
Abstract
Introduction
Patients experience numerous transitions, including changes in clinical status, pharmacologic treatment and prophylaxis, and progression through the physical locations of their healthcare setting as they advance through a venous thromboembolism (VTE) clinical experience. This review provides an overview of these transitions and highlights how they can impact clinical care.
Methods
Major public resources (PubMed, MEDLINE, and Google Scholar) were searched using various combinations of the terms: “venous thromboembolism”, “deep vein thromboses”, “pulmonary embolism”, “transitions in care”, and “hospital protocols” to identify narrative reviews, professional guidelines, or primary manuscripts reporting protocol development strategies and/or clinical data, published in English from 2010 through January 2015. The studies included in this review were selected on the basis of extensive reading of the literature and the author’s clinical expertise.
Results
VTE treatment and prophylaxis is a dynamic process requiring ongoing patient assessments and adjustments to therapeutic strategies as the patient progresses through various hospital and outpatient settings. Throughout these transitions in care, physicians need to be vigilant of any changes in the patient’s clinical condition which may impact the patient’s risk of VTE, and re-evaluate the intervention(s) employed when such changes occur. A standardized, interdisciplinary VTE clinical pathway developed for medical patients with acute VTE resulted in decreased utilization of hospital resources and healthcare costs, suggesting that further research is warranted in this area.
Conclusion
The prevention and management of VTE can be optimized by the development and local implementation of standardized evidence-based clinical pathways.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Pathological blood clots in the venous circulation, generally known as deep vein thromboses (DVT), usually arise via one of three pathogenic processes, sometimes referred to as Virchow’s triad [1]: (1) hypercoagulability of the blood, (2) reduced or static blood flow, and (3) vessel damage because of injury or disease [2, 3]. Pulmonary embolism (PE) results when one or more of these abnormal clots break away from the original site and travel to the lungs where they can lead to serious consequences. Together, DVT and PE comprise venous thromboembolism (VTE) [4]. Approximately 350,000–900,000 patients in the US experience a VTE episode each year, and an estimated 100,000 of these will die because of related complications—sobering statistics which define the significant unmet medical need for this patient population [4]. For patients who experience an initial VTE episode, approximately 50% go on to develop post-thrombotic syndrome, which is characterized by discomfort, discoloration, swelling, and even ulcers in the affected limb in severe cases [4, 5].
Current treatment guidelines support a number of anticoagulation approaches, and these are dependent on the clinical details of an individual VTE event, the stage of the disease, and any associated co-morbidities. For example, treatment with low molecular weight heparin (LMWH) or anticoagulation with a direct oral anticoagulant (DOAC) is recommended for acute episodes of VTE [6]. For proximal DVT or PE, at least 3 months of treatment is recommended when these events are associated with either a surgical procedure or an unrelated and transient risk factor [5, 6]. On the other hand, if the VTE is associated with active cancer, then extended therapy is recommended with LMWH, which is preferred over use of vitamin K antagonists [6]. LMWH has also been reported to have similar efficacy in preventing recurrent VTE, and to increase the frequency of thrombus regression [7]. In addition, the United States Food and Drug Administration has recently approved four DOACs for the treatment and/or prophylaxis of VTE; apixaban (for the prophylaxis of DVT, which may lead to PE in patients who have undergone hip or knee replacement surgery; for the treatment of DVT and PE; and for the reduction in the risk of recurrent DVT and PE following initial therapy) [8], dabigatran (for the treatment of DVT and PE in patients who have been treated with a parenteral anticoagulant for 5–10 days; and to reduce the risk of recurrence of DVT and PE in patients who have been previously treated) [9], edoxaban (for the treatment of DVT and PE following 5–10 days of initial therapy with a parenteral anticoagulant) [10], and rivaroxaban (for the treatment of DVT and PE; for the reduction in the risk of recurrent DVT and PE; and for the prophylaxis of DVT, which may lead to PE in patients undergoing knee or hip replacement surgery) [11]. The role that each of these newer agents will play in the management of VTE will be defined by ongoing clinical trials and real-world experience over the next few years.
