
Abstract
Objectives
Assess baseline characteristics and treatment response to ixekizumab (IXE) categorised by sex in patients with radiographic axial spondyloarthritis (r-axSpA) and non-radiographic axSpA (nr-axSpA) up to 52 weeks.
Methods
Data were analysed from three randomised controlled trials of IXE through 52 weeks. Patients fulfilled ASAS classification criteria for r-axSpA or nr-axSpA and were randomised to receive 80 mg subcutaneous administration of IXE every 2 weeks (Q2W) or 4 weeks (Q4W), or placebo (16 weeks COAST-V/W; 52 weeks COAST-X). Baseline characteristics and treatment outcomes were assessed. Patients were categorised by sex; methods included non-responder imputation for categorical variables, and modified baseline observation carried forward for continuous efficacy variables.
Results
At presentation, female patients had higher disease burden as reflected by significantly higher spinal pain at night, fatigue scores and pain/swelling in joints other than the neck, back or hip. ASAS40 response rate with the approved label dose, IXEQ4W, was achieved in 39% of male patients with r-axSpA by week 16, and 44% by week 52. For female patients, 16.7% and 33.3% achieved ASAS40 at week 16 and 52, respectively. In nr-axSpA, 46% of male patients achieved ASAS40 at week 16 and 30% at week 52. In total, 23.9% of female patients achieved ASAS40 at week 16, and 30.4% at week 52.
Conclusions
This analysis demonstrates that for the axSpA disease spectrum, female patients present with higher disease burden. Following treatment with IXE, there is a higher proportion of male responders up to 16 weeks, while female patients show less robust responses for the first 16 weeks but larger responses from weeks 16 through 52.
Trial Registration Numbers
NCT02696785, NCT02696798 and NCT02757352.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
IXE has demonstrated superior efficacy to placebo in the treatment of patients with r-axSpA (COAST-V and COAST-W) and nr-axSpA (COAST-X). |
This analysis confirms previous observations that the clinical presentations and responses to therapy may differ in male and female patients. |
In this analysis, we demonstrate that for r-axSpA and nr-axSpA, female patients present with higher disease burden as reflected by higher scores in fatigue, spinal pain at night and pain/swelling in joints other than the neck, back or hip. |
What was learned from this study? |
Our findings indicate that for r-axSpA and nr-axSpA, male and female patients respond to therapy with IXE; however, female patients experience the maximum response later in their treatment course. |
Future studies looking into this topic may provide further insights to the current data. |
Introduction
Axial spondyloarthritis (axSpA) is a chronic inflammatory disease of the axial skeleton and sacroiliac joints and comprises two subtypes differentiated by the presence or absence of radiographic sacroiliitis, termed radiographic (r-axSpA, also referred to as ankylosing spondylitis [AS]) and non-radiographic (nr-axSpA).
A recent systematic review highlighted variability in assessment criteria that contributes to difficulty in determining the global incidence and prevalence rates of axSpA [1]. The incidence and prevalence of axSpA in the USA is estimated to be 1.4% [2]. Many studies in AS have included low numbers of female patients, and the analyses often do not account for the potential significance of sex differences in presentation and response to therapy [3]. Historically, AS was considered a male-predominant disease, with initial studies reporting male-to-female ratio of 10:1 [4]; however, this ratio has been revised and is now estimated to be 3:1 [5]. In patients with nr-axSpA, an equal male to female distribution has repeatedly been reported [6].
There are variations in clinical presentation between the sexes. Male patients with AS are more likely to develop radiographic spinal damage, which facilitates early diagnosis, whereas female patients develop more cervical spine and peripheral joint pain and have less frequent radiographic spinal damage [7]; however in patients with nr-axSpA, female patients show higher disease activity scores compared to male patients [8, 9]. A meta-analysis including 42 studies found that age of onset does not differ between male and female patients with spondyloarthritis (SpA) [10]; however, a mean delay in diagnosis showed sex-related differences, 8.8 years (7.4–10.1) for female patients and 6.5 (5.6–7.4) for male patients [10]. This may be in part the result of sex differences in the clinical presentation of patients, and suggests how female patients are frequently more likely to be underdiagnosed [3, 11]. Female patients with axSpA typically report higher Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) scores compared to male patients, specifically greater fatigue, total back pain and a longer duration of morning stiffness [12, 13]. Female patients also report worse quality of life and more activity impairment [14].
