
Abstract
The aims of the present systematic review were to: (1) assess the role of 18F-fluorocholine (FCH) positron emission tomography (PET) with computed tomography (CT) and PET with magnetic resonance imaging (MRI) in patients with biochemically known hyperparathyroidism; (2) compare the diagnostic performance of FCH PET/CT or PET/MRI with conventional morphological and functional imaging. A literature search until December 2019 was performed in the PubMed, Scopus and Web of Science databases, using the terms “choline” AND “PET” AND “hyperparathyroidism”. The search was conducted with and without the addition of filters (e.g., language: English only; type of article: original article; subjects: humans only) and selecting only articles published in the last 5 years. Twenty-three articles and 1112 patients were considered. Different FCH PET/CT acquisition protocols were adopted across the studies, using dynamic, early or delayed scans. FCH PET/CT proved more accurate than ultrasonography (US) or 99mTc-sestamibi single-photon emission tomography (SPET). PET/MRI also seemed to be more accurate than MRI alone in detecting benign parathyroid lesions. FCH PET/CT is more accurate than conventional morphological and functional imaging modalities (US or SPET) for the detection of benign parathyroid lesions. It could, therefore, be a reliable tool in both primary and recurrent hyperparathyroidism.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Primary hyperparathyroidism (PHPT) is a rather common endocrinological disorder, the third most common endocrine disease after diabetes mellitus and thyroid disorders. It is characterized by one or more hyperfunctioning parathyroid glands [1], due to parathyroid adenoma (in > 80% of cases), multiple adenomas, parathyroid hyperplasia (about 15%) or parathyroid carcinoma (less than 1%) [2], [3]. People with mild PHPT are at increased risk of various comorbidities, such as nephrolithiasis, osteoporosis and fragility fractures. Surgical excision is usually a definitive treatment, though repeat surgery may be required in cases of recurrent or persistent hyperparathyroidism (fewer than 5% of patients) [4].
PHPT may also be associated with a higher risk of cardiovascular disease and mortality [5, 6]. The related mortality risk seems to be lower in patients who undergo surgery than in those treated conservatively [6]. A recent cost-effectiveness analysis on patients with non-localized PHPT showed that use of advanced imaging methods is more cost-effective than routine bilateral neck exploration [6]. Based on this evidence, it becomes essential to employ appropriate methods capable of revealing which parathyroid glands are causing PHPT. This is also important to avoid unnecessary surgery and to identify ectopic parathyroid glands.
Benign parathyroid lesions can be identified and located using morphological or functional imaging. Neck ultrasonography (US), computed tomography (CT) and magnetic resonance imaging (MRI) have been extensively used in this setting. Dual-tracer subtraction, mainly using 99mTc-sestamibi (MIBI)/99mTc-pertechnetate scans, and/or dual-phase scintigraphy with planar acquisitions, have been widely employed in cases of hyperparathyroidism, frequently combined with US. For diagnostic purposes, single-photon emission tomography (SPET)/CT has proved the best imaging modality for identifying the site of hyperfunctioning parathyroid glands, better than either SPET alone or planar scintigraphy. That said, even SPET/CT fails to identify the gland in up 30% of cases [7].
When a combination of US and SPET/CT fails, a more effective imaging technique is needed. Radiolabeled choline PET/CT has been widely used in patients with recurrent prostate cancer [8], and it was in this context that a study published in 2013 reported incidentally detecting an 18F-fluorocholine (FCH) hotspot in a patient’s neck, which turned out to be a parathyroid adenoma [9]. In the ensuing 6 years, a number of published studies reported on the role of FCH PET/CT in identifying benign parathyroid lesions.
The aims of the present systematic review are to: (1) assess the role of FCH PET/CT and PET/MRI in patients with known PHPT; and (2) compare the diagnostic performance of FCH PET/CT or PET/MRI with other morphological and/or functional imaging modalities.
Materials and methods
Search strategy and study selection
A literature search until December 2019 was performed in the PubMed, Scopus and Web of Science databases. The terms used were: “choline” AND “PET” AND “hyperparathyroidism”. The search was run with and without the addition of filters, such as language (English only), type of article (original article), subjects (humans only), and only considering articles published in the last 5 years. Two reviewers (I.R., F.M.) conducted the literature search, and two independent physicians (L.E., D.C.) selected studies for inclusion, and data extraction. Any discrepancy was resolved by consensus. Independently identified records were combined, then the full texts were retrieved and examined by three reviewers (I.R., F.M., L.E.). The reference lists of the selected studies were carefully checked to identify any additional relevant literature.