As a VTE episode progresses, patients will most likely transition through a number of defined clinical settings in advanced healthcare environments [12]. These transitions may include a progression from the emergency room (ER) to the intensive care unit (ICU). Then, once the acute episode is stable, the patient may be transferred to the “step-down” unit before being sent to a general medical–surgical floor, and so forth, until the patient is finally discharged [13]. These physical transitions can parallel the patient’s progression through the various stages of a VTE episode including abnormal clotting events and their sequelae, immediate treatment and long-term management, and the potential for readmission because of recurrent VTE [13].
Therefore, the initial VTE risk assessment performed at first contact with the healthcare system should require re-evaluation after each transition. Any changes noted in the patient’s overall VTE risk evaluation resulting from their updated clinical status should call for reconsideration of their ongoing VTE prophylaxis, and any planned long-term regimens [12, 14].
The objective of this narrative review was to present an overview of the numerous transitions patients experience as they progress through VTE clinical events, and how these transitions can impact their clinical care.
Methodology
Major public resources (PubMed, MEDLINE, and Google Scholar), were searched using various combinations of the terms: “venous thromboembolism”, “deep vein thromboses”, “pulmonary embolism”, “transitions in care”, and “hospital protocols” to identify narrative reviews, professional guidelines, or primary manuscripts reporting protocol development strategies and/or clinical data, published in English from 2010 through January 2015. The publications included in this review were selected on the basis of extensive reading of the literature and expert clinical opinion. They include guidelines that define management strategies for the prophylaxis and management of VTE patients, as well as reports on how the development of standardized clinical pathways can improve management as a patient moves through the various stages of their disease process and related clinical care areas.
Compliance with Ethics Guidelines
This article is based on previously conducted studies and does not involve any new studies of human or animal subjects performed by any of the authors.
Changes in Clinical Status may Warrant Updates to a Patient’s Overall Risk for VTE
The American College of Chest Physicians’ evidence-based clinical practice guidelines for VTE prophylaxis, as well as those from the International Consensus Statement on the prevention and treatment of VTE, are defined by a patient’s overall VTE risk and medical status [15–17]. The relative risk of VTE, including both DVT and/or PE, that may arise during a hospital stay can vary significantly depending on the underlying medical condition of the patient. However, while the number and type of VTE risk factors may generally inform overall risk of VTE, there does not yet exist a clinically validated method to accurately predict specific VTE risk for an individual patient [13]. The general incidence of DVT events in hospitalized patients varies by their medical/surgical service, as shown in Table 1 [13].
For medical patients in the acute phase of their hospitalization, and who are considered to be at low risk of thrombosis, pharmacologic or mechanical prophylaxis is not recommended [15]. However, if acutely ill medical patients are at increased risk of thrombosis because of immobilization and concurrent risk factors or co-morbidities (e.g., age >40 years, prior history of VTE, serious infection), then thromboprophylaxis with LMWH, low-dose unfractionated heparin (LDUH) two or three times daily, or fondaparinux is recommended [15, 17]. However, it should be noted that extension of thromboprophylaxis beyond the timeframe when the patient is immobilized, or the full course of the acute hospital stay, is not recommended in this patient population [15]. Prophylaxis with LMWH rather than LDUH is also preferred as it may be administered as a single injection daily, is associated with less hemorrhagic complications and less heparin-induced thrombocytopenia [17].
For patients with suspected or proven hemorrhagic stroke or those with ischemic stroke in whom the risks of prophylactic anticoagulant therapy exceed the benefits, mechanical thromboprophylaxis with graduated compression stockings (GCS) or intermittent pneumatic compression device (IPCD) is recommended [17].
