
Abstract
Introduction
The current non-invasive tools for the diagnosis of non-alcoholic fatty liver disease (NAFLD) have methodological limitations. We aimed to develop a non-invasive scale to assist in the diagnosis of NAFLD. To achieve our aim, we conducted a secondary analysis of data from a large observational study conducted in Russia.
Methods
This retrospective analysis assessed the frequency of NAFLD in the population of patients in the DIREG_L_06725 study, an epidemiological, observational, cross-sectional, multicenter study performed in 50,145 outpatients from 16 Russian cities. Among the cohort of patients diagnosed with NAFLD, we identified factors associated with the risk of NAFLD. To develop a non-invasive tool for diagnosing NAFLD, we also determined the frequency of steatohepatitis.
Results
Our analysis included 48,297 patients; NAFLD was present in 20,281 patients (42.0%). The majority (64.1%) were women (80.3% post-menopause), and 87% had a body mass index (BMI) > 27.0 kg/m2. We developed a fully non-invasive scale (St-index) that showed a specificity of 91.4% for ruling in steatosis, and a sensitivity of 93.8% for ruling out steatosis. Multivariate regression analyses conducted in the subgroups of patients aged ≥ 12 and < 18 years and those with BMI < 25.0 kg/m2 produced area under the receiver operating characteristic (AUROC) curve values of 0.8243 and 0.7054, respectively. The factors most strongly associated with the development of NAFLD were age > 35 years, presence of type 2 diabetes mellitus, and a waist circumference/height ratio > 0.54.
Conclusion
Our non-invasive steatosis scale, St-index, can help physicians diagnose NAFLD in high-risk patients in the absence of ultrasound data.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
Non-alcoholic fatty liver disease (NAFLD) may be underdiagnosed because screening relies on diagnostic imaging, which may not be widely available in many countries, and on unreliable indices, such as the hepatic steatosis index. |
This retrospective analysis of an observational study in Russian patients with suspected NAFLD aimed to develop a non-invasive diagnostic test for NAFLD. |
What was learned from the study? |
The prevalence of NAFLD was 42.0%, and risk factors for NAFLD were patient age > 35 years, presence of type 2 diabetes mellitus, and a waist circumference/height ratio of > 0.54. |
The non-invasive steatosis scale (St-index) accurately identified steatosis 91.4% of the time and accurately ruled out steatosis 93.8% of the time. |
The St-index may be a useful non-invasive tool to help diagnose NAFLD in high-risk patients, particularly in the absence of ultrasound data. |
Digital Features
This article is published with digital features to facilitate understanding of the article. To view digital features for this article go to https://doi.org/10.6084/m9.figshare.12902387.
Introduction
Non-alcoholic fatty liver disease (NAFLD) is rapidly becoming the most common cause of liver disease worldwide [1, 2], with an estimated prevalence of 10–30% in Western countries [3, 4]. A higher prevalence of NAFLD is reported in patients with metabolic syndrome, with up to 40–70% of patients with NAFLD having type 2 diabetes mellitus (T2DM) [3, 5], and as many as 90% having morbid obesity [3].
NAFLD is classified into simple steatosis (”pure steatosis”) and non-alcoholic steatohepatitis (NASH; comprising approx. 20% of NAFLD) [6]. NASH can trigger liver fibrogenesis, which can further progress to cirrhosis and hepatocellular carcinoma [2, 6]. NAFLD is also an independent risk factor for fatal cardiovascular events [2], and even simple steatosis, which can be diagnosed with ultrasound, has been associated with a three-fold increase in cardiovascular mortality rate compared with patients without NAFLD [7].
While liver biopsy is the gold standard for liver diagnostics, it is invasive and impractical for screening large populations [8, 9]. Magnetic resonance imaging (MRI)-based methods are expensive and not widely available; computed tomography and ultrasound have intrinsic subjective and technical limitations [9, 10]; and the fatty liver index (FLI) [11], hepatic steatosis index (HSI) [12], and NAFLD liver fat score (NAFLD-LFS) [13] lack sufficient validation or cannot quantify steatosis accurately [10, 13, 14]. Waist circumference (WC) measurement has been found to be as reliable as FLI [15, 16], and waist circumference/height ratio (WCHR) is reportedly more reliable than WC, although the latter conclusion is questionable [17, 18]. So far, ultrasound remains the most accessible and frequently used screening diagnostic test [9], but insurance limitations in Russia reduce its availability [3]. The limitations of the available screening tests, combined with the often silent nature of NAFLD, may explain the substantial gap in the diagnosis of NAFLD.