A systematic review was conducted using established methods [10], and the results are presented according to the PRISMA guidelines [11].
Only studies that met the following inclusion criteria were considered eligible for the systematic review: (a) a sample size of more than 10 patients; and (b) FCH PET/CT as the index test. Clinical reports, conference abstracts, and editors’ comments were excluded. Systematic reviews, with or without meta-analyses, were considered for the purpose of enriching the bibliographic references.
Data extraction
For each study considered, the general information retrieved included: basic data (authors, year of publication, country, and study design); population characteristics (number of patients, type of hyperparathyroidism, PTH levels); the diagnostic reference standard; and the comparison of FCH PET/CT with other imaging modalities (i.e., US, 99mTc-MIBI SPET, or SPET/CT).
Statistical analysis
Continuous variables were expressed as median (range) and categorical as number (percentage). Data about diagnostic accuracies were obtained from each study to prepare a 2 × 2 contingency table and thus calculating the pooled sensitivity, by a patient-based and lesion-based analysis. Comprehensive meta-analysis (CMA) software version 3.3.070 (Biostat, Englewood, NJ, USA) was used for the assessment of pooled diagnostic performances.
Results
The systematic literature search generated 23 articles (see Fig. 1) concerning a total of 1112 patients investigated with FCH PET/CT for the detection of benign parathyroid lesions. Most of the studies were prospective (n = 15, 65%; 488 patients). Interestingly, 67 patients underwent FCH PET/MRI. As shown in Table 1 [12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33], FCH PET/CT was compared in many cases with US or 99mTc-MIBI scanning, the main endpoint being to assess the accuracy of FCH PET/CT in detecting benign parathyroid lesions in cases of doubtful or negative conventional imaging. In all studies, histopathological examination was the diagnostic reference standard.

PRISMA flow for the selected studies
A careful analysis of the selected literature showed that a dynamic FCH PET/CT protocol was used in 4/23 studies. In particular, Michaud et al. [13] and Kluijhout et al. [14] ran a single dynamic acquisition lasting 10 min and 40 min, respectively; and Michaud et al. and Prabhu et al. [12, 15] performed a dynamic acquisition for 10-15 min followed by a static image 10 or 45 min after the injection. Static acquisitions were obtained in the other studies at a single point ranging from 10 to 60 min after the intravenous administration of FCH in 9/23 studies [4, 16, 17, 19,20,21,22,23, 34]; and twice, first after 2–60 min and then after 60–120 min, in 10/23 studies. Only Rep et al. [25] reported scanning patients 3 times, at 5, 60 and 120 min after FCH injection. The FCH dosage was fixed in 16 studies, in the range of 100-230 MBq [15, 19,20,21,22,23,24,25,26,27,28, 31,32,33,34]; it was adjusted to the patient’s body weight in 5 (1.5–3.2 MBq/kg) and not declared in two studies [12, 16, 17, 29, 30].
FCH PET/CT was compared with US by Amadou et al. [4], Bossert et al. [30], Hocevar et al. [26], Michaud et al. [13], and Thanseer et al. [32]. FCH PET/CT proved to be superior to US in detecting benign parathyroid lesions, with a sensitivity in the range of 85.2–100% and 50–82%, respectively, on patient-based and lesion-based analysis.
Comparisons between FCH PET/CT and 99mTc-MIBI SPET/CT with a dual-phase and/or subtraction protocol were reported in numerous studies (Table 2; [4, 12,13,14,15,16,17, 19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34]).
Quak et al. [17], Araz et al. [20], Kluijhout et al. [16], Hocevar et al. [26], and Thanseer et al. [32] found FCH PET/CT more sensitive than dual-phase SPET/CT (100% vs. 80.7%, and 100% vs. 76.4%, respectively, for patient-based and lesion-based analyses).
Michaud et al. [12, 13], Lezaic et al. [24], Zajickova et al. [22], Rep et al. [27], Amadou et al. [4], Beheshti et al. [29], Bossert et al. [30], Grimaldi et al. [34], and Huber et al. [19] compared FCH PET/CT with 99mTc-MIBI/99mTc-tetrofosmin SPET/CT performed with both subtraction and dual-phase protocols. They found FCH PET/CT superior to SPET/CT with the subtraction and dual-phase protocols for the detection of adenoma and/or hyperplastic parathyroid, with a diagnostic accuracy of 97.4% and 87.7% for PET/CT and SPET/CT, respectively, on lesion-based analyses.
