
Abstract
Introduction
Dalcinonacog alfa (DalcA), a novel subcutaneously administered recombinant human factor IX (FIX) variant is being developed for adult and paediatric patients with hemophilia B (HB). DalcA has been shown to raise FIX to clinically meaningful levels in adults with HB. This work aimed to support dosing regimen selection in adults and perform first-in-paediatric dose extrapolations using a model-based pharmacokinetic (PK) approach.
Methods
A population PK model was built using adult data from two clinical trials (NCT03186677, NCT03995784). With allometry in the model, clinical trial simulations were performed to study alternative dosing regimens in adults and children. Steady-state trough levels and the time-to-reach target were derived to inform dose selection.
Results
Almost 90% of the adults were predicted to achieve desirable FIX levels, i.e. 10% FIX activity, following daily 100 IU/kg dosing, with 90% of the subjects reaching target within 1.6–7.1 days. No every-other-day regimen met the target. A dose of 125 IU/kg resulted in adequate FIX levels down to 6 years, whereas a 150 IU/kg dose was needed below 6 down to 2 years of age. For subjects down to 6 years that did not reach target with 125 IU/kg, a dose escalation to 150 IU/kg was appropriate. The children below 6 to 2 years were shown to need a dose escalation to 200 IU/kg if 150 IU/kg given daily was insufficient.
Conclusion
This study supported the adult dose selection for DalcA in the presence of sparse data and enabled first-in-paediatric dose selection to achieve FIX levels that reduce risk of spontaneous bleeds.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Despite sparse data which is common for rare diseases, a clinical population pharmacokinetic model was successfully developed for a novel hemostatic drug. |
Using the developed model and general clinical guidelines for factor IX levels, dose selection in adults was supported. |
Using the adult data and model, first-in-paediatric dose selection was supported through allometric scaling with fixed exponents. |
The work demonstrates the utility of population pharmacokinetic modelling for a serious and rare disease such as hemophilia B. |
Introduction
Hemophilia B (HB) is a rare sex-linked bleeding disorder caused by deficiency in factor IX (FIX) [1] that causes spontaneous and traumatic bleeding. Current standard of care is to provide missing FIX by intravenous (IV) replacement therapy [2]. Recently, recombinant FIX (rFIX) products with long half-life have enabled weekly to every-2-weekly treatment, which has significantly improved treatment [3]. However, variability in the potential of bleeding prevention, and the need for administration by healthcare professionals in some cases is inconvenient for adults and children. A good alternative to IV infusions is subcutaneous (SC) administration that can be performed by the patient or caregiver, providing advantages with respect to quality of life and reduction in healthcare burden and cost.
Dalcinonacog alfa (DalcA) is a novel rFIX variant that is being developed as a subcutaneous formulation for prophylactic treatment of bleeding episodes in patients with HB. It has previously been studied in phase 1/2a and phase 2b for evaluation of pharmacokinetics (PK), pharmacodynamics (PD), safety and tolerability in adult patients with HB [4, 5]. DalcA has shown a promising PK, efficacy and safety profile [4]. The results in adults have indicated that DalcA is effective in raising FIX levels into ranges that correspond to the phenotypic definition of mild hemophilia, i.e. ≥ 0.1 IU/mL [6], in which spontaneous bleeds are uncommon compared to severe forms of hemophilia [7].
As a result of the rarity of the disease, clinical trials in hemophilia suffer from small sample sizes. In particular, finding eligible paediatric subjects can be a limiting factor in clinical development programs. Another issue when developing prophylactic hemophilia treatments is the efficacy endpoint that is commonly used, namely annualized bleeding rate (ABR). Theoretically, it is a direct measure of clinical benefit; however, in practice, identifying bleeding events can be hard and this will affect the reported ABR [8]. In addition, the definition of a bleeding event in trials varies between and within different product classes which compromises adequate comparison [9]. Usage of more objective endpoints is warranted, such as FIX activity levels, which were used in the DalcA phase 2b trial [5, 8, 10]. The use of factor activity levels as a surrogate for efficacy is currently not validated and a quantitative relationship between steady-state activity levels and bleeding outcomes is needed for a given product [8].