Mechanical thromboprophylaxis with GCS or IPCD may also be considered in patients in whom anticoagulant thromboprophylaxis is contraindicated due to current bleeding or a high risk of bleeding (e.g., patients with multiple bleeding risk factors, or those with active gastroduodenal ulcers, recent bleeding [in the 3 months preceding admission], or thrombocytopenia [<50,000 cells/μL]). However, anticoagulant prophylaxis should be initiated, in place of the mechanical thromboprophylaxis, in cases where the bleeding risk decreases and the risk of VTE persists [15].
Recommendations for thromboprophylaxis for patients who will undergo major orthopedic surgery include the use of one of the following pharmacologic or mechanical approaches: LMWH; fondaparinux; dabigatran, apixaban, rivaroxaban (for total hip or knee arthroplasty, but not hip fracture surgery); LDUH; adjusted-dose vitamin K antagonist; or an IPCD for a minimum of 10–14 days [16, 17]. Aspirin, in conjunction with compression devices, can be used for the prophylaxis of VTE in high-risk patients undergoing orthopedic surgery [18]. Note that the oral factor Xa inhibitor anticoagulants, namely apixaban and rivaroxaban, have been FDA approved for DVT prophylaxis following hip or knee replacement surgery. The recommended duration of such prophylaxis is 10–14 days although it can be extended for up to 35 days [16].
For patients undergoing major orthopedic surgery who are at an increased risk for bleeding, either an IPCD or no prophylaxis is recommended [16]. Inferior vena cava filters are not recommended for primary prevention in patients who have contraindications to both pharmacologic and mechanical thromboprophylaxis [16]. Further, Doppler (or duplex) ultrasonography as a screening tool is not recommended before hospital discharge [16]. Additionally, thromboprophylaxis is not recommended in patients with isolated lower extremity injuries requiring immobilization, or in patients without prior history of VTE who are undergoing knee arthroscopy [16].
Patients with cancer have a 2-year cumulative incidence of VTE between 0.8% and 8%, depending on the type of malignancy [19, 20]. Since VTE is a major cause of morbidity and mortality in cancer patients, they may benefit from prophylaxis and careful monitoring for changes in their VTE risk levels [20].
Thromboprophylaxis is generally not recommended for outpatients with cancer who have no additional risk factors for VTE [15]; however, for some high-risk patients this may be a prudent approach [21]. On the other hand, the majority of patients with cancer who have been admitted to a hospital will require VTE prophylaxis throughout their stay [21]. In particular, it is suggested that multiple myeloma patients who receive anti-angiogenesis agents, along with chemotherapy and/or dexamethasone, receive thromboprophylaxis with either LMWH or low-dose aspirin [21].
Thromboprophylaxis should be initiated prior to major surgery for cancer, and then extended for 7–10 days post-operatively. In patients at high risk for VTE, prophylaxis should be extended to 4 weeks after the surgery [21]. For the first 5–10 days of prophylaxis for VTE, LMWH is recommended. This can be used for longer term prophylaxis (approximately 6 months) [21, 22].
Current guidelines do not recommend the use of DOACs for the treatment of VTE in patients with cancer [21]. This is likely a result of the low enrolment percentage of patients with cancer. However, the results from a number of ongoing clinical trials evaluating their safety and efficacy in this patient population are eagerly awaited to assess their potential use [23].
Overall VTE risk in patients with cancer should be periodically assessed because of the likelihood that as their clinical status changes, their VTE risk profile may change as well [21]. As an adjunct to any ongoing treatments, oncology clinicians should educate their patients regarding the signs and symptoms of VTE [21].
As illustrated by the various guidelines and recommendations, VTE prophylaxis and treatment are dynamic processes requiring ongoing assessment and periodic updates to their management. The intermediate steps and particular inflection points for each patient will depend on their underlying medical condition as they transition through the healthcare system.