The aim of the present study was to develop a new, fully non-invasive screening test for NAFLD, focusing on steatosis, by conducting a secondary analysis of data from the large-scale, observational DIREG_L_06725 study conducted in Russian patients with NAFLD [19]. We also determined the frequency of NAFLD in eligible patients from the DIREG_L_06725 study cohort and in subgroups of interest, identified the most prominent baseline characteristics of patients with NAFLD, as well as the factors associated with the risk of developing NAFLD, the relationship between NAFLD and other comorbidities, and the accuracy of the available non-invasive diagnostic tests for NAFLD.
Methods
Ethics Statements
The present secondary analysis of the DIREG_L_06725 study was conducted in compliance with the Ethical Principles for Medical Research Involving Human Subjects outlined in the Helsinki Declaration of 1975 (revised in 2000). This was a secondary analysis and authors had no access to patients’ confidential information (names); therefore, no informed consent or ethical approval was required.
Study Design
This report presents the results of a secondary analysis of data from the DIREG_L_06725 study. DIREG_L_06725 was an epidemiological, observational, cross-sectional, multicenter study performed to determine the prevalence of NAFLD in 50,145 outpatients from 16 Russian cities [19].
Patients
The DIREG_L_06725 cohort consisted of outpatients aged ≥ 12 and ≤ 80 years, who had presented for initial or repeated consultations with selected physicians in polyclinics, regardless of the cause of the visit, including those with suspected NAFLD. NAFLD was suspected on the basis of the presence of obesity, T2DM, dyslipidemia, metabolic syndrome, hypertension, and/or abnormal cholesterol levels (based on physician/endocrinologist diagnosis and laboratory abnormalities in primary medical records).
The exclusion criteria for DIREG_L_06725 were inability to participate in the study for any reason, pregnancy, secondary causes of liver disease (verified diagnosis of alcoholic liver disease or average daily alcohol consumption ≥ 40 g in men or ≥ 20 g in women; current or previous viral hepatitis; autoimmune hepatitis; toxic liver damage; or hereditary liver diseases) and confirmed absence of hepatic pathologies. We excluded fibrotic or cirrhotic patients from the NAFLD group if they did not have steatosis, because the data did not allow us to distinguish NAFLD-related fibrosis or cirrhosis from cirrhosis caused by other factors.
We excluded from the present analysis patients with missing or conflicting data on the variables of interest, and patients with outlier values for the variables of interest (for each analysis separately).
Study Objectives
We aimed to examine and compare the accuracy of non-invasive diagnostic tests taking ultrasound-based diagnosis as a reference, and to develop a fully non-invasive screening test to diagnose or at least suspect NAFLD (steatosis). We also aimed to estimate the frequency of NAFLD (hepatic steatosis confirmed by ultrasound analysis) in a cohort of patients diagnosed with NAFLD in the DIREG_L_06725 study based on demographic, anthropometric, clinical, and laboratory variables. Furthermore, we aimed to identify the risk factors for NAFLD.
We performed analyses to estimate the frequency of NAFLD by sex, age (≥ 12 and < 18, ≥ 18 and < 35, ≥ 35 and < 60, ≥ 60 and ≤ 80 years), body mass index (BMI; < 25, ≥ 25 and < 30, ≥ 30 kg/m2), WCHR, and the degree of NAFLD (pure steatosis vs. NASH). We also analyzed the distribution of NASH, defined as patients with NAFLD having alanine aminotransferase (ALT)/alanine transaminase (AST) and/or gamma-glutamyl transferase (GGT) levels > 1.5 times the upper limit of normal based on the results of two consecutive laboratory tests with an interval of 1 month. This criterion was chosen on the basis of data from a study by Losekann et al. [20].
