
Abstract
Trans-cranial magnetic stimulation (TMS) can noninvasively modulate specific brain regions to dissipate symptoms in treatment-resistant schizophrenia (TRS). Citing impaired resting state connectivity between cerebellum and prefrontal cortex in schizophrenia, we aimed to study the effect of intermittent theta burst stimulation (iTBS) targeting midline cerebellum in TRS subjects on a randomized rater blinded placebo control study design. In this study, 36 patients were randomly allocated (using block randomization method) to active and sham iTBS groups. They were scheduled to receive ten iTBS sessions, two per day (total of 1200 pulses) for 5 days in a week. The Positive and Negative Syndrome Scale (PANSS), Brief Psychiatric Rating Scale (BPRS), Schizophrenia Cognition Rating Scale (SCoRS), Simpson-Angus Extrapyramidal Side Effects Scale (SAS), and Clinical Global Impression (CGI) were assessed at baseline, after last session, and at 2 weeks post-rTMS. Thirty patients (16 and 14 in active and sham groups) completed the study. Intention to treat analysis (ITT) using mixed (growth curve) model analysis was conducted. No significant group (active vs sham) × time (pretreatment–end of 10th session–end of 2 weeks post iTBS) interaction was found for any of the variable. No major side effects were reported. Our study fails to show a significant effect of intensive cerebellar iTBS (iCiTBS) on schizophrenia psychopathology, cognitive functions, and global improvement, compared with sham stimulation, in treatment resistant cases. However, we conclude that it is safe and well tolerated. Trials using better localization technique with large sample, longer duration, and better dosing protocols are needed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Treatment-resistant schizophrenia (TRS) is defined as refractoriness of the symptoms to more than one adequate trial of antipsychotic [1]. Around 1/3rd of schizophrenia probands suffer from TRS [2, 3]. There is multitude of available therapeutic options including clozapine for TRS [4]. But nearly 60% of TRS probands do not respond to the available therapeutic options, warranting need for developing novel ones [4,5,6]. In line with the recent evidence of electroconvulsive therapy (ECT) response in refractory schizophrenia, another noninvasive brain stimulation method, i.e., trans-cranial magnetic stimulation (TMS) which modulates specific brain regions, can be a novel and safe therapeutic option in TRS [7]. Moreover, TMS has shown promise in other refractory neuropsychiatric diseases such as depression [8].
Repetitive TMS (rTMS) has shown promise in the management of refractory auditory hallucinations (AH) and persistent negative symptoms in schizophrenia [9, 10]. However, evidence-based guidelines suggest, at best, ‘possible efficacy’ and ‘level C’ recommendation for the treatment of both auditory hallucinations and negative symptoms including their refractory phenotype [11, 12]. Majority of the studies have either used conventional protocols or investigated sites like dorso-lateral prefrontal cortex (DLPFC) (for negative symptoms) and temporoparietal cortex (TPC) (for AH) [12, 13]. Importantly, schizophrenia is extremely heterogeneous and has complex multi-factorial etiopathogenesis involving multiple brain areas and neurotransmitter systems [14]. Therefore, there is need to investigate alternate sites like cerebellum for stimulation in TRS [15, 16].
Cerebellar impairment in schizophrenia has been implied owing to cognitive and affective deficits congruous with the cerebellar cognitive affective syndrome [17]. Consistent with the cognitive dysmetria and neo-Bleulerian disconnection paradigm frameworks, schizophrenia probands have displayed cerebellar gray matter reduction and altered cerebellar-thalamo-cortical functional connectivity [18,19,20,21]. As per preliminary evidence, neuromodulation of the cerebellar vermal activity (or cerebellar node) in schizophrenia probands has shown to improve negative, affective, and cognitive symptoms [22,23,24,25,26]. Also, the sole small size open label study of cerebellar theta burst stimulation (TBS) in TRS has shown safety and preliminary benefits in affective and cognitive symptoms [27]. Moreover, intermittent TBS (iTBS) has shorter stimulation time (~ 3 min.), lower threshold intensity, and more long-term excitatory meta-neuroplastic effects in comparison with other TMS protocols.
With this background, we aimed to study the effect of iTBS targeting cerebellar vermis in TRS subjects on a randomized rater blinded placebo control design. The primary outcomes were scores of the Positive And Negative Syndrome Scale (PANSS). The secondary outcomes were cognition scores, overall clinical improvement, and iTBS effects on drug-induced extra-pyramidal symptoms.