Hemophilia is prevalent in both adults and children. Thus, after clinical proof-of-concept has been obtained in adults, a paediatric program needs to be considered [11, 12]. Population PK models built on adult data are useful for characterizing the dose–concentration relationship in adults and aid in extrapolation to children to increase the likelihood of establishing adequate FIX levels by prophylaxis. A model-based analysis of PK data also enables quantification of the inter-individual variability in PK parameters, enabling clinical trial simulations to study different dosing regimens in larger populations. Furthermore, using allometric scaling methods [13], an informed first-in-paediatric dose can be selected, as previously shown [14]. Especially for children down to 2 years of age, this method has been shown to be useful for initiation of a paediatric trial for coagulation factors FVIII and FIX [14]. As phenotypic differences in patients with hemophilia are based on factor activity levels, the target to ensure patients transitioning from severe forms into mild forms is defined. Using the same target for adults and children, clinical trial simulations including allometric scaling are useful to investigate if a one-dose-fits-all approach is adequate, or if a stratified dosing approach based on age ranges is needed to ensure desirable activity levels in coming clinical trials. Dosing for other rFIX products indicates that dosing adjustment might be needed in paediatric patients as a shorter half-life and a higher clearance per kilogram of body weight have been observed [15].
DalcA PK data following IV and SC administration was pooled from two clinical trials [4, 5] in adults and used for building a population PK model to characterize the PK in adults and to extrapolate to exposure in children. The model was used for clinical trial simulations to support the dose selection of prophylactic treatment with DalcA in adults and children down to 2 years of age with HB.
Materials and Methods
Study Design and Patients
The PK data used in this analysis came from two separate open-label trials in which DalcA was studied in previously treated, adult patients with severe HB. One of the studies was a phase 1/2 dose-escalation trial (ISU-301, [NCT03186677]) [4] and the other was a phase 2b prophylaxis study to evaluate PK, PD, safety and tolerability (DLZ-201, [NCT03995784]) [5]. The phase 1/2 trial consisted of five cohorts. Patients in cohort 1 were given a single IV dose of 70 IU/kg. In cohorts 2–3, IV doses of 70 IU/kg were followed by 70 IU/kg or 140 IU/kg single SC dose 4 days after the IV dose. Patients in cohort 4 were given daily SC dosing (140 IU/kg) for 6 days. For patients in cohort 5, a single IV dose of 70 IU/kg was given followed by 8 days of SC dosing (140 IU/kg). PK samples following IV administration were taken pre-dose and at 0.25, 0.5, 1, 3, 6, 9, 24, 48 and 72 h post dose. Following SC dosing, samples were taken pre-dose and at 1, 2, 4, 6, 8, 10, 12, 24, 48 and 72 h post dose. For cohort 5, samples were taken at pre-dose and 6 h after the first injection and after the 6th injection, and at 24 h post dose for all doses given after the 6th injection. In the phase 2b trial (referred to as cohort 6), a single IV dose on the first day (50 IU/kg) was given followed by 28 days of daily SC dosing (100 IU/kg) starting 35 min after the IV dose. One individual received a 150 IU/kg IV dose on the first day and another individual received a lower SC dose (50 IU/kg) than planned on the first two doses. Samples were taken pre-dose on days 2, 3, 7, 14, 21 and 28, and washout sampling was performed 24, 48, 72, 96 and 120 h after the last dose and at end of study.
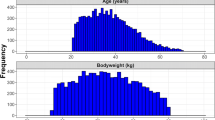
The total number of subjects was 21 (male), with 303 observations. The median body weight and 10–90th percentile range were 67 (61–81) kg, respectively. The median age and 10–90th percentile range were 43 (26–57) years, respectively. The proportion of samples below the quantification limit (BLQ) was 2.9%. For all BLQ PK observations in the elimination phase, the first BLQ sample in an individual PK profile was set to LOQ (limit of quantitation)/2 whereas the remaining BLQ samples within a subject’s PK profile were omitted. For the absorption PK phase, the opposite was applied.