Transitions in Medical Status and Management
As a patient is diagnosed and treated for a VTE, they can be expected to transition through various stages of care, while concurrently passing through distinct clinical care environments in a formal healthcare setting [24, 25]. For example, patients will likely present to the ER where, depending on the severity of the event, they may be admitted to the ICU to receive aggressive medical intervention and nursing care. When their clinical status improves, patients may proceed as medically necessary to the “next” hospital unit. Upon discharge from the hospital, they will need appropriate follow-up and care, including ongoing anticoagulation therapy appropriate for their underlying condition.
In parallel, patients can also transition through stages of care as their disease progresses from an acute event to initial treatment and response and on through what may become a chronic condition. Upon possible readmission, patients re-enter the healthcare system with a more extensive medical history, which will need to be considered as “next-step” treatment options are considered. If re-admitted to the same facility, then continuity of care should be straightforward. If admitted to another facility, however, they will most likely require additional, sometimes duplicative, workup before appropriate treatment decisions can be made.
One of the key questions for healthcare professionals is how to identify those patients who might be at risk of a recurrence and how to best mitigate their chances of such. Strategies to be considered should include appropriate prophylaxis with a change of anticoagulant if compliance or adherence is a concern.
Patients often experience a number of transition events as their treatment paradigm develops over time. These will most likely include different drugs and therapeutic regimens, beginning with their initial treatment for an acute VTE episode, on through sub-acute treatment in the hospital setting, and finally as they and their healthcare team select appropriate therapeutic approaches for the prevention of recurrent episodes post-discharge.
The first stage of treatment usually begins when a patient presents with an acute episode. As a consequence of their rapid onset of action, the first agent is usually a parenteral anticoagulant such as LMWH, fondaparinux, or unfractionated heparin (UFH), dosed either subcutaneously or by intravenous infusion, to achieve a rapid anticoagulation effect [24]. The guidelines recommend concurrent initiation of warfarin for ongoing therapy, since this drug has the benefit of oral administration. It should be noted that the process of transitioning from the parenteral agent to full reliance on warfarin can take several days since its effects on clotting are predicated on time-dependent depletion of individual vitamin K-dependent clotting factors synthesized by the liver (protein C, protein S, factors II, VII, IX, and X) [24]. Individual institutions likely have identified the role of fondaparinux in the acute setting, some limiting this agent to those patients more prone for heparin-induced thrombocytopenia (HIT). While both are legitimate options, when faced with a choice of UFH or LMWH, the latter has the advantages of improved pharmacokinetics and bioavailability. Use of LMWH also obviates the requirement to check a patient’s activated partial thromboplastin time (aPTT) and make the necessary adjustments needed to achieve therapeutic anticoagulation if UFH is administered by continuous infusion. In addition, UFH increases the risk of osteopenia and has a higher incidence of HIT [26–28]. Additionally, a course of UFH (administered first as a bolus of 5000 U followed by an infusion at the rate of 32,000 U/24 h) typically results in the “one-third effect.” That is, at 6 h post-initiation, approximately one-third of patients have sub-therapeutic levels, and approximately one-third have supra-therapeutic levels, so that at this time point, only one-third of patients are in the therapeutic aPTT range [29, 30]. By 24 h, approximately two-thirds of patients are in the therapeutic range, still leaving approximately one-third of patients needing further adjustment in their dosing [29, 30]. Therefore, despite the lower drug acquisition cost of UFH, the lack of mandatory lab testing, the improved efficacy and safety along with a lower nursing burden would seem to favor LMWH.
In most cases, before a patient is ultimately transferred home (from the hospital, rehabilitation center, nursing care facility, etc.), the injectable agent is replaced by an oral one to minimize administration logistics and foster patient adherence. The historical standard of care has been to switch the patient to warfarin, an agent that can be effective when regular monitoring ensures appropriate dosing to achieve its narrow therapeutic window (international normalized ratio [INR] 2–3). In fact, this is only accomplished 55–60% of the time [26]. However, this can be challenging [27]. In addition, warfarin therapy is a leading cause of medication-associated errors, adverse events, and drug–drug and drug–food interactions. Together, these therapeutic difficulties have set the stage for the development of the current generation of DOACs.