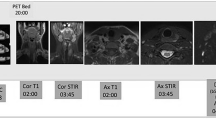
In the study by Kluijhout et al. [14], 10 patients were studied with FCH PET and MRI, and compared with the same patients examined using US and a dual-phase 99mTc-MIBI SPET/CT. While for PET/MRI the sensitivity was 90% and the positive predictive value (PPV) was 100%, MRI alone showed a sensitivity of 55.6% and a PPV of 83.3%. In Fig. 2 is reported a 65-year-old patient with persistent hyperparathyroidism after surgery who underwent FCH PET/MRI in our Department.

Example of positive 18F-FCH PET/MRI (Biograph mMR, Siemens Germany) and negative 99MTc-MIBI SPECT/CT (Infinia Hawkeye, GE Healthcare) performed at the University Hospital of Padova, Department of Medicine, Unit of Nuclear Medicine in a patient with hyperparathyroidism after left thyroidectomy (during a surgical procedure of left parathyroidectomy). MR axial Caipirinha in-phase (1) and MR axial Caipirinha out of-phase (2) demonstrating an ovoidal mass (red arrows) partially liquid at axial T2-Haste (3) with a very high posterior, paratracheal uptake of 18F-FCH PET/MR (4, red arrow). 99MTc-MIBI early after injection (5) and late after injection (6) phases of the same patient demonstrating no significant late retention of MIBI in the area revealed by 18F-FCH PET/MRI. SPET/CT of the same patient revealed only faint uptake (7: red cross) of MIBI in the paratracheal area revealed by 18F-FCH PET comparable to the background
True positive, false positive, true negative and false positive were available in 18 studies, at patient-based analysis and in 14 studies at lesion-based analysis (Table 3). Totally, true positive findings were reported in 686 patients and 530 lesions, respectively. Conversely, the number of false negative results were 35 and 23 on patient-based and lesion-based analysis. Pooled sensitivities were 93.7% and 91.3%, on patient-based and lesion-based analysis, respectively, as illustrated in Fig. 3.

Forest plots for pooled sensitivities of FCH PET/CT or PET/MRI per patient-based and lesion-based analysis
Discussion
The present systematic review showed that, in a population with negative/doubtful imaging findings, FCH PET/CT is more accurate than 99mTc-MIBI scintigraphy (whatever the protocol used) and US in patients with primary or recurrent hyperparathyroidism (all 23 studies considered in the review had included patients with primary hyperparathyroidism, and two (Amadou et al. [4] and Christakis et al. [31]) also included cases of recurrent hyperparathyroidism.
It is important to bear in mind that acquisition protocols for FCH PET/CT vary considerably. This can have an important impact on how images are interpreted and could bias their reported accuracy. FCH PET/CT was nonetheless superior to conventional scintigraphic or radiological approaches in most cases, regardless of the protocol used. In the majority of the studies considered, a single static acquisition was obtained at any time between 2 and 60 min after injecting the tracer. In 6/8 studies involving single static acquisitions, this interval ranged between 30 and 60 min. Full dynamic analysis could clarify the best timing of a static acquisition more precisely. This aspect does not seem to have been addressed in the literature to date and could be an interesting topic for future research. Only the paper by Prabhu et al. [15] reported the time active curves for parathyroid adenoma, thyroid gland and lymph node, demonstrating a higher uptake in parathyroid adenoma in the first 5 min after tracer injection. Michaud et al. [13] demonstrated that abnormal foci at a parathyroid gland were visible on early images, although the significant uptake in blood vessels imposed a more careful analysis of the cross-sectional images. Rep et al. [25] reported a slightly higher accuracy and sensitivity on scans obtained after 60 min than on those obtained after 5 min (94.1 vs. 96.5% and 90.5 vs. 93.6%, respectively). They consequently suggested that, for the preoperative localization of parathyroid gland, image acquisition was optimal 1 h after administering FCH.
Eight studies reported false positive results and 17 obtained false negative findings at 18F-Choline PET/CT (see Table 3), in accordance with the patient-based analysis. False-positive and false-negative results were frequently due to misinterpretation of thyroid anomalies, or due to a high uptake in normal or hyperplastic parathyroid glands, or in case of ectopic glands or adenomas with no specific characteristics or in case of very small adenomas with a fairly low number of oxyphilic cells.