Methodology
Subjects
Patients meeting the diagnostic criteria for schizophrenia (using the Diagnostic Criteria for Research (DCR) of International Classification of Diseases – tenth edition (ICD-10)) were approached [28]. A signed informed consent was obtained prior to inclusion. Schizophrenia probands having treatment resistance were selected as per Modified Kane criteria, i.e., two or more prior drug trials of 4- to 6-week duration at 400 to 600 mg of chlorpromazine (or equivalent) with no clinical improvement, 5 years with no period of good social or occupational functioning, BPRS total score > 45 (on 18-item scale), and item score > 4 (moderate) on at least two of four positive symptoms [29]. Exclusion criteria included a prior history of an unprovoked seizure, patients receiving electroconvulsive therapy (ECT) in last 6 months, significant neurological illness or head trauma, significant unstable medical condition like uncontrolled hypertension, complicated diabetes mellitus, organ failures etc. Patients with left-handedness and current substance use disorders (SUDs) except nicotine and caffeine were also excluded. Age range was 18–59. This investigation is the lead paper of the trial (ISRCTN registry number: ISRCTN49569866). A total of 65 patients were screened between 15/5/2019 and 15/5/2020. A total of 36 patients were enrolled. All patients were inpatients and underwent regular physical examination, routine laboratory studies, and ECG (electrocardiography). Patients were required to remain on their psychotropic medication at same dosages for the entire duration of the trial. None of the patients were being provided any kind of individual psychotherapy. The study protocol was approved by the institute ethics committee (SGRR/IEC/1/19; IEC Registration No. ECR/710/Inst/UK/2015/RR-18). Patients were randomly allocated (using block randomization method) to rTMS and sham groups. The decision to enroll a patient was always made prior to randomization. In our previous study [24], the effect size (partial eta squared value) for the efficacy of cerebellar TMS in PANSS total score was 0.10 (which converts to a Cohen’s d value of 0.67 and f value of 0.34). With effect size ‘f’ of 0.34, number of groups as 2, number of measurements as 3, alpha error of 0.05, a power of 0.95, and estimated 25% of drop out cases, the total priori sample size determined was 40 (20 subjects in ‘active’ and 20 subjects in ‘sham’ group). Expected sample size of 40 could not be recruited due to COVID-19 restrictions.
Out of the 36 patients who were enrolled, 6 patients were not included in the final analysis (1: overnight aggression directed towards family members; 1: lack of improvement on 3rd day; 4: did not follow up); none of the 6 patients dropped out due to adverse effects of rTMS. Only 30 patients (16 in ‘active’ group; 14 in ‘sham’ group) completed the study (see Fig. 1).

Flow diagram showing participants’ recruitment. TBS: theta burst stimulation
rTMS Stimulation Parameters
A MagVenture-MagPro-R30 device with theta burst and B65 coils (figure-of-8-shaped coil) was utilized for the delivery of rTMS. The vermal part of the cerebellum was the preferred stimulation site. The standardized international 10–20 EEG system was used for positioning the TMS coil as it accounts for variability in participant skull size and is consistently used in clinical TMS applications [30]. The coil was centered over midline cerebellum, i.e., 1 cm below the inion (Iz, 10–20 international system) [24, 31]. Reason to choose vermal cerebellum was the evidence of disconnectivity between the midline cerebellum and DLPFC and its correlation with the psychopathology in schizophrenia [24,25,26].
Both groups received a total of ten iTBS sessions using an intensive protocol (i.e. two sessions per day at least half an hour apart for 5 days in a week). In ‘active’ group iTBS, protocol consisting of 3 pulses at 50 Hz repeated at rate of 5 Hz, 20 trains of 10 burst given with 8 s interval, with a total number of 600 pulses was delivered per session. A total of 1200 pulses were delivered per day. The iTBS was specifically chosen due to its excitatory metaplastic effects which could reverse the attenuated cerebellar disconnectivity. These metaplastic effects may lead to changes on longer time scale (hours-to-weeks) [32].We delivered 1200 pulses per day rather than conventional 600 pulses per day as recommended by Huang and colleagues [33]. Safety of 1200 pulses per day to cerebellum has been demonstrated by previous trials [27].