Further, if a patient has not achieved stable anticoagulation on warfarin, is intolerant of this therapy, or has been re-admitted to the hospital because of another VTE-related event resulting from medication non-adherence, then it may be prudent to consider a switch to one of the newer DOACs (apixaban, dabigatran, edoxaban, or rivaroxaban) in accordance with treatment guidelines and appropriate prescribing information for each agent [8–11].
Clinical care guidelines have been established for switching patients between individual DOAC therapies [31], and these include transitions from parenteral to oral medications such as warfarin and the DOACs [31]. Suggested guidelines for such transitions are presented in more detail in Table 2.
Another area of interest is bridging anticoagulation, which can be defined as treatment with a short-acting anticoagulant (either LMWH administered subcutaneously, or UFH via IV infusion) in patients where vitamin K antagonist therapy has been interrupted, and the INR is outside the therapeutic range [32]. LMWH and fondaparinux have predictable pharmacokinetic and pharmacodynamic properties, including rapid anticoagulant effectiveness, and low risk of clinically significant drug interactions [33]. Bridging therapy can be used to carefully balance the relative risks of thromboembolism versus pathological bleeding during high-risk periods associated with certain diagnostic, therapeutic, and/or surgical procedures. Specific evidence-based bridging protocols are recommended for individual clinical settings. For example, in patients with VTE who are at high risk for thromboembolism, bridging anticoagulation is recommended during an interruption of vitamin K antagonist therapy. However, in patients at low risk for thromboembolic events, bridging is not recommended [32]. A complete discussion of this topic is beyond the scope of this manuscript, but the reader is directed to any of the excellent reviews that address this topic in detail.
Clinical Pathways of Acute VTE
Acute VTE is a prevalent and potentially deadly condition, especially when it is undiagnosed or undertreated. Furthermore, if a VTE episode progresses to an advanced stage, management may be expensive. From 2007 to 2009, the annual incidence of VTE as a discharge diagnosis of adult hospitalizations was 550,000. This disease process continues to receive attention as a preventable public health issue and patient safety measure. Evidence-based protocols for diagnosing and managing this complex condition are continuously being developed [4].
One general strategy to optimize care for the prevention and management of VTE would be to develop a protocol based on a reiterative process that is defined by a number of quality control steps, and progressive self-assessments to monitor the effectiveness of the evolving pathway (Fig. 1).

Sequence and relationships of steps in a quality improvement project aimed at reducing the incidence of hospital-acquired venous thromboembolism [13]. aA VTE protocol offers decision support for risk stratification and a menu of appropriate prophylaxis options for each level of risk. VTE venous thromboembolism, QI quality improvement
Key steps in this process would include the identification of existing protocols and current practices, and how “next step” clinical decisions are made and implemented for individual patients depending on their medical status [13]. To move beyond the status quo, existing protocols would need to be refined, with the eventual goal of defining evidence-based protocols that standardize procedures for each patient population and clinical setting.
To this end, the current “delivery of care” protocols would need to be analyzed to identify the steps that have the highest impact on outcome quality. Investigators would need to establish and track performance metrics at regular intervals. This process would depend on inexpensive, reliable, and direct assessments of clinical regimens and outcomes.
More specifically, a VTE assessment protocol would need to be an integral part of the overall clinical workflow for patients in the hospital setting, one which would fit into any pre-existing metrics program already underway at the institution in question. These ongoing cycles of Plan–Do–Study–Act could then be subject to interim analyses, with ongoing re-assessments to improve the process as needed.
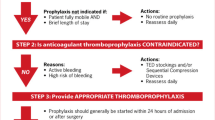
Figure 2 outlines the general strategy for monitoring clinical pathway assessments and patient outcomes, which include initial VTE risk assessment at intake, identification of possible need for initial prophylaxis, and appropriate follow-up with relevant clinical support services. Throughout the hospitalization, intermediate outcomes are assessed at regular intervals (or when any relevant changes in clinical status have been identified) to ensure that the patient is receiving appropriate VTE prophylaxis and/or care.