As in the case of 99mTc-MIBI SPET/CT, some authors preferred to use a dual-phase FCH PET protocol (PET/CT or PET/MRI). It should be noted, however, that the kinetic characteristics of radiolabeled choline are very different from those of 99mTc-MIBI, and so the proper timing of the former cannot be deduced directly from the latter. 99mTc-MIBI accumulates more intensely in malignant cells because of their higher mitochondrial density and transmembrane electrical potential. Non-specific mechanisms lead to the uptake in nontumor cells with a greater metabolic activity or higher density of mitochondria—a situation encountered in atypical hyperplasia or particularly active tumor-like granulation. 99mTc-MIBI uptake in parathyroid foci was found to depend not on the cell type, but rather on either the size or the functional state of a lesion (Fukumoto et al. [35]). On the other hand, tumor cells with a high proliferation rate will have a high uptake of FCH to keep up with an increased demand for the synthesis of phospholipids (Vallabhajosula et al. [36]). A possible explanation for FCH uptake in benign parathyroid adenomas seems to be the increase in phospholipid-dependent choline kinase activity arising from PTH hypersecretion (Ishizuka et al. [37]).
A number of systematic reviews and meta-analyses on FCH PET/CT have been published in the last 2 years (Table 4) (Kim et al. [38]; Treglia et al. [39]; Boccalatte et al. [40]; Broos et al. [33]). In all cases, FCH PET/CT had an optimal performance in identifying benign parathyroid lesions. To the best of our knowledge, however, our systematic review is the first to include a large number of studies (n = 23), and to compare FCH PET/CT with conventional imaging (US and 99mTc-MIBI scanning), based on per-patient and per-lesion analyses. The present review also paid attention to the timing of image acquisition. In clinical practice, it seems that FCH PET/CT could be used for localizing and identifying benign parathyroid lesions, irrespective of the severity of PHPT (Beheshti et al. [29]), and particularly in patients with equivocal or negative conventional imaging.
CT and MRI have always had a marginal role in parathyroid imaging, and been applied mainly when the results of US and 99mTc-MIBI are difficult to interpret, or when parathyroidectomy fails due to ectopic glands (Johnson et al. [41]). Recent technical advances enabling high-resolution MRI of the neck have increased the applicability of such techniques, however. Even small lesions can be reliably detected and characterized nowadays on conventional sequences or with methods like diffusion weighted imaging (DWI) (Yildiz et al. [42]). 4DCeCT combines standard multiplanar CT scanning (non-contrast, arterial and venous phases) with the fourth dimension of changes in contrast attenuation over time, providing both functional and anatomical information about the abnormal parathyroid gland. Some recent studies have reported the role of 4DCeCT in patients with persistent or recurrent parathyroid hyperfunction, showing a sensitivity until to 86% [43,44,45,46]. Piccardo et al. [21], showed that in 31 patients, the association of 18F-Choline PET with 4DCeCT could enhance the sensitivity to 100% in patients with persistent or recurrent hyperfunctioning parathyroid.
Argiro’ et al. [47], for instance, found MRI more sensitive (97.8%) than US or 99mTc-MIBI, either alone (89.1% and 83.6%, respectively) or combined (93.4%), for the pre-surgical detection of benign parathyroid lesions, as well as for the diagnosis of multiglandular disease and ectopic parathyroid adenomas.
Yildiz et al. [48] demonstrated that DWI enables solid parathyroid lesions to be distinguished from surrounding structures, and can also detect different types of lesions with peculiar MRI characteristics on T1w and T2w sequences. They found that parathyroid adenoma and hyperplasia usually appear as small lesions with well-defined margins and contrast enhancement, while parathyroid carcinomas are larger and less homogeneous.
Finally, in a recent study, Ozturk et al. [44] correctly localized 38 parathyroid lesions using 4D MRI, reporting a sensitivity of 90.5% and a PPV of 95%.
The advantages and disadvantages of all imaging techniques that can be used in the definition of parathyroid benign lesions are listed in Table 5.
In the light of the above, an approach combining FCH PET with MRI (using PET/MRI scanners or PET/CT with MRI) represents an optimal choice, improving on the accuracy of either method. Unfortunately, the paucity of data on PET/MRI in this field prevents us from drawing any further conclusions about the diagnostic potential of this technique.
Conclusions
FCH PET is more accurate than conventional imaging modalities (US and 99mTc-MIBI SPET/CT, whatever the protocol used) in detecting benign parathyroid lesions. It has a potential role in both primary and recurrent hyperparathyroidism. Although it would be necessary to conduct a cost-effective analysis before adopting this imaging modality in clinical practice, it seems important to emphasize that, in selected cases, when the outcome of conventional US and scintigraphy is hard to interpret, FCH PET is an appropriate choice. PET/MRI is a very promising technique in this field, but further research is needed to fully assess its role.