We gave iTBS at 80% resting motor threshold (RMT) as stimulus intensity is important in determining plasticity [33]. RMT was ascertained prior to each stimulation session. RMT was based on Rossini-Rothwell algorithm defined as lowest intensity, which produced five MEP responses of at least 50 mV in ten trials [24, 34].
Sham rTMS stimulation was carried out by B-65 sham coil that has both sound and scalp contact similar to those experienced during active stimulation. Similar figure-of-8-shaped coil as active and sham coils has been used by previous studies [27, 35].
Clinical Measures
In this study, psychopathology (positive, negative, and general) was assessed by using the Positive and Negative Syndrome Scale (PANSS) and Brief Psychiatric Rating Scale (BPRS). The PANSS has a total of 30 items that are divided into three subscales—positive (7 items), negative (7 items), and general psychopathology (16 items); each item scored on a 7-point-Likert scale, where 1 indicates absence of symptom and 7 indicates extremely severe symptom; range for PANSS scores is 30–210 [36]. BPRS is a comprehensive 18-item scale, assessing psychotic and mood symptoms relevant to schizophrenia, with scoring similar to the PANSS; range for BPRS scores is 18–126 [37]. The cognitive profile was assessed by interview-based Schizophrenia Cognition Rating Scale (SCoRS). SCoRS is a 20-item tool that assesses 8 cognitive domains—attention, memory, working memory, language, reasoning, problem solving, motor skills and social cognition, and the degree to which deficits in these domains impair daily functioning; each item is rated on a 4-point-Likert scale ranging from no impairment to severe impairment [38]. Extrapyramidal side effects were assessed using the Simpson-Angus Extrapyramidal Side Effects Scale (SAS), a 10-item scale that rates extrapyramidal side effects (i.e., gait, tremors, rigidity) on a scale of 0 to 4 [39]. Overall illness severity was assessed on the Clinical Global Impression (CGI), which has three items—severity, efficacy, and improvement that are rated on a 7-point (1–7)-Likert scale [40].
Blinding Procedure
Subjects were rated at baseline, after 10th session and at 3rd week, i.e., 2 weeks post-TBS on clinical measures by an independent rater who was blind to randomization of TBS groups into active and sham. The patients were sequentially and randomly assigned to the two groups using blocks of random-number sequences. The numbers were written in sealed opaque envelopes. For each patient, the envelope was opened immediately before commencement of the first session by the clinician administering the TBS. The patients were also blind to the arm of treatment (assessment of which was made by asking each participant to guess whether he or she is receiving active stimulation). Retrospectively, the rater was made to guess the treatment arm for the study participants based on their pre- and post-PANSS total scores. The guess matrix [41] resulted in a Cohen’s kappa coefficient of − 0.016, which implied ‘no agreement’ and therefore indicating good integrity of the rater blinding. Integrity of participant blinding to treatment arms could not be ascertained.
Statistical Analysis
Study data were analyzed using SPSS (Version 22). The primary outcome variables were positive syndrome (PANSS-PS), negative syndrome (PANSS-NS), general psychopathology PANSS-GP), and total scores on PANSS. Secondary outcome measures were BPRS, SCoRS, SAS, and CGI scores. The assumption of normality was verified by normal probability plots and the Shapiro-Wilk test. As there were four variables for the assessment of primary outcome, the Bonferroni correction for multiple comparisons was applied and p value of less than 0.05/4, i.e., 0.0125 was considered as statistically significant for analyses involving the PANSS scores; otherwise, p values < 0.05 were considered significant.
Group differences for sample characteristics were examined with independent t test and Chi-square test (wherever applicable). An intention-to-treat (ITT) analysis was conducted to include all the patients recruited in the study, irrespective of whether they completed the study period or not. The missing values were replaced using the last observation carried forward (LOCF) method. The main analysis was the interaction effect of treatment over time (across the three time points—baseline, completion of the 10th iTBS session, i.e., 7th day and 2 weeks post-iTBS, i.e., 21st day) and group (between ‘active’ and sham groups) in the double-blind phase. Overall effect of treatment over time for the two groups was analyzed using the restricted maximum likelihood (ReML) mixed (growth curve) model analysis with allocation order as ‘subjects’, treatment (active/sham) as the between-subject factor, and time (pre-treatment, completion of 10th TBS session, end of 2 weeks post-rTMS) as the within-subject factor. A supplementary per protocol (PP) analysis including subjects who have completed the study was also conducted.