Drug Quantification
Details around how FIX activity was measured can be found in the Supplementary Material.
Model Building
For a simple one-compartment model (with first-order absorption kinetics when SC data was included), relevant PK parameters were estimated using only IV, SC and IV with SC data simultaneously. The resulting parameter estimates were compared and it was concluded that modelling IV and SC data simultaneously was informative without biasing CL and V estimates by including SC data. One-, two- and three-compartment models were explored for all data. Inter-individual variability (IIV) was tested in all parameters. Covariance was tested in appropriate model parameters. Baseline levels of endogenous FIX were modelled as additive to the concentrations of FIX. The individual prediction of FIX concentrations (IPRED) was expressed as:
in which BASE is endogenous FIX levels in a typical patient and IIVbase is the IIV in BASE. A is the amount in the central compartment and Vc is the volume of distribution of the central compartment. Allometric scaling was employed in all clearance and volume terms with fixed exponents of 0.75 and 1 [13], respectively:
where TVCL and TVVc are typical clearance and volume of distribution values in the central compartment, respectively. Scaling was done using 70 kg body weight. After addition of allometric scaling into the model, non-linear elimination was tested. Lastly, inter-occasional variability (IOV) was tested for all PK parameters. All supported IIV and/or IOV parameters were re-evaluated in a backward exclusion step.
Subsequently, trial and age were tested as covariates for CL, Vc, BASE, Q, Vp, ka, F and body weight as a covariate on BASE, ka, and F as it was already included on clearance and volume terms through the allometric function. The covariate search was performed using the stepwise covariate modelling (SCM) approach [16]. Statistical significance was tested (p = 0.05) for the forward search, followed by a stricter criterion (p = 0.01) in the backward evaluation.
Model Evaluation
Discrimination between models was done on the basis of several criteria and a detailed description can be found in the Supplementary Material.
Dosing Regimen Exploration to Change the Hemophilic Phenotype to Mild
The predefined target in all simulations was based on reaching factor levels corresponding to mild hemophilia phenotypic status and was set to 0.1 IU/mL [6, 7, 17, 18]. The target was not age-dependent and was as such the same in the adult and paediatric simulations.
In adults, 1000 individuals were used for simulation of different dosing regimens given once daily (50, 75, 90, 100 IU/kg [OD]) or given every other day (125, 150 IU/kg [EOD]). Rich PK profiles were simulated over 40 days and trough levels for each dosing regimen were derived. Subsequently, the percentage of the population at or above the target over time was identified on the basis of steady-state trough levels (Cmin,ss) for each dosing regimen. In addition, the median and 90% prediction interval (PI) of Cmin,ss were derived for each OD regimen. Furthermore, the median and 90% PI were calculated for the time-to-reach at or above the target for all OD doses across all 1000 individuals.
The National Health and Nutrition Examination Survey (NHANES) dataset of the US Centers for Disease Control and Prevention (CDC) was used as source for age-body weight pairs in paediatrics. The paediatric simulations were performed after the adult simulations to have the adult results for comparison, and were based on age groups 11, 6, 4 and 2 years of age (n = 1000 per age group). Rich concentration PK profiles were simulated over 40 days using different daily dosing regimens (100, 125 and 150 IU/kg). On the basis of the PK simulations, the median and 90% PI of Cmin,ss levels were derived for all dose levels and age groups. As the paediatric dose evaluation was intended to support a first-in-paediatric trial setting, a potential dose escalation to 175 or 200 IU/kg was studied for the subjects that did not reach the target FIX levels at steady state.