Flowchart detailing individual steps and assessments in the VTE care pathway. VTE venous thromboembolism
Development and Optimization of a Clinical Pathway for VTE Quality Control/Care
In a hospital setting, significant variations of VTE care and outcomes were identified based on medical coverage payer. A VTE clinical pathway was developed to standardize patient care (thereby mitigating disparities), minimize unnecessary utilization of hospital resources, and educate both patients and providers [34]. This interdisciplinary pathway was focused on medical patients with acute VTE. The strategy comprised the development of prepared order sets, system-wide educational programs and tools, follow-up phone calls with patients, and clear and coordinated post-hospital care [34].
Hospital admission outcomes, length of stay, and reutilization were stratified by payer source in study patients (n = 241) and historical data (n = 234) (Table 3). Of the study patients, 107 presented with DVT (44.4%) and 134 with a PE (55.6%) [34]. Significant differences were noted in the rate at which VTE patients were admitted, (65.9 versus 79.1%, uninsured versus insured, respectively; P = 0.032). For VTE patients admitted to the hospital who followed a clinical pathway, the length of stay decreased from 4.4 to 3.1 days (P < 0.001), and a similar trend was seen for the uninsured patients (from 5.9 to 3.1 days; P < 0.001) [34]. Interestingly, this reduction did not translate into a decrease in ED revisits or readmission rates. However, there was a significant reduction in overall hospital expenses for those patients admitted under a pathway ($7038), compared with those who were treated according to historical procedures ($10,324; P = 0.044). Also, this reduction was most pronounced in the uninsured cohort, where the costs for pathway patients ($6375) were significantly lower than for the patients treated according to historical procedures ($14,420; P = 0.005) [34]. Further work in this field is necessary.
Establishing an interdisciplinary and standardized pathway of care for VTE patients significantly lowered the utilization of hospital resources and healthcare costs. Of importance to institutions that provide care to uninsured patients, overall cost savings were especially significant for this population [34]. The findings of this study present a model for improving coordination of transitional care within local community health clinics, and also the delivery of appropriate medical care to vulnerable populations with chronic medical conditions [34].
Conclusions
VTE is a common, dangerous, and potentially expensive clinical condition that can benefit from local implementation of standardized, evidence-based clinical pathways to improve individual patient care and minimize unnecessary utilization of hospital resources. These should include quality control steps to monitor the effectiveness of the evolving pathway, identifying steps that have the highest impact on outcome quality and refining the process as necessary.
Practitioners should continue to be ever vigilant in their patient’s VTE risk assessment, understanding that this may change commensurate with changes in the patient’s condition or physical location. Hence, an evaluation of the intervention(s) employed, pharmacological and/or mechanical, should occur with such changes. In this way, VTE patients will be satisfactorily managed as they transition though the healthcare system.
References
Bagot CN, Arya R. Virchow and his triad: a question of attribution. Br J Haematol. 2008;143(2):180–90 (Epub 2008/09/12).
Deep vein thrombosis (DVT). 2014 [cited 2014 Sept 3]; Available from: http://www.mayoclinic.org/diseases-conditions/deep-vein-thrombosis/basics/definition/con-20031922.
Agency for Healthcare Research and Quality. Venous thromboembolism (VTE). Agency for Healthcare Research and Quality; 2014 [cited 2014 Sept 3]; Available from: http://www.guideline.gov/content.aspx?id=14422.
Streiff MB, Brady J, Grant AM, Grosse SD, Wong B, Popovic T. CDC grand rounds: preventing hospital-associated venous thromboembolism. Centers for Disease Control and Prevention; 2014.
Baldwin MJ, Moore HM, Rudarakanchana N, Gohel M, Davies AH. Post-thrombotic syndrome: a clinical review. J Thromb Haemost. 2013;11(5):795–805.