We looked for any statistically significant differences between patients with pure steatosis and NASH, as defined using liver enzymes; and NASH by demographic, anthropometric, clinical, and laboratory variables; identify factors associated with the risk of NAFLD in patients from different BMI groups (BMI < 25, ≥ 25 and < 30, ≥ 30 kg/m2), and aimed to identify the factors associated with the risk of NAFLD in patients aged ≥ 12 and < 18 years.
Statistical Analysis
Statistical analysis and presentation of the results were undertaken using software SAS version 9.4 (SAS Institute, Cary, NC, USA). Characterization of the studied groups was performed using descriptive statistics, including calculation of mean, standard deviation, mode, median, lower and upper quartiles, maximum and minimum values, and proportions or percentages (where appropriate).
Differences between the analyzed groups were investigated using unpaired t test (for normally distributed quantitative variables), and nonparametric tests (including chi-squared test, Mann–Whitney U test, and Wilcoxon signed-rank test). Univariate logistic regression analysis was performed, and odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. The statistical significance threshold was set at p < 0.05. Independent risk factors were identified using multiple regression analysis with a model constructed using variables that were statistically significant in the univariate analysis.
Multivariate regression analysis was used to develop a non-invasive diagnostic test for NAFLD based on the results of the present study. To develop a non-invasive test, the DIREG_L_06725 study cohort was randomly divided into the derivation cohort (90% of the entire sample) and the validation cohort (10% of the entire sample). The first cohort was used to derive an equation to predict the risk of NAFLD (via multiple regression analysis). We included fully non-invasive parameters which could potentially help to predict steatosis in the multiple regression model. We chose parameters with the maximal weight to derive the final equation for the non-invasive diagnostic index, which we termed the St-index. The second cohort was used to validate the diagnostic performance of the St-index (via area under the receiver operating characteristic curve [AUROC], sensitivity, and specificity calculation). The same cohort was used to examine and compare the accuracy of the St-index to existing tests.
Results
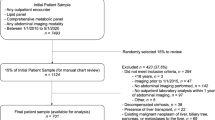
We planned to include data from 48,297 patients from the DIREG_L_06725 study in this analysis (Fig. 1). However, data from 1832 patients from the original cohort were excluded because hepatobiliary ultrasound data were missing, and 16 patients did not meet selection criteria.

Disposition of patients from the DIREG_L_06725 study. HBsAg hepatitis B surface antigen, HCV hepatitis C virus, NAFLD non-alcoholic fatty liver disease
Frequency of NAFLD and Characterization of NAFLD Cohort
The frequency of NAFLD according to age, sex, and BMI is shown in Fig. 2. The frequency of ultrasound-diagnosed NAFLD in eligible DIREG_L_06725 participants was 42.0%. The median age of patients was 57.4 years, 64.1% were women, and 52.6% of patients were employed. Of the female population, 75.1% were in menopause (80.3% defined as postmenopausal and 25.2% reported as having climacteric syndrome). Mean BMI was 31.7 kg/m2, and 87% of individuals had a BMI > 27.0 kg/m2. Ultrasound showed enlarged liver in 58.1% of patients. According to the NAFLD fibrosis score (n = 5991), 93.8% of patients had low risk and 2.0% had high risk of liver fibrosis; according to the fibrosis (FIB)-4 index (n = 13,391), 98.6% of patients had low risk and 0.2% had high risk of liver fibrosis. Conversely, AST/ALT ratio (n = 17,383) and BMI, AST/ALT ratio, diabetes (BARD) scores (n = 17,318) identified 28.6% and 22.2% of patients, respectively, as having a low risk of liver fibrosis, and 71.4% and 77.8% of patients, respectively, as having a high risk of liver fibrosis.