Results
Sample Characteristics
The two groups were comparable in terms of gender, marital status, religion, habitat, socioeconomic status, employment status, and education. Both ‘active’ and ‘sham’ group subjects had comparable proportion of medical morbidity (X2 (1, 34) = .066, p = 1.00), schizophrenia subtype (paranoid vs. non-paranoid) (X2 (1, 34) = 1.092, p = .391), and first episode (as index episode) (X2 (1, 34) = .253, p = 1.00). Subjects randomized to ‘active’ and ‘sham’ groups were comparable on age (t (34) = .834, p = 0.410), duration of illness (t (34) = 1.466, p = 0.152), RMT (t (34) = .013, p = 0.990), and antipsychotic dose per trial (chlorpromazine equivalent dose calculated as per Woods [42] and Bazire [43]) as well (see Table 1).
Safety and Side Effects
No major side effects were reported with iTBS. Seven patients (five from ‘active’ and two from ‘sham’) reported headache during first few sessions that responded to analgesics. None of the patients reportedly discontinued due to side effects.
Outcome Measures
At the baseline, PANSS-PS (t = 1.150; p = 0.140), PANSS-NS (t = .728; p = .472), PANSS-GS (t = .318; p = .752), PANSS-total (t = .891; p = .379), BPRS (t = .144; p = 0.887), SAS (t = .421; p = 0.676), CGI (t = 1.072; p = 0.291), and SCoRS (all three sub scores) were comparable for both ‘active’ and ‘sham’ group. Table 2 shows effect of time × group comparison of pre-post effects from pretreatment phase, end of 10th session to end of 2 weeks post-iTBS across the two groups on the ITT analysis.
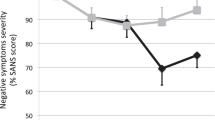
The ITT analysis using the mixed model analysis showed no significant group × time effect for any of the variables. With time (pre-treatment/after 10th session/2 weeks post-rTMS Treatment) as the within-subject factor, the treatments showed significant effect on PANSS-PS (F = 62.041, p < 0.001), PANSS-NS (F = 30.515, p < 0.001), PANSS-GS (F = 89.480, p < 0.001), PANSS-total (F = 100.029, p < 0.001), BPRS (F = 72.507, p < 0.001), SCoRS patient (F = 6.608, p = .002), SCoRS informant (F = 64.496, p < .001), SCoRS interviewer (F = 13.085, p < .001), and CGI (F = 78.770, p < 0.001) scores; the effect of treatment on SAS (F = 1.393, p = .255) scores over time was not significant. Although there was statistically significant improvement in psychopathology scores over the course of both active and sham treatments, the 2-week post-iTBS mean scores of PANSS total (viz. > 70) and BPRS (viz. > 45) imply that the improvement was not clinically significant. In the PP analysis, however, a significant time × group interaction was found for the PANSS general psychopathology scores (Supplementary Table 1).
Discussion
The current study is the first randomized controlled trial (RCT) using iTBS targeting cerebellar vermis for treating resistant schizophrenia. We find that although iTBS has shown statistically significant improvement in all psychopathology scores across 3 weeks, the benefits were not better than the placebo control.
We chose cerebellar vermal as a neuro-functional marker for excitatory iTBS due to evidence of its decreased resting-state functional connectivity with prefrontal cortex in schizophrenia [26]. More so, this reduced cerebellar-prefrontal connectivity has been suggested to be causally related to the negative symptoms and cognition in schizophrenia and is not merely an epiphenomenon [26]. Similarly, in our prior work, we have used excitatory protocols like theta range rTMS for cerebellar stimulation with significant effect on negative symptoms and gamma spectral power distribution in schizophrenia [24, 25]. TBS was chosen citing its preliminary evidence in TRS [26] and negative symptoms [44]. In this study, we chose the intensive iTBS protocol where we delivered ten sessions in 5 days (two sessions per day). This intensive iTBS protocol was pragmatically implemented in order to shorten the total treatment duration. Similar intensive and accelerated protocols have been successfully investigated in other refractory psychiatric disorders [45]. However, our study failed to show significant placebo-controlled improvement with this protocol.