It has been shown for r-axSpA that male patients are more likely to be prescribed biological disease-modifying antirheumatic drugs (bDMARDs) compared to female patients who are more likely to be prescribed sulfasalazine, NSAIDs, muscle relaxants (not the standard of care), anticonvulsants, opioids and glucocorticoids [15]. Sex differences in clinical presentation may also affect a clinician’s perception of disease severity and activity, and thus influence disease management [16]. Cytokine signalling through the interleukin-17 (IL-17) pathway is a key contributor to the pathogenesis of axSpA, and IL-17A inhibitors are an efficacious alternative to tumour necrosis factor inhibitor (TNFi) for patients with axSpA [17, 18]. IL-17 signature studies have shown upregulated Il-17 gene expression in male patients compared to female patients [19]. Ixekizumab (IXE) is a high-affinity IL-17A monoclonal antibody and has demonstrated efficacy for patients with both r-axSpA and nr-axSpA [20, 21]. COAST-V was the first phase III clinical study assessing treatment with IXE in patients with r-axSpA and achieved ASAS40 as a primary endpoint [20]. This manuscript explores differences in male and female patients with r-axSpA and nr-axSpA who were included in three separate clinical trials of IXE. The first two trials included patients with r-axSpA who were either bDMARD-naïve (COAST-V) or TNFi-experienced (COAST-W). The third trial included patients with nr-axSpA who were bDMARD-naïve (COAST-X).
Methods
Study Design
COAST-V (NCT02696785), COAST-W (NCT02696798) and COAST-X (NCT02757352) were phase III, multicentre, randomised, double-blind, active-controlled (COAST-V only) and placebo (PBO)-controlled, 52-week trials, followed by an optional 2-year extension. Baseline clinical characteristics and treatment response of patients with r-axSpA were integrated from COAST-V and COAST-W and categorised by sex. Baseline clinical characteristics and treatment response of patients with nr-axSpA from COAST-X were analysed separately and categorised by sex.
The COAST-V, COAST-W and COAST-X trials were conducted in accordance with the standards of the Declaration of Helsinki and Good Clinical Practice Guidelines (CPMP/ICH/135/95). The master ethics committee was Schulman Associates IRB, Cincinnati, OH, USA. Full listings of investigators and sites are available in previously published manuscript supplements [20, 22]. All patients gave written informed consent before trial start.
Patients and Treatment Protocol
Patient eligibility criteria have been described previously [20, 21]. Patients in COAST-V/W were aged 18 years or older, with an established diagnosis of r-axSpA, and meeting Assessment of SpondyloArthritis International Society (ASAS) criteria (with central reading of radiographic sacroiliitis). Patients in COAST-W were required to have discontinued one or two TNFi because of intolerance or inadequate response; COAST-V only included bDMARD-naïve patients. In COAST-V, there was an additional active-reference arm in which patients were treated with 40 mg adalimumab every 2 weeks (Q2W). For COAST-X, eligible patients were aged 18 years or older, with a physician-established axSpA diagnosis, fulfilling ASAS criteria and had a treatment history for axSpA for at least 12 weeks. Patients meeting the radiologic criterion of the modified New York criteria (according to central reading by two readers and an adjudicator in case of a discrepancy) were excluded. Patients were randomised to receive 80 mg subcutaneous administration of IXE Q2W, every 4 weeks (Q4W) or PBO. COAST-X was a 52-week, double-blind, PBO-controlled trial; however, patients could switch to open-label IXEQ2W after week 16 and at the discretion of the primary investigator [21]; patients who switched to open-label treatment were analysed as non-responders.