Ethics
The studies were conducted in accordance with the Declaration of Helsinki and US Code of Federal Regulations, International Conference on Harmonisation Guidelines on Good Clinical Practices, and South Korean national laws and regulations. Both study protocols were reviewed and approved by the institutional review board or independent ethics committee at each study site. All participants provided informed consent prior to enrolment [4, 5].
Results
Model Development
The base population PK model was a two-compartmental disposition model with first-order absorption and elimination. IIV was supported for CL, BASE and ka. Covariance was statistically significant as a full block (∆OFV = − 10) but was not included because of high uncertainty. Inclusion of non-linear elimination was not supported by the data. The residual error model was well described with a proportional model. IOV was statistically significant for Vc, but not included in the model because of high uncertainty. The SCM covariate search resulted in one statistically significant covariate, a study effect on F (∆OFV = − 11.5). The effect indicated that the DalcA trial performed in South Africa (phase 2b) [5] had 35% lower F compared to the trial in South Korea (phase 1/2) [4]. However, as a result of the small sample size, elevated uncertainty and that the covariate effect had no impact on the model’s descriptive performance of the data, the trial effect on F was not included in the final model. The final model described both IV and SC data well (Fig. 1). All final parameters are reported in Table 1 with model code in the Supplementary Material.

Prediction corrected visual predictive check (pcVPC) for all IV and SC data up to 120 h after DalcA administration. The solid and dashed lines are the median and 2.5th and 97.5th percentiles of the observed data, respectively. The shaded areas (top to bottom) are the 95% confidence intervals of the 97.5th (light grey), median (dark grey) and 2.5th (light grey) percentiles of the simulated data. Open circles are prediction-corrected observation points
Dose Regimen Exploration in Adults
The clinical trial simulations of different doses given OD or EOD showed that a large majority of adults would reach Cmin,ss at or above the target at steady state with a dose of 100 IU/kg given OD (Fig. 2). The two studied regimens of 125 and 150 IU/kg given EOD were not sufficient for achieving target trough levels (Fig. 2) in a majority of the simulated subjects and therefore not studied further. In addition, the time-to-target was derived across all simulated subjects for each regimen that was given OD. The median and 90% PI were derived and it was shown that for 50, 75, 90 and 100 IU/kg, the time-to-target was 6.3 (2.1–13.4), 4.4 (5.0–9.5), 3.6 (2.0–8.3) and 3.2 (1.6–7.1) days, respectively.

Percentage of population above target at different time points (pre-treatment, 4, 8, 12, 16 and 20 days on treatment) based on Cmin levels following different doses and dosing frequencies (OD, once daily and EOD, every other day). The yellow dashed line marks 80% of the population being above the target
Dose Regimen Exploration in the Paediatric Population
The paediatric PK simulations showed that a dose of 125 IU/kg given OD would result in the majority of the subjects down to 6 years being at or above the target at steady state (Fig. 3), and have trough levels similar to adults following 100 IU/kg given OD (Fig. 4). However, for subjects below 6 down to and including 2 years of age, a 150 IU/kg dose given OD was shown to be more appropriate (Figs. 3 and 4). The median and 90% PI of Cmin illustrate the distribution of Cmin values in comparison to adult levels and indicate a slightly lower prediction of Cmin in the 6-year-old group (Fig. 4). The median and 90% PI of time-to-target following OD dosing of 125 IU/kg were 2.7 (1.3–6.2), 3.1 (1.3–7.2), 3.2 (1.4–8.2) and 3.3 (1.5–7.3) days for the 11, 6, 4 and 2-year-old groups, respectively. The corresponding values for a daily 150 IU/kg dose were 2.2 (1.2–4.4), 2.3 (1.2–5.2), 2.4 (1.2–6.2) and 2.5 (1.3–7.2) days.