However, despite employing relative stronger stimulation protocol, iTBS was well tolerated with only mild adverse effects. Transient headache was present in 23% of subjects. Prior cerebellar stimulation studies have also documented similar side effects like pain in stimulation site [46]. This has been postulated due to contraction of neck muscles during the process of stimulation. Reportedly, none of the patient in index study discontinued trial due to side effects. Therefore, safety and tolerability of TBS stimulating midline cerebellum are established in sync with prior work conducted by Demirtas-Tatlidede and colleagues [27].
In our study, we used an adequate sample of TRS subjects, random allocation, and blinded ratings in comparison with other studies [25,26,27]. While failing to conclude that adjunctive iCiTBS is better than placebo for treating treatment-resistant schizophrenia, we propose possible shortcomings of our study that might have led to this outcome. Firstly, we used figure of 8 coil and not double-cone coil. The distance of cerebellum from scalp is more than that from primary motor cortex; so, double-cone coils would be more effective for deep stimulation than figure of 8 ones [46]. Secondly, we stimulated vermis at lower intensity (80% RMT as per recommendations by Huang et al. [33]) in contrast to prior trials [24, 27]. Interestingly, Spampinato and colleagues [47] demonstrated that only Deymed double-cone coil could effectively stimulate the cerebellum at lower intensities. Thirdly, we delivered 1200 pulses per day. Other trials, such as the one by Zhao and colleagues [44], which have successfully employed TBS in schizophrenia, have delivered higher dose of stimulation, i.e., 2400 pulses per day. Presumably, the parameters we chose may not have been sufficient to induce discernible changes in schizophrenia symptom domains.
In addition to the above-mentioned limitations, future studies should consider trials with longer follow-up or accelerated TMS protocols to establish efficacy. The priori sample size estimation did not include the effects of multiple comparisons, which might have led to underestimation of sample size. And therefore, due to this relatively smaller sample size, generalizability of the findings is limited. Lack of assessment of drug compliance is another important limitation. There is lack of experimental studies investigating the effect of TBS in this novel site and its mechanism which might limit the generalization of the inferences. The use of neuronavigation to target a specific cortical site rather than scalp-based localization technique can be improved upon. Moreover, biophysical models to counter optimal angle of stimulation may be used to personalize TMS delivery as suggested in other psychiatric conditions like OCD [48]. This being the first RCT of iTBS over midline cerebellum is the strength of the study.
Conclusion
Our trial concludes that although safe and well tolerated, intensive cerebellar iTBS (iCiTBS) shows no significant difference in the change in schizophrenia psychopathology, compared with the placebo/sham control in treatment resistant cases. Trials using neuro-navigation-based localization technique with large sample, longer duration, and better dosing protocols may be needed.
References
Howes OD, McCutcheon R, Agid O, de Bartolomeis A, van Beveren NJ, Birnbaum ML, et al. Treatment-resistant schizophrenia: treatment response and resistance in psychosis (TRRIP) Working Group Consensus Guidelines on Diagnosis and Terminology. Am J Psychiatry. 2017;174(3):216–29. https://doi.org/10.1176/appi.ajp.2016.16050503.
Demjaha A, Lappin JM, Stahl D, Patel MX, MacCabe JH, et al. Antipsychotic treatment resistance in first-episode psychosis: prevalence, subtypes and predictors. Psychol Med. 2017;47(11):1981–9. https://doi.org/10.1017/S0033291717000435.
Lally J, Gaughran F, Timms P, Curran SR. Treatment-resistant schizophrenia: current insights on the pharmacogenomics of antipsychotics. Pharmgenomics Pers Med. 2016;9:117–29. https://doi.org/10.2147/PGPM.S115741.
Kane JM, Agid O, Baldwin ML, Howes O, Lindenmayer JP, Marder S, et al. Clinical guidance on the identification and management of treatment-resistant schizophrenia. J Clin Psychiatry. 2019;80(2):18com12123. https://doi.org/10.4088/JCP.18com12123.
Siskind D, Siskind V, Kisely S, et al. Can J Psychiatry. 2017;62(11):772–7. https://doi.org/10.1177/0706743717718167.
