
Abstract
Introduction
Long-standing acanthamoeba keratitis (AK) may result in corneal neovascularization, extension of the infiltrate to the limbus or sclera, broad peripheral synechiae, mature cataract or ischemic posterior segment inflammation. We investigated the impact of early emergency penetrating keratoplasty (PKP) in therapy-resistant cases among the patients of a highly specialized tertiary care center.
Methods
In this retrospective, observational cohort within a single institution, we collected data on best-corrected visual acuity (BCVA), epithelial wound healing, graft survival and secondary complications of AK patients who underwent PKP. A total of 23 eyes of 23 patients diagnosed with acute, therapy-resistant AK between 2006 and 2015 were enrolled. Postoperative combined topical treatment was tapered for 6–9 months.
Results
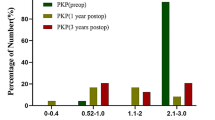
Eyes were grouped based on preoperative disease duration as shorter (group 1) or longer (group 2) than the median. The median was 5.3 (0.66–36) months. The BCVA in group 1 (20/44 ± 20/18; 0.32 ± 0.18 logMAR) was significantly better than in group 2 (20/1200 ± 20/1133; 1.28 ± 0.89; logMAR); p = 0.015. Persisting epithelial defects occurred in 5 patients (50%) of group 1 and in 10 patients (77%) of group 2. In 5 eyes (group 2), no epithelial healing could be achieved. After 36 months, graft survival (Kaplan–Meier) was 78% (18 grafts) for all patients (90% in group 1 and 44% in group 2).
Conclusion
PKP à chaud within 5.3 months after first symptoms of therapy-resistant AK seems to result in better final BCVA than delayed graft surgery if the disease is resistant to a classical topical triple therapy. In addition, early PKP may have a favorable impact on epithelial healing and graft survival.
Funding
We thank the Alexander von Humboldt Foundation for supporting the work of Prof. N. Szentmáry at the Department of Ophthalmology of Saarland University Medical Center in Homburg/Saar, Germany. We thank the University of Saarland for funding the medical writing assistance and the Rapid Service Fees. The funding organisation had no role in the design or conduct of this research.