Percentage of population above target at different time points (pre-treatment, 4, 8, 12, 16 and 20 days on treatment) for different age groups based on Cmin levels following different doses given once daily (OD). The blue line is the corresponding result in adults following a 100 IU/kg dose given OD. The yellow dashed line marks 80% of the population being above the target

Mean (triangle) and 90% prediction interval of Cmin levels for different doses given once daily, at steady state for each age group. The blue horizontal line is the corresponding interval following once daily dosing of 100 IU/kg in adults. The vertical dashed line illustrates the target of 0.1 IU/mL
For the subjects in the 11- and 6-year-old groups that did not reach target at steady state following 125 IU/kg (n = 72, 154), a dose escalation to 175 IU/kg would bring 90% and 82% of them above target, respectively. For the paediatric subjects in the 4- and 2-year-old groups that did not reach target at steady state with 150 IU/kg given OD (n = 80, 133), a dose escalation to 200 IU/kg was shown to be sufficient to reach target at steady state in 88% and 84% of the subjects, respectively.
Discussion
This work sought to quantitatively characterize the PK of DalcA using population PK modelling and use the model for supporting dose selection [4, 5]. As a result of the rarity of the disease and small sample size of the trials, a population approach is suitable for informing first-in-paediatric dose selection. Data from two trials [4, 5] were pooled and a model with reasonable parameter precision (Table 1) and predictive performance (Fig. 1) was developed. The identified study effect could be explained by ethnicity, but was not identified for other FIX products in the literature and associated with uncertainty given the small sample size and therefore it was not included.
The clinical trial simulations in adults showed that a majority of patients in a large population of 1000 virtual subjects would achieve Cmin levels ≥ 0.1 IU/mL (10% FIX) with a dose of 100 IU/kg given OD (Fig. 2). This is in line with the conclusion of the previous actual trials, which in general suffered from small sample sizes. The model also enabled testing less frequent administration (EOD), which was shown to be insufficient (Fig. 2). However, the simulations assumed a target of 0.1 IU/mL and if a lower target based on clinical experience/criteria is set, EOD dosing might still be feasible. Another drawback of small sample sizes in prophylaxis trials for HB is the uncertainty associated with the time needed to reach target therapeutic levels, something that was studied with the model. For the 100 IU/kg dose level, 90% of virtual adult individuals had predicted time-to-target of 1.6–7.1 days. This is an important aspect as it determines a period in which subjects are still at risk of spontaneous bleeding events.
HB is a congenital disease affecting both adults and children with significant social and clinical impact lowering the quality of life for the patients. In particular for children, prophylaxis has at least in high-income countries been shown to introduce social benefits in comparison to on-demand treatment with potential to improve quality of life [19]. As such, developing models for novel prophylactic treatments including paediatric extrapolation of expected exposure levels in children is important. Dose selection for first-in-paediatric trials for coagulation factors have been shown to be reasonably well informed using allometric scaling with fixed exponents of 0.75 and 1 for clearance and volume terms, respectively [14]. Although associated with potential overprediction in the dose for younger children due to age-dependent organ maturation, in particular below 2 years of age, the method can provide a well-informed starting point in children [14, 19, 20]. With a larger sample size covering broad body weight range (not available in this study), the exponents of the allometric function can be estimated. The simulations showed that a 125 IU/kg dose given OD would result in FIX Cmin,ss values at or above the target in a majority of children down to 6 years of age, whereas below 6 and down to 2 years, 150 IU/kg appeared more suitable (Figs. 3 and 4). Using the same dose as appropriate for adults would not be sufficient in general, and is in accordance with other rFIX products [15]. The time-to-target was similar to adults (median level), but was shown to have a larger expected spread than adults in the simulated paediatric subjects. As the model was built on adult data and the paediatric simulations were based on extrapolation using allometry, the aspect of dose escalation in a situation of insufficient exposure at steady state was studied. For the few children predicted to be below target (n = 72, 154) in the 11 and 6-year-old groups, a dose escalation from 125 to 175 IU/kg would bring a majority above the target. For the younger children in the 4- and 2-year-old groups that did not reach target at steady state (n = 80, 133, respectively), with the predicted 150 IU/kg dose, a dose increase to 200 IU/kg would result in the majority of the children being above target. As adaptive trial designs are increasingly common, simulations like these can inform clinical investigators about potential dose escalations within a trial. Although the paediatric simulations are associated with uncertainty, model-based extrapolations are helpful for initial dose selection and can be confirmed or improved once actual data is available, in particular for children below 2 years of age.