Potkin SG, Kane JM, Correll CU, Lindenmayer JP, Agid O, Marder SR, et al. The neurobiology of treatment-resistant schizophrenia: paths to antipsychotic resistance and a roadmap for future research. NPJ Schizophr. 2020;6(1):1. https://doi.org/10.1038/s41537-019-0090-z.
Wang G, Zheng W, Li XB, Wang SB, Cai DB, Yang XH, et al. ECT augmentation of clozapine for clozapine-resistant schizophrenia: a meta-analysis of randomized controlled trials. J Psychiatr Res. 2018;105:23–32. https://doi.org/10.1016/j.jpsychires.2018.08.002.
Conelea CA, Philip NS, Yip AG, Barnes JL, Niedzwiecki MJ, Greenberg BD, et al. Transcranial magnetic stimulation for treatment-resistant depression: naturalistic treatment outcomes for younger versus older patients. J Affect Disord. 2017;217:42–7. https://doi.org/10.1016/j.jad.2017.03.063.
Wagner E, Honer WG, Sommer IE, Koops S, Blumberger DM, Daskalakis ZJ, et al. Repetitive transcranial magnetic stimulation (rTMS) for schizophrenia patients treated with clozapine. World J Biol Psychiatry. 2020;13:1–13. https://doi.org/10.1080/15622975.2020.1733080.
Hovington CL, McGirr A, Lepage M, Berlim MT. Repetitive transcranial magnetic stimulation (rTMS) for treating major depression and schizophrenia: a systematic review of recent meta-analyses. Ann Med. 2013;45(4):308–21. https://doi.org/10.3109/07853890.2013.783993.
Wagner E, Löhrs L, Siskind D, Honer WG, Falkai P, Hasan A. Clozapine augmentation strategies - a systematic meta-review of available evidence. Treatment options for clozapine resistance. J Psychopharmacol. 2019;33(4):423–35. https://doi.org/10.1177/0269881118822171.
Lefaucheur JP, Aleman A, Baeken C, Benninger DH, Brunelin J, Di Lazzaro V, et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): an update (2014-2018). Clin Neurophysiol. 2020;131(2):474–528. https://doi.org/10.1016/j.clinph.2019.11.002 Erratum in: Clin Neurophysiol 2020;131(5):1168–1169.
Koops S, van Dellen E, Schutte MJ, Nieuwdorp W, Neggers SF, Sommer IE. Theta burst transcranial magnetic stimulation for auditory verbal hallucinations: negative findings from a double-blind-randomized trial. Schizophr Bull. 2016;42(1):250–7. https://doi.org/10.1093/schbul/sbv100.
Owen MJ, Sawa A, Mortensen PB. Schizophrenia. Lancet. 2016;388(10039):86–97. https://doi.org/10.1016/S0140-6736(15)01121-6.
Stanford AD, Sharif Z, Corcoran C, Urban N, Malaspina D, Lisanby SH. rTMS strategies for the study and treatment of schizophrenia: a review. Int J Neuropsychopharmacol. 2008;11(4):563–76. https://doi.org/10.1017/S1461145707008309.
Freitas C, Fregni F, Pascual-Leone A. Meta-analysis of the effects of repetitive transcranial magnetic stimulation (rTMS) on negative and positive symptoms in schizophrenia. Schizophr Res. 2009;108(1–3):11–24. https://doi.org/10.1016/j.schres.2008.11.027.
Schmahmann JD. The cerebellum and cognition. Neurosci Lett. 2019;688:62–75. https://doi.org/10.1016/j.neulet.2018.07.005.
Bernard JA, Mittal VA. Dysfunctional activation of the cerebellum in schizophrenia: a functional neuroimaging meta-analysis. Clin Psychol Sci. 2015;3(4):545–66. https://doi.org/10.1177/2167702614542463.
Cao H, Chén OY, Chung Y, Forsyth JK, McEwen SC, Gee DG, et al. Cerebello-thalamo-cortical hyperconnectivity as a state-independent functional neural signature for psychosis prediction and characterization. Nat Commun. 2018;9(1):3836. https://doi.org/10.1038/s41467-018-06350-7.
He H, Luo C, Luo Y, Duan M, Yi Q, Biswal BB, et al. Reduction in gray matter of cerebellum in schizophrenia and its influence on static and dynamic connectivity. Hum Brain Mapp. 2019;40(2):517–28. https://doi.org/10.1002/hbm.24391.