Assessments
In this post hoc analysis, patients were categorised by sex. The primary objective was to compare the efficacy of IXE (all dosing regimens) versus PBO at weeks 16 and 52 (COAST-X), and the response up to week 52 in COAST-V and COAST-W, as measured by the proportion of patients achieving an ASAS40 response. The major secondary objectives were to compare IXE (all dosing regimens) versus PBO at weeks 16 and 52 (COAST-X) as measured by the proportion of patients achieving at least 50% improvement in the BASDAI score from baseline, and Ankylosing Spondylitis Disease Activity Score (ASDAS) inactive disease (defined as ASDAS < 1.3), as well as the change from baseline in ASDAS Low Disease Activity (LDA) (defined as ASDAS LDA < 2.1), Bath Ankylosing Spondylitis Functional Index (BASFI), magnetic resonance imaging of the spine SPARCC score, Medical Outcomes Study 36-Item Short Form Health Survey (SF-36) physical component summary, and the ASAS Health Index. Full inclusion/exclusion criteria, treatment protocols, safety outcomes and adverse events have been published for the three trials previously.
Statistical Analysis
Descriptive baseline clinical characteristics were categorised by sex to demonstrate the difference between male and female patients. In COAST-X, patients who switched to open label after week 16 were analysed as non-responders. To examine the statistical significance of the difference in baseline, Fisher’s exact test or CMH test was conducted for categorical data, and analysis of covariance (ANCOVA) or analysis of variance (ANOVA) was conducted for continuous data.
Differences in response between IXE treatment groups versus PBO were assessed at week 16 (and at week 52 for COAST-X) for post-baseline efficacy assessments. Categorical assessments used the CMH test stratified by study for each sex subgroup for the integrated study (COAST-V and COAST-W), and Fisher’s exact test for COAST-X. Continuous assessments used the LSM change from baseline and p value vs PBO from ANCOVA models with covariates specific to the respective studies. Missing values were imputed using last observation carried forward.
Results
Baseline Characteristics by Sex
There were statistically significant differences between male and female patients at age of disease onset, with female patients of older age, for patients with r-axSpA (mean ± SD; female patients: 30.1 ± 10.1 years, male patients: 26.5 ± 8.7 years, p = 0.002) and nr-axSpA (female patients: 32 ± 10.7 years, male patients: 27.9 ± 7.7 years, p = 0.002). Female patients also had longer symptom duration (r-axSpA: 17.8 ± 12.2 years vs 16.7 ± 10.5 years; nr-axSpA: 12.3 ± 11.3 years vs 9.5 ± 9.2 years) than male patients. High disease activity, as measured by mean total BASDAI score, was reported for both female patients (r-axSpA: 7.4 ± 1.5; nr-axSpA: 7.4 ± 1.4) and male patients (r-axSpA: 7.1 ± 1.4; nr-axSpA: 6.9 ± 1.4). This difference was statistically significant in patients with nr-axSpA (p = 0.013). Female patients with nr-axSpA scored higher than male patients on all six BASDAI questions, and female patients with r-axSpA scored higher on five of the six BASDAI questions (Table 1). Female patients also reported higher scores on spinal pain at night than male patients (r-axSpA: 7.8 ± 1.7 vs 7.4 ± 1.5; nr-axSpA: 7.6 ± 1.8 vs 7.0 ± 1.8); this was significant for both r-axSpA and nr-axSpA (COAST-V/W: p = 0.033; COAST-X: p = 0.027). C-reactive protein levels were significantly higher in male patients versus female patients in patients with r-axSpA (female patients: 11.2 ± 12.8 vs male patients: 17.4 ± 25.5, p = 0.030) but similar in patients with nr-axSpA (female patients: 12.3 ± 18.5 vs male patients: 12.1 ± 17.4, p = 0.931).
A higher proportion of male patients than female patients had a history of anterior uveitis for r-axSpA (23.8% vs 17.9%), and conversely, more female patients than male patients had a history of anterior uveitis for nr-axSpA (15.2% vs 7.1%).
The proportion of patients who were human leukocyte antigen B27 positive was higher for male patients compared with female patients for r-axSpA (86.9% vs 79.5%) and nr-axSpA (76.3% vs 70.7%), but the differences were not significant.