Prevalence of non-alcoholic fatty liver disease according to a age, b sex (unadjusted), and c body mass index
A high proportion of patients had cardiometabolic comorbidities, including hypertension (71.9%), other cardiovascular diseases (24.6%), T2DM (25.7%), metabolic syndrome (35.3%), hypertriglyceridemia (39.0%), hypercholesterolemia (60.0%), and hyperlipidemia (72.6%). Increased ALT was observed in 52% of patients (median 33.00 U/L; Q1, Q3 21.00, 50.00 U/L), increased AST in 46.5% (median 30.00 U/L; Q1, Q3 20.40, 44.00 U/L), and increased GGT in 52.3% (median 40.00 U/L; Q1, Q3 27.00, 62.00 U/L).
Factors Associated with NAFLD
The following factors were found to be positively associated with NAFLD: age and age-related occupational status, weight, BMI (including BMI ≥ 27.0 kg/m2 and ≥ 30.0 kg/m2), waist circumference, WCHR, disability, menopause and climacteric syndrome (perimenopause) in women, arterial hypertension, other cardiovascular diseases, metabolic syndrome, obesity, T2DM, hypertriglyceridemia, hypercholesterolemia, hyperlipidemia, prothrombin level, total cholesterol level, ALT, AST, and GGT. Factors inversely associated with NAFLD were platelet count, ALT/AST ratio, being a student (age was therefore a bias), and female sex (NAFLD frequency 64.1% vs. 62.0%, univariate logistic regression: OR 1.096, p < 0.001; Table 1). However, after adjustment for age, women were at lower risk of NAFLD (OR 0.938, p < 0.001). After adjustment for age, BMI, and WCHR, the OR for developing NAFLD in women was 0.862 (p < 0.001). The most relevant risk factors (age > 35 years, presence of T2DM, and WCHR > 0.54) were used to develop a dichotomous tree of NAFLD risk (Table 2). NAFLD was highly prevalent in patients with cardiometabolic comorbidities (> 54%) and reached the maximal prevalence in patients with T2DM (59.0%).
Development of a Non-Invasive Diagnostic Test Focused on Steatosis (St-index) and Comparison with Other Diagnostic Tools
On the basis of the multiple regression model of factors associated with NAFLD, the non-invasive factors with the highest weight were age, T2DM, and WCHR. The following equation provided maximal AUROC:
where age is the age of the person in years, DM = 0 or 1 when T2DM is absent or present, respectively, and WCHR is the waist circumference/height ratio.
The resulting AUROC curve for the developed predictive model was 0.6527 (Fig. 3). By expanding the “gray zone” interval (an area of values where the discriminatory performance is insufficient), this test can provide good specificity/sensitivity and likelihood ratios at the expense of a high proportion of patients being at “indeterminate” risk:

ROC curve of the St-index according to the multivariate analysis. ROC receiver operating characteristic, St steatosis
We compared the results of our novel formula with three other diagnostic parameters: the HSI, waist circumference, and WCHR, which yielded similar AUROC values (Table 3).
Multivariate regression models in the subgroups of patients aged ≥ 12 and < 18 years and those with BMI < 25.0 kg/m2 (subgroups in which associated factors displayed the greatest effect sizes) showed AUROC values of 0.8243 and 0.7054, respectively.
Distribution of Simple Steatosis and NASH in Cohort of Patients with NAFLD
Increased values for AST, ALT, and GGT were used to diagnose NASH in 17.8% of outpatients with NAFLD, and simple steatosis in 82.3%. The overall frequency of NASH using liver enzymes in the studied population was 7.5%. Liver biopsy results were available for 12 patients in the simple steatosis group and 23 patients in the NASH group, and steatohepatitis was shown in 50% of the simple steatosis (with normal enzymes) and in 56.5% of the patients with NASH.
Further analysis revealed a number of statistically significant differences between the simple steatosis and NASH subgroups, determined using liver enzymes. The following were significantly higher in the group with NASH: female-to-male ratio, BMI, weight, waist circumference, WCHR, climacteric syndrome, T2DM, metabolic syndrome, obesity, hypertriglyceridemia, hypercholesterolemia, hyperlipidemia, total cholesterol, fasting glucose, triglycerides, bilirubin (total, direct and indirect), and gamma globulin. The following were significantly lower in the group with NASH: median age, proportion of postmenopausal women, proportion of patients with disability, and other cardiovascular diseases. Prothrombin time and median height were slightly lower in the NASH group (data not shown).