Escelsior A, Belvederi Murri M, Calcagno P, Cervetti A, Caruso R, Croce E, et al. Effectiveness of cerebellar circuitry modulation in schizophrenia: a systematic review. J Nerv Ment Dis. 2019;207(11):977–86. https://doi.org/10.1097/NMD.0000000000001064.
Garg S, Tikka SK, Goyal N, Sinha VK, Nizamie SH. Amelioration of anergia and thought disorder with adjunctive high frequency cerebellar vermal repetitive transcranial magnetic stimulation in schizophrenia: a case report. Schizophr Res. 2013a;143(1):225–7. https://doi.org/10.1016/j.schres.2012.10.022.
Garg S, Goyal N, Tikka SK, Sinha VK. Exacerbation of auditory verbal hallucinations with adjunctive high-frequency cerebellar vermal repetitive transcranial magnetic stimulation in schizophrenia: a case report. J ECT. 2013b;29(1):65–6. https://doi.org/10.1097/YCT.0b013e3182706aa1.
Garg S, Sinha VK, Tikka SK, Mishra P, Goyal N. The efficacy of cerebellar vermal deep high frequency (theta range) repetitive transcranial magnetic stimulation (rTMS) in schizophrenia: a randomized rater blind-sham controlled study. Psychiatry Res. 2016;243:413–20. https://doi.org/10.1016/j.psychres.2016.07.023.
Tikka SK, Garg S, Sinha VK, Nizamie SH, Goyal N. Resting state dense array gamma oscillatory activity as a response marker for cerebellar-repetitive transcranial magnetic stimulation (rTMS) in schizophrenia. J ECT. 2015;31(4):258–62. https://doi.org/10.1097/YCT.0000000000000242.
Brady RO Jr, Gonsalvez I, Lee I, Öngür D, Seidman LJ, Schmahmann JD, et al. Cerebellar-prefrontal network connectivity and negative symptoms in schizophrenia. Am J Psychiatry. 2019;176(7):512–20. https://doi.org/10.1176/appi.ajp.2018.18040429.
Demirtas-Tatlidede A, Freitas C, Cromer JR, Safar L, Ongur D, Stone WS, et al. Safety and proof of principle study of cerebellar vermal theta burst stimulation in refractory schizophrenia. Schizophr Res. 2010;124(1–3):91–100. https://doi.org/10.1016/j.schres.2010.08.015.
World Health Organization. The ICD-10 classification of mental and behavioral disorders: diagnostic criteria for research. Geneva: WHO; 1992.
Conley RR, Kelly DL. Management of treatment resistance in schizophrenia. Biol Psychiatry. 2001;50(11):898–911. https://doi.org/10.1016/s0006-3223(01)01271-9.
Hanlon CA, Dowdle LT, Correia B, Mithoefer O, Kearney-Ramos T, Lench D, et al. Left frontal pole theta burst stimulation decreases orbitofrontal and insula activity in cocaine users and alcohol users. Drug Alcohol Depend. 2017;178:310–7. https://doi.org/10.1016/j.drugalcdep.2017.03.039.
Schutter DJ, van Honk J, d'Alfonso AA, Peper JS, Panksepp J. High frequency repetitive transcranial magnetic over the medial cerebellum induces a shift in the prefrontal electroencephalography gamma spectrum: a pilot study in humans. Neurosci Lett. 2003;336(2):73–6. https://doi.org/10.1016/s0304-3940(02)01077-7.
Doeltgen SH, Ridding MC. Modulation of cortical motor networks following primed theta burst transcranial magnetic stimulation. Exp Brain Res. 2011;215:199–206. https://doi.org/10.1007/s00221-011-2886-6.
Huang YZ, Edwards MJ, Rounis E, Bhatia KP, Rothwell JC. Theta burst stimulation of the human motor cortex. Neuron. 2005;45:201–6. https://doi.org/10.1016/j.neuron.2004.12.033.
Rothwell JC, Hallett M, Berardelli A, Eisen A, Rossini P, Paulus W. Magnetic stimulation: motor evoked potentials. The International Federation of Clinical Neurophysiology. Electroencephalogr Clin Neurophysiol Suppl. 1999;52:97–103.