Treatment Response by Sex
ASAS40
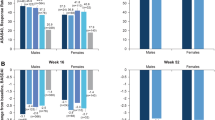
For IXEQ4W (approved label dose) male patients with r-axSpA, 39% (n = 62/159) achieved ASAS40 at week 16; this was sustained at week 52 (44%). Male patients with nr-axSpA achieved an ASAS40 response of 46% at week 16, which was significant over PBO (IXEQ4W: n = 23/50, 46%; PBO: n = 8/44, 18.2%, p = 0.005); at week 52, male ASAS40 response was 30%. Female patients with r-axSpA achieved an ASAS40 response of 16.7% (n = 6/36) at week 16, which was statistically different from PBO (p = 0.041); this response rose to 33.3% at week 52. Female patients with nr-axSpA achieved an ASAS40 response of 23.9% at week 16, which was not significant over PBO (IXEQ4W: n = 11/46, 23.9%; PBO: 12/61, 19.7%, p = 0.640); however, female patients showed a significant response compared to PBO at week 52 (IXEQ4W: n = 14/46, 30.4%; PBO: 5/61, 8.2%, p = 0.004) (Fig. 1).

COAST-V/W and COAST-X ASAS40 (ITT, NRI). Patients initially randomised to PBO in COAST-V/W switched to IXEQ2W or Q4W at week 16 by study design; PBO data are summarised up to week 16. Data displayed as mean. Significantly greater response rate versus PBO following IXE treatment denoted by * (p ≤ 0.05), ** (p ≤ 0.01), *** (p ≤ 0.001). ASAS40 Assessment in SpondyloArthritis International Society 40%, Q4W every 4 weeks, Q2W every 2 weeks, ITT intent-to-treat population, NRI non-responder imputation, PBO placebo, IXE ixekizumab
ASDAS-LDA (< 2.1)
For IXEQ4W (approved label dose), the proportion of male patients with r-axSpA who achieved ASDAS-LDA (< 2.1) response was significantly greater compared to PBO at week 16 (male patients: n = 49/159, 30.8%; PBO: n = 15/159, 9.4%, p < 0.001). This response was not significant for PBO in female patients (IXEQ4W: n = 6/36, 16.7%; PBO: n = 1/32, 3.1%, p = 0.110). A higher response rate was observed for male patients with nr-axSpA versus PBO at week 16 (IXEQ4W: n = 19/49, 38.8%; PBO: n = 5/44, 11.4%, p = 0.004), which was sustained at week 52 (IXEQ4W: 16/49, 32.7%; PBO: 4/44, 9.1%, p = 0.010). There was no significant response compared to PBO for female patients with nr-axSpA at week 16 (IXEQ4W: n = 7/45, 15.6%; PBO: 8/61, 13.1%, p = 0.782), but by week 52 there was a significant response versus PBO (IXEQ4W: n = 12/45, 26.7%; PBO: n = 5/61, 8.2%, p = 0.015) (Fig. 2).

ASDAS LDA < 2.1 response rate (%) across three treatment groups. Data displayed as mean. Significantly greater response rate versus PBO following IXE treatment denoted by * (p ≤ 0.05), ** (p ≤ 0.01), *** (p ≤ 0.001). ASDAS Ankylosing Spondylitis Disease Activity Score, LDA low disease activity, Q4W every 4 weeks, Q2W every 2 weeks, ITT intent-to-treat population, NRI non-responder imputation, PBO placebo, IXE ixekizumab
BASDAI
The overall BASDAI response rate in patients with r-axSpA saw a greater change from baseline response in male patients versus PBO at week 16 ([LSM ± SE] IXEQ4W male patients [n = 159/195]: − 2.65 ± 0.16; PBO: − 1.35 ± 0.16, p < 0.001) than female patients (IXEQ4W female patients [n = 36/195]: − 1.86 ± 0.34; PBO: − 0.66 ± 0.36, p = 0.015) (Table 2). For BASDAI Q6 (duration of morning stiffness), female patients displayed greater change from baseline response (IXEQ4W: − 2.17 ± 0.4; PBO: − 0.90 ± 0.43, p = 0.030). Significant responses were also seen in male patients compared to PBO at week 16 in spinal pain at night (IXEQ4W: − 3.24 ± 0.19; PBO: − 1.50 ± 0.19, p < 0.001), BASFI (IXEQ4W: − 2.21 ± 0.16; PBO: − 1.08 ± 0.16, p < 0.001) and SF-36 Physical Component Score (IXEQ4W: 7.15 ± 0.55; PBO: 3.06 ± 0.55, p < 0.001). Significant responses varied in these measures when observed in female patients at week 16 (Table 2).