Discussion
The present analysis of the retrospective observational DIREG_L_06725 study conducted in Russia showed that a higher proportion of patients (42.0%) had NAFLD compared with the proportions reported in a meta-analysis of previous studies, which ranged from 13.5% in Africa to 30.5% in South America [4]. This can most likely be explained by the baseline characteristics of enrolled individuals, who were outpatients visiting medical practitioners (often gastroenterologists), and many of whom were aged > 50 years, obese/overweight, and had cardiometabolic comorbidities. Thus, this study population was not representative of the general population. Patients with NAFLD included in our analysis also had more pronounced signs of overweight/obesity/central adiposity, a higher prevalence of comorbidities/accompanying pathologies, were older on average, and had a higher female-to-male ratio than the general population. Interestingly, the prevalence of arterial hypertension in patients with NAFLD was considerably higher than that of the pooled estimate from previous studies, while the frequency of other comorbidities was close to that reported previously [4]. The frequency of NAFLD in the current analysis is also higher than that in the original DIREG_L_06725 report [19] because we focused on ultrasound screening for NAFLD; therefore, we further limited our inclusion criteria.
The subgroup analysis indicated that female patients with NAFLD were older, more obese, and more frequently had comorbidities and liver enzyme deviations; thus it is the older age of female patients, rather than sex per se, that was responsible for the other factors. It should also be noted that the same inverse age/sex relationship was observed in the overall cohort, showing that older women make up a higher proportion of outpatients. Moreover, this may be associated with the reduced life expectancy of men in Russia, since according to an official local public report in 2017, the female-to-male ratio in Russia was 1.6–1 for individuals aged 60–65 years and 3–1 for those aged 80 years [21].
Another interesting finding was that, compared with older patients, young patients with NAFLD (aged 12–18 years) showed greater deviations from normal ranges in ALT, AST, fasting insulin, and some other laboratory values, but they less frequently had abnormal levels of GGT; the latter may be related to the lower probability of alcohol intake. In this analysis, nearly half of patients with NAFLD had normal levels of liver enzymes (ALT, AST, and GGT). This observation shows that a surrogate blood marker-based approach to NAFLD identification can lead to underdiagnosis. Subgroups of patients having NASH or simple steatosis were distinguished retrospectively on the basis of ALT, AST, and GGT (based on current Russian NAFLD/NASH guidelines). This approach yielded the 7.5% prevalence of NASH in the overall studied population, while in the cohort of patients with NAFLD, 18% had NASH and 82% had pure steatosis. Further analysis revealed a number of statistically significant differences between these subgroups; however, these differences were of no practical clinical value for distinguishing steatosis from steatohepatitis. Of note, a small subgroup of patients had results of biopsy analysis. Histological steatohepatitis was found in a similar proportion of patients diagnosed with NASH and simple steatosis on the basis of liver enzymes. Thus, biopsy results were not consistent with laboratory tests. This finding is consistent with data showing that aminotransferase levels can fluctuate and are not necessarily reflective of steatosis or fibrosis, or indeed the degree of liver inflammation [22]. Therefore, steatohepatitis is definitively distinguishable by histology only, which is not performed routinely in patients with NAFLD. Increased ALT and AST levels can alert physicians to a potential problem [23], but they cannot provide a definitive diagnosis, nor does NASH constitute merely an asymptomatic elevation of enzymes, itself a common clinical misconception. The challenge is thus to develop a standardized approach to steatohepatitis screening and management in patients with NAFLD with or without elevated liver enzymes, and in the absence of liver ultrasound or biopsy. This may need to include not only acknowledging the potential seriousness of suspected “pure” steatosis but also assuming that NASH is present and managing patients accordingly.
While it is clear that NAFLD is associated with cardiovascular disease, it is not yet known whether this association applies to NASH only, or also to simple steatosis [24]. In a 2011 meta-analysis, Musso et al. found that individuals with NASH had higher liver-related mortality than those with simple steatosis, but not higher cardiovascular disease mortality [25]. On the other hand, a considerable number of studies have shown a link between imaging- or biopsy-proven NAFLD in the absence of liver enzyme data, and the development of cardiovascular disease [5]. It has been shown that simple steatosis has the potential to progress regardless of the presence of NASH, with fibrosis, particularly advanced fibrosis, being the most important prognostic factor [25, 26].