References
Hindié E, Ugur O, Fuster D, O’Doherty M, Grassetto G, Ureña P, Kettle A, Gulec SA, Pons F, Rubello D. Parathyroid Task Group of the EANM, 2009 EANM parathyroid guidelines. Eur J Nucl Med Mol Imaging. 2009;36:1201–16. https://doi.org/10.1007/s00259-009-1131-z.
Delellis RA, Mazzaglia P, Mangray S. Primary hyperparathyroidism: a current perspective. Arch Pathol Lab Med. 2008;132:1251–62. https://doi.org/10.1043/1543-2165(2008)132%5b1251:PHACP%5d2.0.CO;2.
Carling T, Ocal IT, Udelsman R. Special variants of differentiated thyroid cancer: does it alter the extent of surgery versus well-differentiated thyroid cancer? World J Surg. 2007;31:916–23. https://doi.org/10.1007/s00268-006-0837-3.
Amadou C, Bera G, Ezziane M, Chami L, Delbot T, Rouxel A, Leban M, Herve G, Menegaux F, Leenhardt L, Kas A, Trésallet C, Ghander C, Lussey-Lepoutre C. 18F-fluorocholine PET/CT and parathyroid 4D computed tomography for primary hyperparathyroidism: the challenge of reoperative patients. World J Surg. 2019;43:1232–42. https://doi.org/10.1007/s00268-019-04910-6.
Reid LJ, Muthukrishnan B, Patel D, Seckl JR, Gibb FW. Predictors of nephrolithiasis, osteoporosis, and mortality in primary hyperparathyroidism. J Clin Endocrinol Metab. 2019;104:3692–700. https://doi.org/10.1210/jc.2018-02483.
Collier A, Ghosh S, Nowell S, Clark D. Increased mortality in patients with primary hyperparathyroidism: does surgery make a difference? Endocr Pract. 2019;25:335–9. https://doi.org/10.4158/EP-2018-0407.
Ciappuccini R, Morera J, Pascal P, Rame J-P, Heutte N, Aide N, Babin E, Reznik Y, Bardet S. Dual-phase 99mTc sestamibi scintigraphy with neck and thorax SPECT/CT in primary hyperparathyroidism: a single-institution experience. Clin Nucl Med. 2012;37:223–8. https://doi.org/10.1097/RLU.0b013e31823362e5.
Evangelista L, Zattoni F, Guttilla A, Saladini G, Zattoni F, Colletti PM, Rubello D. Choline PET or PET/CT and biochemical relapse of prostate cancer: a systematic review and meta-analysis. Clin Nucl Med. 2013;38:305–14. https://doi.org/10.1097/RLU.0b013e3182867f3c.
Quak E, Lheureux S, Reznik Y, Bardet S, Aide N. F18-choline, a novel PET tracer for parathyroid adenoma? J Clin Endocrinol Metab. 2013;98:3111–2. https://doi.org/10.1210/jc.2013-2084.
Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60. https://doi.org/10.1136/bmj.327.7414.557.
Moher D, Liberati A, Tetzlaff J, Altman DG, DPRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151:264–9. https://doi.org/10.7326/0003-4819-151-4-200908180-00135.
Michaud L, Burgess A, Huchet V, Lefèvre M, Tassart M, Ohnona J, Kerrou K, Balogova S, Talbot J-N, Périé S. Is 18F-fluorocholine-positron emission tomography/computerized tomography a new imaging tool for detecting hyperfunctioning parathyroid glands in primary or secondary hyperparathyroidism? J Clin Endocrinol Metab. 2014;99:4531–6. https://doi.org/10.1210/jc.2014-2821.
Michaud L, Balogova S, Burgess A, Ohnona J, Huchet V, Kerrou K, Lefèvre M, Tassart M, Montravers F, Périé S, Talbot J-N. A pilot comparison of 18F-fluorocholine PET/CT, ultrasonography and 123I/99mTc-sestaMIBI dual-phase dual-isotope scintigraphy in the preoperative localization of hyperfunctioning parathyroid glands in primary or secondary hyperparathyroidism: influence of. Medicine (Baltimore). 2015;94:e1701. https://doi.org/10.1097/MD.0000000000001701.