Kearon C, Akl EA, Comerota AJ, Prandoni P, Bounameaux H, Goldhaber SZ, et al. Antithrombotic therapy for VTE disease: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):e419S–94S (Epub 2012/02/15).
Gonzalez-Fajardo JA, Martin-Pedrosa M, Castrodeza J, Tamames S, Vaquero-Puerta C. Effect of the anticoagulant therapy in the incidence of post-thrombotic syndrome and recurrent thromboembolism: comparative study of enoxaparin versus coumarin. J Vasc Surg. 2008;48(4):953–9.
Bristol-Meyers Squibb I. Eliquis prescribing information. Bristol-Meyers Squibb Company; 2015.
Ingelheim B. Pharmaceuticals I. Pradaxa prescribing information. Ridgefield: Boehringer Ingelheim Pharmaceuticals, Inc; 2015.
Daiichi Sankyo I. Savaysa prescribing information. Parsippany: Daiichi Sankyo Inc.; 2015. p. 31.
Janssen Pharmaceuticals I. Xarelto prescribing information. Titusville: Janssen Pharmaceuticals, Inc; 2015.
Lenchus JD. Strategies for venous thromboembolism prophylaxis programs. Postgrad Med. 2011;123(6):91–101 (Epub 2011/11/23).
Maynard G, Stein J. Preventing hospital-acquired venous thromboembolism: a guide for effective quality improvement. In: Quality AfHRa, editor. Rockville: AHRQ; 2008.
Nieto JA, Camara T, Camacho I. Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients. A retrospective multicenter study. Eur J Intern Med. 2014;25(8):717–23 (Epub Aug 1, 2014).
Kahn SR, Lim W, Dunn AS, Cushman M, Dentali F, Akl EA, et al. Prevention of VTE in nonsurgical patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):e195S–226S.
Falck-Ytter Y, Francis CW, Johanson NA, Curley C, Dahl OE, Schulman S, et al. Prevention of VTE in orthopedic surgery patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):e278S–325S.
Nicolaides AN, Fareed J, Kakkar AK, Comerota AJ, Goldhaber SZ, Hull R, et al. Prevention and treatment of venous thromboembolism—International Consensus Statement. Int Angiol J Int Union Angiol. 2013;32(2):111–260 (Epub 2014/01/10).
Stewart DW, Freshour JE. Aspirin for the prophylaxis of venous thromboembolic events in orthopedic surgery patients: a comparison of the AAOS and ACCP guidelines with review of the evidence. Ann Pharmacotherapy. 2013;47(1):63–74 (Epub 2013/01/18).
Chew HK, Wun T, Harvey D, Zhou H, White RH. Incidence of venous thromboembolism and its effect on survival among patients with common cancers. Arch Intern Med. 2006;166(4):458–64.
Mandala M, Falanga A, Roila F. Management of venous thromboembolism (VTE) in cancer patients: ESMO clinical practice guidelines. Ann Oncol. 2011;22(Suppl 6):vi85–92.
Lyman GH, Khorana AA, Kuderer NM, Lee AY, Arcelus JI, Balaban EP, et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol Off J Am Soc Clin Oncol. 2013;31(17):2189–204.
Tardy B, Chalayer E, Chapelle C, Mismetti P. The effect of low molecular weight heparin on survival in cancer patients: an updated systematic review and meta-analysis of randomized trials: comment. J Thromb Haemost. 2014;12(9):1572–3.
Lee AY, Carrier M. Treatment of cancer-associated thrombosis: perspectives on the use of novel oral anticoagulants. Thromb Res. 2014;133(Suppl 2):S167–71.
Guyatt GH, Akl EA, Crowther M, Gutterman DD, Schuunemann HJ. Executive summary: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):7S–47S.