Using multivariate regression analysis, we developed a fully non-invasive diagnostic test for NAFLD, the “St-index”. The resulting predictive model was not cumulatively highly accurate, although the AUROC for the St-index was higher than for the other indices tested in the present dataset (HSI, WC, WCHR). More importantly, we achieved high specificity (91.4%) in ruling in and high sensitivity in ruling out (93.8%) NAFLD, using only non-invasive parameters. For HSI, NAFLD was ruled out at a proposed cutoff of < 30, with higher sensitivity than in the original study (98.6% vs. 93.1%), but was ruled in at a proposed cutoff of > 36.0 with much lower specificity than in the original study cohort (25.7% vs. 92.4%) [12]. Thus, in the present study sample, HSI was effective at excluding NAFLD, but ineffective at diagnosing it.
Lower than expected diagnostic efficacy of the indices is not an uncommon finding [10]. Discrepancies in results can be explained by differences in baseline characteristics of the studied populations. These may also include ethnic differences: WCHR was originally proposed for a Taiwanese population [17] and HSI for a South Korean cohort [12]. Other differences include measurement techniques. In a study that determined the accuracy of WC in quantifying longitudinal change, NAFLD diagnosis was based on proton magnetic resonance spectroscopy [16], while other studies used ultrasound. Thus, in the present population, the tests used were less accurate than in the populations from which the tests were derived.
The St-index may, therefore, not provide a way to definitively diagnose steatosis, but to suspect it and provide physicians with a practical decision-making tool to identify patients requiring ultrasound. Use of such a tool in clinical practice may be more readily reimbursed by health insurers who may be reluctant to reimburse diagnostic tests for asymptomatic conditions. Additionally, we revealed that multivariate regression models in the subgroups of patients aged ≥ 12 and < 18 years and individuals with BMI < 25.0 kg/m2 (subgroups in which associated factors displayed the greatest effect sizes) had a more accurate AUROC. This may be because in children, lipid metabolism disturbances, and in particular excess of fat in the liver, are more accurately reflected in an abnormal WCHR. Hence, developing diagnostic tests for these patient categories may be more promising in the future.
Our analysis has some limitations. Firstly, the high prevalence of individuals with gastroenterological/cardiometabolic conditions could potentially hinder identification of factors associated with the risk of NAFLD. The age of patients was ≥ 12 and ≤ 80 years due to the primary dataset inclusion criteria; therefore, our analysis in children is limited and exploratory in nature. NAFLD was diagnosed using ultrasound, which is characterized by high sensitivity and specificity in the diagnosis of grade 2–3 steatosis (84.8% and 93.6%, respectively) [27]. Therefore, it cannot distinguish mild steatosis from severe cases because it lacks sensitivity and is highly operator-dependent. Simple steatosis and NASH were distinguished on the basis of liver enzyme levels, which can likewise only provide an approximate differentiation. In addition, laboratory data were not necessarily presented with unified reference ranges because different ranges were used at the various institutions. Finally, the level of physical activity of the patients was not measured.
Despite these limitations, our large sample size allowed us to detect a variety of factors, with a high level of statistical significance, and the revealed associations support further strong, complex, and multidirectional relationships between NAFLD and excess weight, abdominal obesity, metabolic syndrome and its components, T2DM, and related cardiometabolic disorders. Our findings also support the idea that simple steatosis is almost indistinguishable from NASH in routine clinical practice, thus demanding consistent vigilance in diagnosis. When it comes to diagnosis, our tree of NAFLD risk, where age > 35 years, T2DM presence, and WCHR > 0.54 were predictive factors, could help physicians to distinguish patients with NAFLD more easily. While the newly developed St-index is not accurate enough to diagnose steatosis, it is a fully non-invasive test, unlike BARD, HSI, and ALT/AST measurements. Importantly, it could help physicians to promptly identify potential candidates for further ultrasound testing, which cannot be feasibly performed in all patients presenting to their general practitioners without additional substantiation.