In patients with nr-axSpA, male patients showed a greater change from baseline compared to PBO at week 16 for BASDAI Q2 (spinal pain) (male patients: − 2.99 ± 0.33; PBO: − 1.61 ± 0.37, p = 0.006), Q6 (duration of morning stiffness) (male patients: − 2.98 ± 0.37; PBO: − 1.34 ± 0.41, p = 0.003) and BASFI (male patients: − 2.40 ± 0.32; PBO: − 1.35 ± 0.35, p = 0.028). These changes were sustained at week 52 for Q6 (duration of morning stiffness) (male patients: − 3.05 ± − 0.38; PBO: − 1.58 ± 0.43, p = 0.010) and BASFI (male patients: − 2.64 ± 0.35; PBO: − 1.50 ± 0.39, p = 0.029) with the addition of a significant change in BASDAI Q5 (morning stiffness) (male patients: − 3.09 ± − 0.37; PBO: − 1.89 ± 0.41, p = 0.030). No significant changes from baseline were seen for female patients with nr-axSpA at week 16. At week 52, female patients showed a greater improvement versus PBO in four out of six BASDAI questions, BASDAI Q1 (fatigue/tiredness) (female patients: − 2.33 ± 0.36; PBO: − 1.36 ± 0.32, p = 0.044), Q2 (spinal pain) (female patients: − 2.26 ± 0.36; PBO: − 1.18 ± 0.32, p = 0.026), Q3 (pain/swelling in other joints) (female patients: − 2.19 ± 0.39; PBO: − 0.65 ± 0.34, p = 0.003) and Q5 (morning stiffness) (female patients: − 2.66 ± 0.39; PBO: − 1.37 ± 0.34, p = 0.013) (Table 3).
For treatment responses in IXEQ2W patients with r-axSpA and nr-axSpA, refer to Supplementary Tables 1 and 2.
Discussion
Baseline Characteristics by Sex
Several studies considering sex (gender) differences have revealed that female patients with axSpA have a longer diagnostic delay compared to male patients [3, 6, 23], with the disease severity presenting differently between the two sexes. The reasons for these differences are not clear, but factors such as differences in immune, hormonal and genetic responses may play a role [3]. The results of this analysis suggest potentially important clinical differences between male and female patients with r-axSpA and nr-axSpA. Female patients with r-axSpA and nr-axSpA experienced longer duration of symptoms since axSpA onset than male patients, in line with previous studies [23, 24], supporting observations that sex differences in clinical presentation of patients with axSpA can lead to delayed diagnosis in female patients [3, 11] and highlighting the need for more awareness of potential clinical differences in presentation between male and female patients.
Higher BASDAI scores at baseline in female patients compared with male patients have been found in other studies [9, 25]. In this analysis, female patients with r-axSpA scored numerically higher than male patients on five of the six symptoms assessed by BASDAI at baseline (fatigue/tiredness, spinal pain, pain/swelling in other joints, discomfort/tenderness to touch/pressure and morning stiffness). This trend was also visible in female patients with nr-axSpA, with added statistical significance, suggesting a somewhat higher disease burden in female patients within the axSpA spectrums in line with previous studies [3].
In this analysis, C-reactive protein levels were significantly higher in male patients compared to female patients with r-axSpA but similar in patients with nr-axSpA.
Treatment Response by Sex
This post hoc analysis suggests that male patients achieve a peak response earlier than female patients, but with continuation of treatment, female patients continue to improve over time.
Research evaluating sex differences in pain largely focuses on understanding biological and psychosocial variables in pain [26, 27]. Biological explanations range from identified differences in gonadal hormones to neurochemistry, with psychological explanations ranging from typical gender roles to varying coping mechanisms between the sexes [28]. Sex-influenced access to healthcare, and associated diagnosis, assessment and management have also been considered [29].