National Clinical Guideline Centre—Acute and Chronic Conditions (UK). Venous thromboembolism: reducing the risk of venous thromboembolism (thrombosis and pulmonary embolism) in Patients Admitted to Hospital. 2010.
Hirsh J, Levine MN. Low molecular weight heparin. Blood. 1992;79(1):1–17 (Epub 1992/01/01).
Junqueira DR, Perini E, Penholati RR, Carvalho MG. Unfractionated heparin versus low molecular weight heparin for avoiding heparin-induced thrombocytopenia in postoperative patients. Cochrane Database Syst Rev. 2012;9:CD007557 (Epub 2012/09/14).
Walenga JM, Prechel M, Jeske WP, Bakhos M. Unfractionated heparin compared with low-molecular-weight heparin as related to heparin-induced thrombocytopenia. Curr Opin Pulm Med. 2005;11(5):385–91 (Epub 2005/08/12).
Cruickshank MK, Levine MN, Hirsh J, Roberts R, Siguenza M. A standard heparin nomogram for the management of heparin therapy. Arch Intern Med. 1991;151(2):333–7 (Epub 1991/02/01).
Hirsh J, Hoak J. Management of deep vein thrombosis and pulmonary embolism. A statement for healthcare professionals. Council on Thrombosis (in consultation with the Council on Cardiovascular Radiology), American Heart Association. Circulation. 1996;93(12):2212–45 (Epub 1996/06/15).
Heidbuchel H, Verhamme P, Alings M, Antz M, Hacke W, Oldgren J, et al. European Heart Rhythm Association Practical Guide on the use of new oral anticoagulants in patients with non-valvular atrial fibrillation. Europace. 2013;15(5):625–51.
Douketis JD, Spyropoulos AC, Spencer FA, Mayr M, Jaffer AK, Eckman MH, et al. Perioperative management of antithrombotic therapy: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):e326S–50S (Epub 2012/02/15).
Michota F. Transitions of care in anticoagulated patients. J Multidiscip Healthc. 2013;6:215–28 (Epub 2013/07/03).
Misky GJ, Carlson T, Thompson E, Trujillo T, Nordenholz K. Implementation of an acute venous thromboembolism clinical pathway reduces healthcare utilization and mitigates health disparities. J Hosp Med. 2014;9(7):430–5.
Hellerslia V, Mehta P. Transition of Anticoagulants 2014. Thomas Land; 2014 [cited 2014 Oct 7]; Wall chart of transition strategies. Available from: http://www.thomasland.com/AnticoagTransitions_2014.pdf.
GlaxoSmithKline. Argatroban prescribing information. Research Triangle Park: GlaxoSmithKline; 2014.
Laboratories P. Heparin sodium prescribing information. New York: Pfizer Labs, Division of Pfizer Inc; 2013.
Squibb B-M. Coumadin prescribing information. Princeton: Bristol-Myers Squibb; 2011.
Acknowledgments
This work was supported by Boehringer Ingelheim Pharmaceuticals, Inc. (BIPI), Ridgefield, CT, USA, who funded article processing and open access charges for this study. Writing, editorial support, and/or formatting assistance was provided by José L. Walewski, PhD of Envision Scientific, which was contracted, and compensated by BIPI for these services.
The author meets criteria for authorship as recommended by the International Committee of Medical Journal Editors (ICMJE) for authorship for this manuscript, and takes responsibility for the integrity of the work as a whole, and has given final approval to the version to be published. The author takes responsibility for all content and editorial decisions, and was involved at all stages of manuscript development. The author received no compensation related to the development of the manuscript.
Disclosures
J. D. Lenchus has nothing to disclose.
Compliance with ethics guidelines
This article is based on previously conducted studies, and does not involve any new studies of human or animal subjects performed by the author.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Lenchus, J.D. Transitions in the Prophylaxis, Treatment and Care of Patients with Venous Thromboembolism. Adv Ther 33, 29–45 (2016). https://doi.org/10.1007/s12325-015-0271-8
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-015-0271-8