-dose chemotherapy with methotrexate and vinblastine for patients with advanced aggressive fibromatosis. Cancer. 2001;92(5):1259–64. https://doi.org/10.1002/1097-0142(20010901)92:5%3c1259::aid-cncr1446%3e3.0.co;2-y.
Skapek SX, Ferguson WS, Granowetter L, et al. Vinblastine and methotrexate for desmoid fibromatosis in children: results of a Pediatric Oncology Group phase II trial. J Clin Oncol. 2007;25(5):501–6. https://doi.org/10.1200/jco.2006.08.2966.
Palassini E, Frezza AM, Mariani L, et al. Long-term efficacy of methotrexate plus vinblastine/vinorelbine in a large series of patients affected by desmoid-type fibromatosis. Cancer J. 2017;23(2):86–91. https://doi.org/10.1097/ppo.0000000000000254.
Weiss AJ, Horowitz S, Lackman RD. Therapy of desmoid tumors and fibromatosis using vinorelbine. Am J Clin Oncol. 1999;22(2):193–5. https://doi.org/10.1097/00000421-199904000-00020.
SpringWorks press release. SpringWorks Therapeutics, Inc. SpringWorks Therapeutics announces nirogacestat achieved primary and all key secondary endpoints in phase 3 DeFi trial in adult patients with progressing desmoid tumors. 24 May 2022. https://ir.springworkstx.com/news-releases/news-release-details/springworks-therapeutics-announces-nirogacestat-achieved-primary. Accessed 28 July 2022.
Acknowledgements
Funding
SpringWorks Therapeutics, Inc., provided funding to RTI Health Solutions for conducting this study and developing the manuscript. SpringWorks Therapeutics Inc. was involved in reviewing the manuscript and funded the Rapid Service Fee.
Medical Writing, Editorial, and Other Assistance
Medical writing services were provided by RTI Health Solutions, funded by SpringWorks Therapeutics, Inc. The authors thank John Forbes, Medical Editor at RTI Health Solutions, for his contributions of editorial revisions of this manuscript, and Jennifer Han from SpringWorks Therapeutics, Inc., for reviewing the manuscript.
Author Contributions
This research was developed under a research contract between RTI Health Solutions (Meryem Bektas, Shahnaz Khan, Maria Fernandez, and Catriona Heyes) and SpringWorks Therapeutics (Timothy Bell, Brad Tumminello, and Ana B. Oton) and was funded by SpringWorks Therapeutics, Inc. SpringWorks Therapeutics, Inc. led the concept design of this publication, review and interpretation, approval, and decision to publish. RTI performed the literature search, data analysis, and drafted the manuscript.
Prior Presentation
Parts of this manuscript have been presented as posters at the Desmoid Tumor Research Foundation Conference in 23–25 September 2022 (virtual) and at the Connective Tissue Oncology Society 2022 Annual Meeting, November 16–19, in Vancouver Canada (abstract ID: 2206524 and poster ID: P 260).
Disclosures
Timothy Bell, Ana B. Oton, and Brad Tumminello are employees of SpringWorks Therapeutics, Inc. Shahnaz Khan, Catriona Heyes, and Meryem Bektas are employees of RTI Health Solutions. Maria Fernandez is a former employer of RTI Health Solutions.
Compliance with Ethics Guidelines
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Data Availability
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Author information
Authors and Affiliations
Corresponding author
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Bektas, M., Bell, T., Khan, S. et al. Desmoid Tumors: A Comprehensive Review. Adv Ther 40, 3697–3722 (2023). https://doi.org/10.1007/s12325-023-02592-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-023-02592-0