Kluijfhout WP, Pasternak JD, Gosnell JE, Shen WT, Duh Q-Y, Vriens MR, de Keizer B, Hope TA, Glastonbury CM, Pampaloni MH, Suh I. 18F fluorocholine PET/MR imaging in patients with primary hyperparathyroidism and inconclusive conventional imaging: a prospective pilot study. Radiology. 2017;284:460–7. https://doi.org/10.1148/radiol.2016160768.
Prabhu M, Kumari G, Damle NA, Arora G, Kumar P, Kumar R, Tripathi M, Bal C, Khadgawat R, Kumar C, Agarwal S. Assessment of the role of early dynamic PET/CT with 18F-fluorocholine in detection of parathyroid lesions in patients with primary hyperparathyroidism. Nucl Med Commun. 2018;39:1190–6. https://doi.org/10.1097/MNM.0000000000000924.
Kluijfhout WP, Vorselaars WMCM, van den Berk SAM, Vriens MR, Borel Rinkes IHM, Valk GD, van Dalen T, de Klerk JMH, de Keizer B. Fluorine-18 fluorocholine PET-CT localizes hyperparathyroidism in patients with inconclusive conventional imaging: a multicenter study from the Netherlands. Nucl Med Commun. 2016;37:1246–52. https://doi.org/10.1097/MNM.0000000000000595.
Quak E, Blanchard D, Houdu B, Le Roux Y, Ciappuccini R, Lireux B, de Raucourt D, Grellard J-M, Licaj I, Bardet S, Reznik Y, Clarisse B, Aide N. F18-choline PET/CT guided surgery in primary hyperparathyroidism when ultrasound and MIBI SPECT/CT are negative or inconclusive: the APACH1 study. Eur J Nucl Med Mol Imaging. 2018;45:658–66. https://doi.org/10.1007/s00259-017-3911-1.
Grimaldi S, Young J, Kamenicky P, Hartl D, Terroir M, Leboulleux S, Berdelou A, Hadoux J, Hescot S, Remy H, Baudin E, Schlumberger M, Deandreis D. Challenging pre-surgical localization of hyperfunctioning parathyroid glands in primary hyperparathyroidism: the added value of 18F-Fluorocholine PET/CT. Eur J Nucl Med Mol Imaging. 2018;45:1772–80. https://doi.org/10.1007/s00259-018-4018-z.
Huber GF, Hüllner M, Schmid C, Brunner A, Sah B, Vetter D, Kaufmann PA, von Schulthess GK. Benefit of 18F-fluorocholine PET imaging in parathyroid surgery. Eur Radiol. 2018;28:2700–7. https://doi.org/10.1007/s00330-017-5190-4.
Araz M, Soydal Ç, Özkan E, Kir MK, İbiş E, Güllü S, Erdoğan MF, Emral R, Küçük ÖN. The efficacy of fluorine-18-choline PET/CT in comparison with 99mTc-MIBI SPECT/CT in the localization of a hyperfunctioning parathyroid gland in primary hyperparathyroidism. Nucl Med Commun. 2018;39:989–94. https://doi.org/10.1097/MNM.0000000000000899.
Piccardo A, Trimboli P, Rutigliani M, Puntoni M, Foppiani L, Bacigalupo L, Crescenzi A, Bottoni G, Treglia G, Paparo F, Del Monte P, Lanata M, Paone G, Ferrarazzo G, Catrambone U, Arlandini A, Ceriani L, Cabria M, Giovanella L. Additional value of integrated 18F-choline PET/4D contrast-enhanced CT in the localization of hyperfunctioning parathyroid glands and correlation with molecular profile. Eur J Nucl Med Mol Imaging. 2019;46:766–75. https://doi.org/10.1007/s00259-018-4147-4.
Zajíčková K, Zogala D, Kubinyi J. Parathyroid imaging by (18)F-fluorocholine PET/CT in patients with primary hyperparathyroidism and inconclusive conventional methods: clinico-pathological correlations. Physiol Res. 2018;67:S551–7. https://doi.org/10.33549/physiolres.934029.
Fischli S, Suter-Widmer I, Nguyen BT, Müller W, Metzger J, Strobel K, Grünig H, Henzen C. The Significance of 18F-fluorocholine-PET/CT as localizing imaging technique in patients with primary hyperparathyroidism and negative conventional imaging. Front Endocrinol (Lausanne). 2017;8:380. https://doi.org/10.3389/fendo.2017.00380.