Similar content being viewed by others


References
Naginton J, Watson PG, Playfair TJ, McGill J, Jones BR, Steele AD. Amoebic infection of the eye. Lancet. 1974;2:1537–40.
Meltendorf C, Duncker G. Akanthamöben-Keratitis. Klin Monbl Augenheilkd. 2011;228:R29–43.
Szentmary N, Daas L, Matoula P, Goebels S, Seitz B. Akanthamöbenkeratitis. Ophthalmologe. 2013;110:1203–10.
Claerhout I, Goegebuer A, Van Den Broecke C, Kestelyn P. Delay in diagnosis and outcome of Acanthamoeba keratitis. Graef Arch Clin Exp Ophthalmol. 2004;242:648–53.
Daas L, Szentmary N, Eppig T, et al. Das Deutsche Akanthamöbenkeratitis-Register: Erste Ergebnisse einer multizentrischen Erhebung. Ophthalmologe. 2015;112:752–63.
Lorenzo-Morales J, Khan NA, Walochnik J. An update on Acanthamoeba keratitis: diagnosis, pathogenesis and treatment. Parasite. 2015;22:10.
Awwad ST, Heilman M, Hogan RN, et al. Severe reactive ischemic posterior segment inflammation in acanthamoeba keratitis: a new potentially blindign syndrome. Ophthalmology. 2007;114:313–20.
Blackman HJ, Rao NA, Lemp MA, Visvesvara GS. Acanthamoeba keratitis successfully treated with penetrating keratoplasty: suggested immunogenic mechanisms of action. Cornea. 1984;3:125–30.
Dart JK, Saw VP, Kilvington S. Acanthamoeba keratitis: diagnosis and treatment update 2009. Am J Ophthalmol. 2009;148:487–99.
Robaei D, Carnt N, Minassian DC, Dart JK. Therapeutic and optical keratoplasty in the management of Acanthamoeba keratitis: risk factors, outcomes, and summary of the literature. Ophthalmology. 2015;122:17–24.
Illingworth CD, Cook SD. Acanthamoeba keratitis. Surv Ophthalmol. 1998;42:493–508.
Awwad ST, Parmar DN, Heilman M, Bowman RW, McCulley JP, Cavanagh HD. Results of penetrating keratoplasty for visual rehabilitation after Acanthamoeba keratitis. Am J Ophthalmol. 2005;140:1080–4.
Hager T, Hasenfus A, Stachon T, Seitz B, Szentmary N. Crosslinking and corneal cryotherapy in acanthamoeba keratitis—a histological study. Graefes Arch Clin Exp Ophthalmol. 2015;254:149–53.
Küchle M, Seitz B, Langenbucher A, Naumann GO. Nonmechanical excimer laser penetrating keratoplasty for perforated or predescemetal corneal ulcers. Ophthalmology. 1999;106:2203–9.
Seitz B, Resch M, Schlötzer-Schrehardt U, Hofmann-Rummelt C, Sauer R, Kruse FE. Histopathology and ultrastructure of human corneas after amniotic membrane transplantation. Arch Ophthalmol. 2006;124:1487–90.
Robaei D, Carnt N, Minassian DC, Dart JK. The impact of topical corticosteroid use before diagnosis on the outcome of Acanthamoeba keratitis. Ophthalmology. 2014;121:1383–8.
Kashiwabuchi RT, de Freitas D, Alvarenga LS, et al. Corneal graft survival after therapeutic keratoplasty for Acanthamoeba keratitis. Acta Ophthalmol. 2008;86:666–9.
Ficker LA, Kirkness C, Wright P. Prognosis for keratoplasty in Acanthamoeba keratitis. Ophthalmology. 1993;100:105–10.
Illingworth CD, Cook SD, Karabatsas CH, Easty DL. Acanthamoeba keratitis: risk factors and outcome. Br J Ophthalmol. 1995;79:1078–82.
Chen WL, Wu CY, Hu FR, Wang IJ. Therapeutic penetrating keratoplasty for microbial keratitis in Taiwan from 1987 to 2001. Am J Ophthalmol. 2004;137:736–43.
Sarnicola E, Sarnicola C, Sabatino F, Tosi GM, Perri P, Sarnicola V. Early Deep Anterior Lamellar Keratoplasty (DALK) for Acanthamoeba keratitis poorly responsive to medical treatment. Cornea. 2016;35:1–5.
Ehlers N, Hjortdal J. Are cataract and iris atrophy toxic complications of medical treatment of acanthamoeba keratitis? Acta Ophthalmol Scand. 2004;82:228–31.
Herz NL, Matoba AY, Wilhelmus KR. Rapidly progressive cataract and iris atrophy during treatment of Acanthamoeba keratitis. Ophthalmology. 2008;115:866–9.
Daas L, Viestenz A, Schnabel PA, et al. Confocal microscopy as an early relapse marker for Acanthamoeba keratitis. Clin Anat. 2018;31:60–3.
Dohlman CH, Terada H. Keratoprosthesis in pemphigoid and Stevens-Johnson syndrome. Adv Exp Med Biol. 1998;438:1021–5.
Bach M, Kommerell G. Sehschärfebestimmung nach Europäischer Norm: wissenschaftliche Grundlagen und Möglichkeiten der automatischen Messung. Klin Monbl Augenheilkund. 1998;212(4):190–5.
Acknowledgements
Funding
We thank the Alexander von Humboldt Foundation for supporting the work of Prof. N. Szentmáry at the Department of Ophthalmology of Saarland University Medical Center in Homburg/Saar, Germany. We thank the University of Saarland for funding the medical writing assistance and the Rapid Service Fees. The funding organisation had no role in the design or conduct of this research.
Medical Writing Assistance
Language editing and assistance for this article was provided by Chrisitna Turner of the ACT-Fachübersetzunge and was funded by the University of Saarland.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Disclosures
Kornélia L. Laurik, Nóra Szentmáry, Loay Daas, Achim Langenbucher and Berthold Seitz have nothing to disclose.
Compliance with Ethics Guidelines
All procedures performed in our study involving human participants were in accordance with the ethical standards of the Ethical Committee of the Medical Association of Saarland and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent for participation and publication of patient data was obtained from all individual participants included in the study.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
We hereby thank all the participants of the study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced Digital Features
To view enhanced digital features for this article go to https://doi.org/10.6084/m9.figshare.8546129.
Rights and permissions
About this article

Cite this article
Laurik, K.L., Szentmáry, N., Daas, L. et al. Early Penetrating Keratoplasty À Chaud May Improve Outcome in Therapy-Resistant Acanthamoeba Keratitis. Adv Ther 36, 2528–2540 (2019). https://doi.org/10.1007/s12325-019-01031-3
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-019-01031-3