Conclusions
This analysis of Russian outpatients showed a high proportion of patients with NAFLD (42.0%) and NASH (7.5%). NAFLD was associated with excess weight, abdominal obesity, metabolic syndrome and its components, T2DM, and cardiometabolic disorders. Although men are generally known to be at higher risk of NAFLD than women, this is not the case in Russia because of population-related differences in age between men and women. There was histological evidence of steatohepatitis in a similar proportion of patients diagnosed with NASH and simple steatosis using liver enzymes; by comparison, liver enzyme tests alone underestimated the presence of NASH. Liver biopsy is not routine in NAFLD, but simple steatosis and NASH are indistinguishable using clinical and laboratory parameters in the absence of histology. Despite the low AUROC, the new steatosis scale (St-index), combined with the NAFLD tree of risks, provides physicians with a fully non-invasive means for diagnosing NAFLD in routine clinical practice and may help in early identification of patients who need referral for diagnostic verification of steatosis and further testing for inflammation.
References
Masuoka HC, Chalasani N. Nonalcoholic fatty liver disease: an emerging threat to obese and diabetic individuals. Ann N Y Acad Sci. 2013;1281:106–22.
Benedict M, Zhang X. Non-alcoholic fatty liver disease: an expanded review. World J Hepatol. 2017;9:715–32.
Alexander M, Loomis AK, Fairburn-Beech J, et al. Real-world data reveal a diagnostic gap in non-alcoholic fatty liver disease. BMC Med. 2018;16:130.
Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease—meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64:73–84.
Byrne CD, Targher G. NAFLD: a multisystem disease. J Hepatol. 2015;62:S47–64.
Baffy G, Brunt EM, Caldwell SH. Hepatocellular carcinoma in non-alcoholic fatty liver disease: an emerging menace. J Hepatol. 2012;56:1384–91.
Zhou YJ, Li YY, Nie YQ, Huang CM, Cao CY. Natural course of nonalcoholic fatty liver disease in southern China: a prospective cohort study. J Dig Dis. 2012;13:153–60.
Machado MV, Cortez-Pinto H. Non-invasive diagnosis of non-alcoholic fatty liver disease. A critical appraisal. J Hepatol. 2013;58:1007–19.
Hussain HK. Imaging methods for screening of hepatic steatosis. In: Williams R, Taylor-Robinson SD, editors. Clinical dilemmas in non-alcoholic fatty liver disease. Chichester: Wiley; 2016. p. 138–51.
Kahl S, Strassburger K, Nowotny B, et al. Comparison of liver fat indices for the diagnosis of hepatic steatosis and insulin resistance. PLoS One. 2014;9:e94059.
Bedogni G, Bellentani S, Miglioli L, et al. The Fatty Liver Index: a simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006;6:33.
Lee JH, Kim D, Kim HJ, et al. Hepatic steatosis index: a simple screening tool reflecting nonalcoholic fatty liver disease. Dig Liver Dis. 2010;42:503–8.
Kotronen A, Peltonen M, Hakkarainen A, et al. Prediction of non-alcoholic fatty liver disease and liver fat using metabolic and genetic factors. Gastroenterology. 2009;137:865–72.
Fedchuk L, Nascimbeni F, Pais R, et al. Performance and limitations of steatosis biomarkers in patients with nonalcoholic fatty liver disease. Aliment Pharmacol Ther. 2014;40:1209–22.
Motamed N, Sohrabi M, Ajdarkosh H, et al. Fatty liver index vs waist circumference for predicting non-alcoholic fatty liver disease. World J Gastroenterol. 2016;22:3023–30.
Keating SE, Parker HM, Hickman IJ, et al. NAFLD in clinical practice: can simple blood and anthropometric markers be used to detect change in liver fat measured by 1H-MRS? Liver Int. 2017;37:1907–15.
Lin MS, Lin TH, Guo SE, et al. Waist-to-height ratio is a useful index for nonalcoholic fatty liver disease in children and adolescents: a secondary data analysis. BMC Public Health. 2017;17:851.