Current research suggests that disease activity (BASDAI) scores are significantly higher in women and that they have significantly lower response rates to treatment with TNFi [3, 12]. Data on sex differences in other biologics, such as IL-17 inhibitors, are limited [23]. As stated previously, a higher burden of disease was evident in this study for female patients at baseline with female patients having significantly higher pain and fatigue scores. Male patients with r-axSpA showed greater response rates versus PBO across most of the treatment parameters measured. Female patients with r-axSpA and nr-axSpA displayed delayed attainment of peak responses to treatment with the approved label dose, with a higher percentage of male patients achieving ASAS40 and ASDAS < 2.1 at week 16 than female patients, despite similar retention rates.
A 2013 study by van der Horst-Bruinsma et al. [25] examining the impact of gender on clinical, functional and patient-reported treatment outcomes using data pooled from four AS clinical trials demonstrated similar early stage (week 12) findings to this analysis where, although both gender groups showed improvements, female patients showed significantly smaller changes. The higher age at disease onset seen in female patients in both r-axSpA and nr-axSpA in this analysis may have contributed to the higher disease burden observed at baseline. van der Horst-Bruinsma et al. [25] further suggested that this higher burden at baseline may lead to more resistant disease and a reduced response to treatment compared to male patients, particularly earlier on in treatment, as seen in this analysis. The differences in the proportion of the responses cannot be explained from this post hoc analysis. While a recent study revealed increased Th17 repertoire and elevated IL-17 levels in male patients compared to female patients [19], our study revealed that female patients showed a significant response to IXE although the response was initially delayed. This analysis, in line with previous studies [25], highlights a greater disease severity and lessened treatment response in female patients. Future studies looking into this topic may provide further insights to the current data.
A limitation of this study was the lack of pre-specified criteria in COAST-X to allow patients to switch to open label at week 16 and be analysed as non-responders, which may have resulted in the ASAS40 response rate drop seen in male patients with nr-axSpA. Additionally, the disproportion in the number of male and female patients in the r-axSpA trials limits the validity when comparing responses between the two sexes.
Conclusion
This analysis demonstrates that, in general, female patients had higher disease burden than male patients for the axSpA disease spectrum. Our findings indicate that, while female patients show lower ASAS40 response rates than male patients at week 16, IXE is efficacious in treating male and female patients with AS and nr-axSpA. Nonetheless, female patients tend to experience achievement of response later in their treatment course.
References
Akkoc N, Khan MA. Is axial spondyloarthritis more common than rheumatoid arthritis? Curr Rheumatol Rep. 2020;22(9):54.
Reveille JD, Witter JP, Weisman MH. Prevalence of axial spondylarthritis in the United States: estimates from a cross-sectional survey. Arthritis Care Res (Hoboken). 2012;64(6):905–10.
Rusman T, van Vollenhoven RF, van der Horst-Bruinsma IE. Gender differences in axial spondyloarthritis: women are not so lucky. Curr Rheumatol Rep. 2018;20(6):35.
West HF. Aetiology of ankylosing spondylitis. Ann Rheum Dis. 1949;8:143–8.
Kennedy LG, Will R, Calin A. Sex ratio in the spondyloarthropathies and its relationship to phenotypic expression, mode of inheritance and age at onset. J Rheumatol. 1993;20(11):1900–4.
Neuenschwander R, Hebeisen M, Micheroli R, et al. Differences between men and women with nonradiographic axial spondyloarthritis: clinical characteristics and treatment effectiveness in a real-life prospective cohort. Arthritis Res Ther. 2020;22(1):233.
Lee W, Reveille JD, Weisman MH. Women with ankylosing spondylitis: a review. Arthritis Rheum. 2008;59(3):449–54.
Tournadre A, Pereira B, Lhoste A, et al. Differences between women and men with recent-onset axial spondyloarthritis: results from a prospective multicenter French cohort. Arthritis Care Res (Hoboken). 2013;65(9):1482–9.
de Carvalho HM, Bortoluzzo AB, Gonçalves CR, et al. Gender characterization in a large series of Brazilian patients with spondyloarthritis. Clin Rheumatol. 2012;31(4):687–95.
Jovaní V, Blasco-Blasco M, Ruiz-Cantero MT, Pascual E. Understanding how the diagnostic delay of spondyloarthritis differs between women and men: a systematic review and metaanalysis. J Rheumatol. 2017;44(2):174–83.