To use FIX levels as a surrogate for clinical efficacy and subsequent regulatory approval, the PK/PD relationship between FIX levels and ABR need (per the existing guidelines) to be characterized in actual prospective clinical trials over 50 exposure days [8, 10] which was not the goal of this analysis as a result of limited PD data [5]. Furthermore, as PK data in children become available, the clinical trial simulations in children which currently are based on extrapolation through allometry can be revisited and confirmed or updated. Larger phase 3 trials need to be executed in an informed way to minimize bleeding risk for trial subjects as well as for de-risking the trial’s probability of success. Despite limited data and a small sample size, this modelling work supported the development of SC DalcA by providing a framework of the dose–concentration relationship for DalcA in adults and children, and by informing dosing selection.
Conclusion
Based on PK data from two clinical trials, a population PK model was successfully developed. Clinical trial simulations with the developed model indicated that 100 IU/kg given OD is a promising regimen for SC DalcA in adults. A dosing regimen of 125 IU/kg given OD is likely to meet the target in children down to 6 years of age, whereas 150 IU/kg given OD appears more appropriate for children below 6 down to 2 years of age.
References
Mannucci PM, Tuddenham EGD. The hemophilias—from royal genes to gene therapy. N Engl J Med. 2001;344:1773–9.
Srivastava A, Brewer AK, Mauser-Bunschoten EP, et al. Guidelines for the management of hemophilia. Haemophilia. 2013;19:e1–47.
Mannucci PM. Hemophilia therapy: the future has begun. Haematologica. 2020;105:545–53.
You CW, Hong S-B, Kim S, et al. Safety, pharmacokinetics, and pharmacodynamics of a next-generation subcutaneously administered coagulation factor IX variant, dalcinonacog alfa, in previously treated hemophilia B patients. J Thromb Haemost. 2021;19:967–75.
Mahlangu J, Levy H, Lee M, Del Greco F. Efficacy and safety of subcutaneous prophylaxis with dalcinonacog alfa in adults with haemophilia B. Haemophilia. 2021;27:574–80.
Blanchette VS, Key NS, Ljung LR, et al. Definitions in hemophilia: communication from the SSC of the ISTH. J Thromb Haemost. 2014;12:1935–9.
Zimmerman B, Valentino LA. Hemophilia: in review. Pediatr Rev. 2013;34:289–94 (quiz 295).
Center for Biologics Evaluation and Research. Human gene therapy for hemophilia. US Food and Drug Administration. 2002. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/human-gene-therapy-hemophilia. Accessed 21 June 2023.
Keipert C, Müller-Olling M, Gauly F, Arras-Reiter C, Hilger A. Annual bleeding rates: pitfalls of clinical trial outcomes in hemophilia patients. Clin Transl Sci. 2020;13:1127–36.
European Medicines Agency (2018) EMA Clinical investigation of recombinant and human plasma-derived factor IX products—Scientific guideline. https://www.ema.europa.eu/en/clinical-investigation-recombinant-human-plasma-derived-factor-ix-products-scientific-guideline.
Center for Drug Evaluation, Research Center for Biologics Evaluation and Research. Pediatric study plans: content of and process for submitting initial pediatric study plans and amended initial pediatric study plans. US Food and Drug Administration. 2020. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/pediatric-study-plans-content-and-process-submitting-initial-pediatric-study-plans-and-amended. Accessed 21 June 2023.