Lezaic L, Rep S, Sever MJ, Kocjan T, Hocevar M, Fettich J. 18F-Fluorocholine PET/CT for localization of hyperfunctioning parathyroid tissue in primary hyperparathyroidism: a pilot study. Eur J Nucl Med Mol Imaging. 2014;41:2083–9. https://doi.org/10.1007/s00259-014-2837-0.
Rep S, Lezaic L, Kocjan T, Pfeifer M, Sever MJ, Simoncic U, Tomse P, Hocevar M. Optimal scan time for evaluation of parathyroid adenoma with [(18)F]-fluorocholine PET/CT. Radiol Oncol. 2015;49:327–33. https://doi.org/10.1515/raon-2015-0016.
Hocevar M, Lezaic L, Rep S, Zaletel K, Kocjan T, Sever MJ, Zgajnar J, Peric B. Focused parathyroidectomy without intraoperative parathormone testing is safe after pre-operative localization with 18F-Fluorocholine PET/CT. Eur J Surg Oncol. 2017;43:133–7. https://doi.org/10.1016/j.ejso.2016.09.016.
Rep S, Hocevar M, Vaupotic J, Zdesar U, Zaletel K, Lezaic L. 18F-choline PET/CT for parathyroid scintigraphy: significantly lower radiation exposure of patients in comparison to conventional nuclear medicine imaging approaches. J Radiol Prot. 2018;38:343–56. https://doi.org/10.1088/1361-6498/aaa86f.
Alharbi AA, Alshehri FM, Albatly AA, Sah B-R, Schmid C, Huber GF, Huellner MW. [18F]fluorocholine uptake of parathyroid adenoma is correlated with parathyroid hormone level. Mol Imaging Biol. 2018;20:857–67. https://doi.org/10.1007/s11307-018-1179-x.
Beheshti M, Hehenwarter L, Paymani Z, Rendl G, Imamovic L, Rettenbacher R, Tsybrovskyy O, Langsteger W, Pirich C. 18F-Fluorocholine PET/CT in the assessment of primary hyperparathyroidism compared with 99mTc-MIBI or 99mTc-tetrofosmin SPECT/CT: a prospective dual-centre study in 100 patients. Eur. J. Nucl. Med. Mol. Imaging. 2018;45:1762–71. https://doi.org/10.1007/s00259-018-3980-9.
Bossert I, Chytiris S, Hodolic M, Croce L, Mansi L, Chiovato L, Mariani G, Trifirò G. PETC/CT with 18F-Choline localizes hyperfunctioning parathyroid adenomas equally well in normocalcemic hyperparathyroidism as in overt hyperparathyroidism. J Endocrinol Invest. 2019;42:419–26. https://doi.org/10.1007/s40618-018-0931-z.
Christakis I, Khan S, Sadler GP, Gleeson FV, Bradley KM, Mihai R. 18Fluorocholine PET/CT scanning with arterial phase-enhanced CT is useful for persistent/recurrent primary hyperparathyroidism: first UK case series results. Ann R Coll Surg Engl. 2019;101:501–7. https://doi.org/10.1308/rcsann.2019.0059.
Thanseer NTK, Parihar AS, Sood A, Bhadada SK, Dahiya D, Singh P, Mittal BR. Evaluation of recurrent parathyroid carcinoma: a new imaging tool in uncommon entity. World J Nucl Med. 2018;18:198–200. https://doi.org/10.4103/wjnm.WJNM_67_18.
Broos WAM, van der Zant FM, Knol RJJ, Wondergem M. Choline PET/CT in parathyroid imaging: a systematic review. Nucl Med Commun. 2019;40:96–105. https://doi.org/10.1097/MNM.0000000000000952.
Hansen BB, Hansen P, Nordberg CL, Boesen M. Imaging of the spine in cases of low back pain. Ugeskr Laeger. 2018;180(16):V06170475
Fukumoto M. Single-photon agents for tumor imaging: 201Tl, 99mTc-MIBI, and 99mTc-tetrofosmin. Ann Nucl Med. 2004;18:79–95. https://doi.org/10.1007/bf02985098.
Vallabhajosula S. (18)F-labeled positron emission tomographic radiopharmaceuticals in oncology: an overview of radiochemistry and mechanisms of tumor localization. Semin Nucl Med. 2007;37:400–19. https://doi.org/10.1053/j.semnuclmed.2007.08.004.