Horst-Bruinsma IVD, Hunter T, Bolce R, Holdsworth E, Booth N. SAT0332 gender differences in disease status, quality of life and treatment patterns among axial spondyloarthritis patients: findings from a global survey. Ann Rheum Dis. 2019;78(Suppl 2):1245–1245.
Webers C, Essers I, Ramiro S, et al. Gender-attributable differences in outcome of ankylosing spondylitis: long-term results from the Outcome in Ankylosing Spondylitis International Study. Rheumatology (Oxford). 2016;55(3):419–28.
Swinnen TW, Westhovens R, Dankaerts W, de Vlam K. Widespread pain in axial spondyloarthritis: clinical importance and gender differences. Arthritis Res Ther. 2018;20(1):156.
Ibn Yacoub Y, Amine B, Laatiris A, Hajjaj-Hassouni N. Gender and disease features in Moroccan patients with ankylosing spondylitis. Clin Rheumatol. 2012;31(2):293–7.
Walsh J, Hunter T, Schroeder K, Sandoval D, Bolce R. Trends in diagnostic prevalence and treatment patterns of male and female ankylosing spondylitis patients in the United States, 2006–2016. BMC Rheumatol. 2019;3:39.
Barnabe C, Bessette L, Flanagan C, et al. Sex differences in pain scores and localization in inflammatory arthritis: a systematic review and metaanalysis. J Rheumatol. 2012;39(6):1221–30.
San Koo B, Kim TH. The role of ixekizumab in non-radiographic axial spondyloarthritis. Ther Adv Musculoskelet Dis. 2021;13:1759720x20986734.
McGonagle DG, McInnes IB, Kirkham BW, Sherlock J, Moots R. The role of IL-17A in axial spondyloarthritis and psoriatic arthritis: recent advances and controversies. Ann Rheum Dis. 2019;78(9):1167–78.
Gracey E, Yao Y, Green B, et al. Sexual dimorphism in the Th17 signature of ankylosing spondylitis. Arthritis Rheumatol. 2016;68(3):679–89.
van der Heijde D, Cheng-Chung Wei J, Dougados M, et al. Ixekizumab, an interleukin-17A antagonist in the treatment of ankylosing spondylitis or radiographic axial spondyloarthritis in patients previously untreated with biological disease-modifying anti-rheumatic drugs (COAST-V): 16 week results of a phase 3 randomised, double-blind, active-controlled and placebo-controlled trial. Lancet. 2018;392(10163):2441–51.
Deodhar A, van der Heijde D, Gensler LS, et al. Ixekizumab for patients with non-radiographic axial spondyloarthritis (COAST-X): a randomised, placebo-controlled trial. Lancet. 2020;395(10217):53–64.
Deodhar A, Poddubnyy D, Pacheco-Tena C, et al. Efficacy and safety of ixekizumab in the treatment of radiographic axial spondyloarthritis: sixteen-week results from a phase III randomized, double-blind, placebo-controlled trial in patients with prior inadequate response to or intolerance of tumor necrosis factor inhibitors. Arthritis Rheumatol. 2019;71(4):599–611.
Rusman T, van Bentum RE, van der Horst-Bruinsma IE. Sex and gender differences in axial spondyloarthritis: myths and truths. Rheumatology (Oxford). 2020;59(Suppl4):iv38–46.
Wright GC, Kaine J, Deodhar A. Understanding differences between men and women with axial spondyloarthritis. Semin Arthritis Rheum. 2020;50(4):687–94.
van der Horst-Bruinsma IE, Zack DJ, Szumski A, Koenig AS. Female patients with ankylosing spondylitis: analysis of the impact of gender across treatment studies. Ann Rheum Dis. 2013;72(7):1221–4.
Fillingim RB, King CD, Ribeiro-Dasilva MC, Rahim-Williams B, Riley JL 3rd. Sex, gender, and pain: a review of recent clinical and experimental findings. J Pain. 2009;10(5):447–85.
Mogil JS, Bailey AL. Sex and gender differences in pain and analgesia. Prog Brain Res. 2010;186:141–57.
Mogil JS. Sex differences in pain and pain inhibition: multiple explanations of a controversial phenomenon. Nat Rev Neurosci. 2012;13(12):859–66.