Bologna M, Di Biasio F, Conte A, Iezzi E, Modugno N, Berardelli A. Effects of cerebellar continuous theta burst stimulation on resting tremor in Parkinson's disease. Parkinsonism Relat Disord. 2015;21(9):1061–6. https://doi.org/10.1016/j.parkreldis.2015.06.015.
Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13(2):261–76. https://doi.org/10.1093/schbul/13.2.261.
Overall JE, Gorham DR. The brief psychiatric rating scale. Psychol Rep. 1962;10:799–812.
Keefe RS, Poe M, Walker TM, Kang JW, Harvey PD. The Schizophrenia Cognition Rating Scale: an interview-based assessment and its relationship to cognition, real-world functioning, and functional capacity. Am J Psychiatry. 2006;163(3):426–32. https://doi.org/10.1176/appi.ajp.163.3.426.
Simpson GM, Angus JW. A rating scale for extrapyramidal side effects. Acta Psychiatr Scand Suppl. 1970;212:11–9. https://doi.org/10.1111/j.1600-0447.1970.tb02066.x.
Guy W. ECDEU assessment manual for psychopharmacology. National Institute of Mental Health; 1976.
Waite JC. Assessing Blinding in Randomized Clinical Trials. [Thesis on the internet]. Pomana: California State Polytechnic University; 2017. Available at http://dspace.calstate.edu/bitstream/handle/10211.3/196699/WaiteJesse_Thesis2017.pdf?sequence=6. Assessed 01 July 2020.
Woods SW. Chlorpromazine equivalent doses for the newer atypical antipsychotics. J Clin Psychiatry. 2003;64(6):663–7. https://doi.org/10.4088/jcp.v64n0607.
Bazire S. Psychotropic drug directory. Health Comm UK Limited.
Zhao S, Kong J, Li S, Tong Z, Yang C, Zhong H. Randomized controlled trial of four protocols of repetitive transcranial magnetic stimulation for treating the negative symptoms of schizophrenia. Shanghai Arch Psychiatry. 2014;26(1):15–21. https://doi.org/10.3969/j.issn.1002-0829.2014.01.003.
Sonmez AI, Camsari DD, Nandakumar AL, Voort JLV, Kung S, Lewis CP, et al. Accelerated TMS for depression: a systematic review and meta-analysis. Psychiatry Res. 2019;273:770–81. https://doi.org/10.1016/j.psychres.2018.12.041.
Demirtas-Tatlidede A, Freitas C, Pascual-Leone A, Schmahmann JD. Modulatory effects of theta burst stimulation on cerebellar nonsomatic functions. Cerebellum. 2011;10(3):495–503. https://doi.org/10.1007/s12311-010-0230-5.
Spampinato D, Ibáñez J, Spanoudakis M, Hammond P, Rothwell JC. Cerebellar transcranial magnetic stimulation: the role of coil type from distinct manufacturers. Brain Stimul. 2020;13(1):153–6. https://doi.org/10.1016/j.brs.2019.09.005.
Cocchi L, Zalesky A, Nott Z, Whybird G, Fitzgerald PB, Breakspear M. Transcranial magnetic stimulation in obsessive-compulsive disorder: a focus on network mechanisms and state dependence. Neuroimage Clin. 2018;19:661–74. https://doi.org/10.1016/j.nicl.2018.05.029.
Funding
• No funding received in any respect.
The corresponding author has full access to all the data in the study and has the final responsibility for the decision to submit for publication.
Author information
Authors and Affiliations
Contributions
• PC wrote the protocol and collected the data and helped with interpretation of findings and development of the manuscript.
• PC, SG, and SK conceptualized the study hypotheses and the design.
• SG and SKT conducted statistical analysis and interpreted the results.
• PC and SG wrote the manuscript.
• SKT and SK were involved in the critical evaluation of the literature.
• All authors have approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Work carried out at: Shri Guru Ram Rai Institute of Medical and Health Sciences, 248001, Uttarakhand, India
Electronic supplementary material
ESM 1
(DOCX 17 kb)
Rights and permissions
About this article

Cite this article
Chauhan, P., Garg, S., Tikka, S.K. et al. Efficacy of Intensive Cerebellar Intermittent Theta Burst Stimulation (iCiTBS) in Treatment-Resistant Schizophrenia: a Randomized Placebo-Controlled Study. Cerebellum 20, 116–123 (2021). https://doi.org/10.1007/s12311-020-01193-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12311-020-01193-9