EMA. Paediatric investigation plans: questions and answers. European Medicines Agency. 2018. https://www.ema.europa.eu/en/human-regulatory/research-development/paediatric-medicines/paediatric-investigation-plans/paediatric-investigation-plans-questions-answers. Accessed 21 June 2023.
Anderson BJ, Holford NHG. Mechanism-based concepts of size and maturity in pharmacokinetics. Annu Rev Pharmacol Toxicol. 2008;48:303–32.
Mahmood I. Initiation of pediatric clinical trials for coagulation factors: application of pharmacokinetics and allometry to first-in-pediatric dose selection. J Clin Pharmacol. 2019;59:829–34.
FDA. and BeneFIX. US Food and Drug Administration. 20222. https://www.fda.gov/vaccines-blood-biologics/approved-blood-products/benefix. Accessed 21 June 2023.
Wählby U, Jonsson EN, Karlsson MO. Comparison of stepwise covariate model building strategies in population pharmacokinetic-pharmacodynamic analysis. AAPS J. 2002;4:68–79.
White GC 2nd, Rosendaal F, Aledort LM, et al. Definitions in hemophilia. Recommendation of the scientific subcommittee on factor VIII and factor IX of the scientific and standardization committee of the International Society on Thrombosis and Haemostasis. Thromb Haemost. 2001;85:560.
Introduction to hemophilia. Stage ELearning. https://elearning.wfh.org/elearning-centres/hemophilia/. Accessed 21 June 2023.
Giordano P, Lassandro G, Valente M, Molinari AC, Ieranò P, Coppola A. Current management of the hemophilic child: a demanding interlocutor. Quality of life and adequate cost-efficacy analysis. Pediatric Hematol Oncol. 2014;31:687–702.
Mahmood I. Prediction of clearance of monoclonal and polyclonal antibodies and non-antibody proteins in children: application of allometric scaling. Antibodies (Basel). 2020;9:40.
Acknowledgements
We thank the participants of the study, as well as the staff that executed the trials.
Funding
Open access funding provided by Uppsala University. USHS received funding from Catalyst Biosciences to do this work. The Rapid Service Fee was funded by Uppsala University.
Author Contributions
AF, USHS, TK, NLM, EG, and GEB performed the research. AF, USHS, TK, NLM, EG, and GEB designed the research study. AF, USHS, TK, NLM, EG, and GEB analyzed the data. AF, USHS, TK, NLM, EG, and GEB wrote the manuscript.
Prior Publication
Parts of this manuscript has been presented in a poster at the Population Approach Group in Europe (PAGE) conference (Ljubljana, Slovenia, 28 June–1 July, 2022).
Disclosures
Natacha Le Moan, Eduard Gorina, Grant E. Blouse and Tom Knudsen were employees and Natacha Le Moan and Tom Knudsen were shareholders of Catalyst Biosciences when this work was performed. Ulrika S.H. Simonsson received funding for this work. Alan Faraj have no conflict of interest to declare. Natacha Le Moan and Eduard Gorina changed affiliation prior to completion of the manuscript (Ashvattha Therapeutics, Inc and Freelance, respectively).
Compliance with Ethics Guidelines
The studies were conducted in accordance with the Declaration of Helsinki and US Code of Federal Regulations, International Conference on Harmonisation Guidelines on Good Clinical Practices, and South Korean national laws and regulations. Both study protocols were reviewed and approved by the institutional review board or independent ethics committee at each study site. All participants provided informed consent prior to enrollment.
Code Availability
The NONMEM code for the final model is provided in the supplementary material.
Data Availability
The dataset generated during and analyzed during the current study are available from the corresponding author upon reasonable request.
Author information
Authors and Affiliations
Corresponding author
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Faraj, A., Le Moan, N., Gorina, E. et al. Model-Informed Support of Dose Selection for Prophylactic Treatment with Dalcinonacog Alfa in Adult and Paediatric Hemophilia B Patients. Adv Ther 40, 3739–3750 (2023). https://doi.org/10.1007/s12325-023-02570-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-023-02570-6