Ishizuka T, Kajita K, Kamikubo K, Komaki T, Miura K, Nagao S, Nozawa Y. Phospholipid/Ca2 + -dependent protein kinase activity in human parathyroid adenoma. Endocrinol Jpn. 1987;34:965–8. https://doi.org/10.1507/endocrj1954.34.965.
Kim S-J, Lee S-W, Jeong SY, Pak K, Kim K. Diagnostic performance of F-18 fluorocholine PET/CT for parathyroid localization in hyperparathyroidism: a systematic review and meta-analysis. Horm Cancer. 2018;9:440–7. https://doi.org/10.1007/s12672-018-0347-4.
Treglia G, Piccardo A, Imperiale A, Strobel K, Kaufmann PA, Prior JO, Giovanella L. Diagnostic performance of choline PET for detection of hyperfunctioning parathyroid glands in hyperparathyroidism: a systematic review and meta-analysis. Eur J Nucl Med Mol Imaging. 2019;46:751–65. https://doi.org/10.1007/s00259-018-4123-z.
Boccalatte LA, Higuera F, Gómez NL, de la Torre AY, Mazzaro EL, Galich AM, Collaud C, Figari MF. Usefulness of 18F-fluorocholine positron emission tomography-computed tomography in locating lesions in hyperparathyroidism: a systematic review. JAMA Otolaryngol Head Neck Surg. 2019. https://doi.org/10.1001/jamaoto.2019.0574.
Johnson NA, Tublin ME, Ogilvie JB. Parathyroid imaging: technique and role in the preoperative evaluation of primary hyperparathyroidism. AJR Am J Roentgenol. 2007;188:1706–15. https://doi.org/10.2214/AJR.06.0938.
Yildiz S, Aralasmak A, Yetis H, Kilicarslan R, Sharifov R, Alkan A, Toprak H. MRI findings and utility of DWI in the evaluation of solid parathyroid lesions. Radiol Med. 2019;124:360–7. https://doi.org/10.1007/s11547-018-0970-8.
Starker LF, Mahajan A, Bjorklund P, Sze G, Udelsman R, Carling T. 4D parathyroid CT as the initial localization study for patients with de novo primary hyperparathyroidism. Ann Surg Oncol. 2011;18:1723–8.
Mekel M, Linder R, Bishara B, Kluger Y, Bar-On O, Fischer D. 4-dimensional computed tomography for localization of parathyroid adenoma. Harefuah. 2013;152:710–2.
Hamidi M, Sullivan M, Hunter G, Hamberg L, Cho NL, Gawande AA, et al. 4D-CT is superior to ultrasound and sestamibi for localizing recurrent parathyroid disease. Ann Surg Oncol. 2018;25(5):1403–9.
Tian Y, Tanny ST, Einsiedel P, Lichtenstein M, Stella DL, Phal PM, et al. Four-dimensional computed tomography: clinical impact for patients with primary hyperparathyroidism. Ann Surg Oncol. 2018;25:117–21.
Argirò R, Diacinti D, Sacconi B, Iannarelli A, Diacinti D, Cipriani C, Pisani D, Romagnoli E, Biffoni M, Di Gioia C, Pepe J, Bezzi M, Letizia C, Minisola S, Catalano C. Diagnostic accuracy of 3T magnetic resonance imaging in the preoperative localisation of parathyroid adenomas: comparison with ultrasound and 99mTc-sestamibi scans. Eur Radiol. 2018;28:4900–8. https://doi.org/10.1007/s00330-018-5437-8.
Ozturk M, Polat AV, Celenk C, Elmali M, Kir S, Polat C. The diagnostic value of 4D MRI at 3T for the localization of parathyroid adenomas. Eur J Radiol. 2019;112:207–13. https://doi.org/10.1016/j.ejrad.2019.01.022.
Acknowledgments
Open access funding provided by Università degli Studi di Padova within the CRUI-CARE Agreement.
Funding
No grants or fellowships have supported the writing of the paper.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Evangelista Laura: nothing to disclose. Ravelli Ilaria: nothing to disclose. Magnani Fabio: nothing to disclose. Iacobone Maurizio: nothing to disclose. Chiara Giraudo: nothing to disclose. Camozzi Valentina: nothing to disclose. Spimpolo Alessandro: nothing to disclose. Cecchin Diego: nothing to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Evangelista, L., Ravelli, I., Magnani, F. et al. 18F-choline PET/CT and PET/MRI in primary and recurrent hyperparathyroidism: a systematic review of the literature. Ann Nucl Med 34, 601–619 (2020). https://doi.org/10.1007/s12149-020-01507-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12149-020-01507-1