Leresche L. Defining gender disparities in pain management. Clin Orthop Relat Res. 2011;469(7):1871–7.
Acknowledgements
Authors who are employees of the study sponsor, Eli Lilly and Company (Indianapolis, IN, USA), were involved in the study design, collecting and analysing the data, interpreting the results and preparing the abstract. Writing support was provided by Geraldine Fahy and Natalie Haustrup, employees of Eli Lilly and Company; editorial support, and quality review was provided by Sukanya Chaudhury, and Jyoshna M, respectively, employees of Eli Lilly and Company.
Funding
Eli Lilly and Company funded the study, the Rapid Service Fee and the Open Access Fee.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author Contributions
DS and RB conceived the presented idea; DZ and VG carried out analysis of the data for the work; all authors interpreted the data for the work and critically revised the work. All authors discussed the results and contributed to the final manuscript.
Disclosures
Prof Dr van der Horst-Bruinsma affiliation during the trial was the Department of Rheumatology, Amsterdam UMC, VU University Medical Centre, Amsterdam, the Netherlands. Prof Dr van der Horst-Bruinsma has received grant/research support and consultancy fees from: AbbVie, Merck Sharp & Dohme, Novartis, Pfizer, and UCB Pharma; and is on the speakers bureau for: AbbVie, Bristol Myers Squibb, Merck Sharp & Dohme, and Pfizer; Prof. de Vlam has received grant/research support and consultancy fees from: AbbVie, Janssen, Sandoz, Amgen, Merck Sharp & Dohme, Novartis, Pfizer, Galapagos, Eli Lilly and UCB Pharma; and is on the speakers bureau for: Amgen, Eli Lilly, AbbVie, UCB, Merck Sharp & Dohme, and Pfizer; Dr Walsh has received consulting fees from AbbVie, Novartis, Lilly, Amgen, UCB, Pfizer, Janssen. Grants from Pfizer, Merck, AbbVie; Dr Bolce, Dr Hunter, Dr Sandoval, Dr Zhu and Dr Geneus are employees of Eli Lilly and Company; Dr Soriano has received grant/research support from AbbVie, Janssen, Novartis, Pfizer, Roche, and UCB Pharma, and honoraria for consulting from AbbVie, Amgen, BMS, Janssen, Eli Lilly and Company, Novartis, Pfizer, Roche, Sandoz, and UCB Pharma; Dr Magrey has received grant/research support and consultancy fees from: AbbVie, Eli Lilly and Company, Janssen, Novartis, and UCB Pharma, and honoraria from Eli Lilly and Company.
Compliance with Ethics Guidelines
COAST-V, W and X (Clinicaltrials.gov: NCT02696785, NCT02696798 and NCT02757352) were conducted in accordance with the ethical principles of the Declaration of Helsinki and Good Clinical Practice Guidelines (CPMP/ICH/135/95). The master ethics committee was Schulman Associates IRB, Cincinnati, OH, USA. Full listings of investigators and sites are available in previously published manuscript supplements [20, 22]. All patients gave written informed consent before trial start.
Data Availability
Lilly provides access to all individual participant data collected during the trial, after anonymization, with the exception of pharmacokinetic or genetic data. Data are available to request 6 months after the indication studied has been approved in the USA and EU and after primary publication acceptance, whichever is later. No expiration date of data requests is currently set once data are made available. Access is provided after a proposal has been approved by an independent review committee identified for this purpose and after receipt of a signed data sharing agreement. Data and documents, including the study protocol, statistical analysis plan, clinical study report, blank or annotated case report forms, will be provided in a secure data sharing environment. For details on submitting a request, see the instructions provided at www.vivli.org.
Author information
Authors and Affiliations
Corresponding author
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
van der Horst-Bruinsma, I.E., de Vlam, K., Walsh, J.A. et al. Baseline Characteristics and Treatment Response to Ixekizumab Categorised by Sex in Radiographic and Non-radiographic Axial Spondylarthritis Through 52 Weeks: Data from Three Phase III Randomised Controlled Trials. Adv Ther 39, 2806–2819 (2022). https://doi.org/10.1007/s12325-022-02132-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-022-02132-2