Ashwell M, Gunn P, Gibson S. Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: systematic review and meta-analysis. Obes Rev. 2012;13:275–86.
Ivashkin V, Drapkina O, Mayev I. The prevalence of non-alcoholic fatty liver disease in patients of outpatient practice in the Russian Federation: the results of the study DIREG 2. Russ J Gastroenterol Hepatol Coloproctol. 2015;25:31–8.
Losekann A, Weston AC, de Mattos AA, et al. Non-alcoholic steatohepatitis (NASH): risk factors in morbidly obese patients. Int J Mol Sci. 2015;16:25552–9.
Population of Russia by gender and age: statistics, distribution. 2017. http://www.statdata.ru/nasel_pol_vozr. Accessed 19 March 2020.
Charatcharoenwitthaya P, Lindor KD, Angulo P. The spontaneous course of liver enzymes and its correlation in nonalcoholic fatty liver disease. Dig Dis Sci. 2012;57:1925–31.
Malakouti M, Kataria A, Ali SK, Schenker S. Elevated liver enzymes in asymptomatic patients—what should I do? J Clin Transl Hepatol. 2017;5:394–403.
Patil R, Sood GK. Non-alcoholic fatty liver disease and cardiovascular risk. World J Gastrointest Pathophysiol. 2017;8:51–8.
Musso G, Gambino R, Cassader M, Pagano G. Meta-analysis: natural history of non-alcoholic fatty liver disease (NAFLD) and diagnostic accuracy of non-invasive tests for liver disease severity. Ann Med. 2011;43:617–49.
Wong VW, Chan WK, Chitturi S, et al. Asia-Pacific working party on non-alcoholic fatty liver disease guidelines 2017-part 1: definition, risk factors and assessment. J Gastroenterol Hepatol. 2018;33:70–85.
Hernaez R, Lazo M, Bonekamp S, et al. Diagnostic accuracy and reliability of ultrasonography for the detection of fatty liver: a meta-analysis. Hepatology. 2011;54:1082–90.
Acknowledgements
Funding
This study, the Rapid Service Fee, and the Open Access Fee were funded by Sanofi Aventis.
Medical Writing, Editorial, and Other Assistance
We would like to thank Atlant Clinical Ltd. Clinical Research Organization for conducting the analysis. Editorial assistance was kindly provided by Marion Barnett, on behalf of Springer Healthcare Communications. This medical writing assistance was funded by Sanofi Aventis.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Disclosures
Kirill Starostin is a Sanofi employee. Igor Maev, Alexey Samsonov, Leonid Lazebnik, Elena Golovanova, Chavdar Pavlov, Elena Vovk, and Vlad Ratziu have nothing to disclose.
Compliance with Ethics Guidelines
The present secondary analysis of the DIREG_L_06725 study was conducted in compliance with the Ethical Principles for Medical Research Involving Human Subjects outlined in the Helsinki Declaration of 1975 (revised in 2000). This was a secondary analysis and authors had no access to patients’ confidential information (names); therefore, no informed consent or ethical approval was required. The primary studies were sponsored by Sanofi and therefore Sanofi had the permission to use the data for secondary analyses.
Data Availability
Qualified researchers may request access to patient level data and related study documents, including the clinical study report, study protocol with any amendments, blank case report form, statistical analysis plan, and dataset specifications. Patient level data will be anonymized and study documents will be redacted to protect the privacy of trial participants. Further details on Sanofi’s data sharing criteria, eligible studies, and process for requesting access can be found at https://www.clinicalstudydatarequest.com.
Author information
Authors and Affiliations
Corresponding author
Additional information
Digital Features
To view digital features for this article go to https://doi.org/10.6084/m9.figshare.12902387.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Maev, I.V., Samsonov, A.A., Lazebnik, L.B. et al. A New, Non-Invasive Scale for Steatosis Developed Using Real-World Data From Russian Outpatients to Aid in the Diagnosis of Non-Alcoholic Fatty Liver Disease. Adv Ther 37, 4627–4640 (2020). https://doi.org/10.1007/s12325-020-01493-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-020-01493-w