
Abstract
This cross-sectional study investigated the mental health of Italian women who gave birth during the three years of the COVID-19 pandemic. The study focused on the impact of the partner’s presence during childbirth, the time point of birth in relation to pandemic waves, hospital restrictions, and individual attitudes regarding the pandemic. In addition, the study aimed to determine potential risk or protective factors for postpartum depression. 1,636 Italian women who gave birth between 2020 and 2022 in a hospital-restricted setting were surveyed anonymously online. Standardized questionnaires were used to evaluate depression, post-traumatic stress, and psychological well-being. Women who gave birth in 2020 had the highest percentage of unaccompanied births and higher levels of depression and fear of COVID-19. Women who gave birth alone reported higher depression and post-traumatic stress and lower psychological well-being. Furthermore, they were more frightened by COVID-19 and less in agreement with pandemic restrictions than women who gave birth with their partner present. The main risk factors for postpartum depression were childbirth in 2020, high COVID-19 anxiety, discomfort with pandemic restrictions, and the partner’s absence during birth. Protective factors were the partner’s presence during childbirth and satisfaction with the partner relationship. This study emphasizes the importance of targeted support to women who give birth during crises such as the COVID-19 pandemic to reduce risk factors and enhance protective factors, particularly by strengthening the partner’s presence. Future research should focus on children born during these tumultuous periods, assessing potential impacts on their developmental trajectories and relationships with primary caregivers.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
COVID-19 pandemic as a non-normative event in the postpartum period
Pregnancy, birth, and motherhood are critical stages in a woman’s life and are considered biopsychosocial events. Biological factors, as well as psychological and social factors, play a significant role both during pregnancy and after birth, and mental health can directly impact maternal and neonatal health outcomes (Blount et al., 2021).
The lifespan perspective classifies two life events that challenge individual development and well-being (Hendry & Kloep, 2002). Normative events are associated with a specific time and strongly correlate with age-related social practices or biological factors. In this sense, the birth of a child can undoubtedly be considered a normative event (Samuel & Vilter, 2008). Non-normative events, however, are unpredictable and unique experiences unrelated to a specific point in an individual’s development or a specific historical period (Koulenti & Anastassiou-Hadjicharalambous, 2011). From this perspective, the events that occur unexpectedly during pregnancy and childbirth, such as medical complications, newborn disabilities/diseases, marital problems, and stressful life events, can affect mothers’ and fathers’ postpartum well-being and the quality of their future relationship with the child (Carmichael et al., 2007; Ding et al., 2021).
COVID-19 pandemic and the unprecedented lockdown measures adopted to counter the spread of the disease undoubtedly fall into the category of non-normative life events and developmental challenges (Calandri et al., 2021; Hendry & Kloep, 2002), during which subjects in more delicate developmental stages were most affected by the psychological effects (Commodari & La Rosa, 2020; Craparo et al., 2022; La Rosa et al., 2022). In particular, the COVID-19 pandemic had a significant psychological impact on women in the postpartum period (Hessami et al., 2022). In this regard, recent studies (Lin et al., 2023; Safi-Keykaleh et al., 2022) suggested that the COVID-19 pandemic has increased the risk of postpartum depression (PPD) in new mothers compared to the pre-pandemic period. A recent meta-analysis by Chen et al. (2022) investigated the effect of the COVID-19 pandemic on the prevalence of PPD based on eight cross-sectional studies of women up to 18 months postpartum. The results showed that during the COVID-19 pandemic, the pooled prevalence of PPD using a cut-off score of 13 or higher on the Edinburgh Postnatal Depression Scale (EPDS) (Cox et al., 1987) was 34% (95% CI: 21–46), much higher than during the non-pandemic period (approximately 10–26%) (Chen et al., 2022). Data reported in the meta-analysis by Lin et al. (2023) and Safi-Keykaleh et al. (2022) also confirm a higher prevalence of PPD during the pandemic than in the pre-pandemic period (24% and 28%, respectively). However, the PPD prevalence rates are lower than those reported by Chen et al. (2022).
The role of partner support during the COVID-19 pandemic
The COVID-19 pandemic and the associated lockdown measures are likely exacerbating the most significant risk factors for the onset of mood disorders in the postpartum period, including lack of social support, distance from family, economic and work-related challenges, pregnancy complications, cesarean section, traumatic experiences related to childbirth. Other specific risk factors that may increase the risk of PPD during the pandemic include fear and worry about COVID-19 infection, hospital visitation restrictions, and reduced social support (Shuman et al., 2022).
Research before the pandemic has shown that the partner’s presence during birth has several psychological benefits for new mothers, including reduced anxiety levels, increased support and comfort, and improved maternal-infant bonding (Bohren et al., 2017; Britton, 2008; Peter et al., 2017; Reblin & Uchino, 2008). The partner’s presence during childbirth can also help new mothers feel more in control and empowered during an overwhelming and stressful time (Beigi et al., 2016; Ip, 2001; Schmitt et al., 2022). Therefore, the absence of partners during birth has been associated with adverse psychological outcomes, such as increased anxiety levels, depression, and post-traumatic stress symptoms (Ford & Ayers, 2011; Ford et al., 2010; Surkan et al., 2006). Until now, limited research exists that investigated the role of partner support during childbirth and the postpartum period in the COVID-19 pandemic, both in Italy and other countries.
Specific to the pandemic period, Molgora and Accordini (2020) investigated the effect of the presence or absence of a partner during childbirth on anxiety and depressive disorders as well as post-traumatic stress symptoms in a sample of 575 Italian women recruited between March 1, 2020, and May 3, 2020. This study revealed that women who did not have their partners with them during childbirth were found to be at a higher risk of experiencing not only clinically relevant state anxiety and trait anxiety but also of developing postpartum post-traumatic stress symptoms. Furthermore, a study by Meister et al. (2022), conducted on 131 postpartum women between March and October 2020, reported a significant increase in postpartum depression scores in the first days after birth due to the separation from the partner. In contrast, mothers supported by their partners during childbirth reported significantly decreased levels of postpartum depression. Regarding experiences in other countries, a recent study of our research group (Oddo-Sommerfeld et al., 2022) investigated the psychological effects of COVID-19 visiting restrictions on mothers who gave birth alone and compared them with those with partners present. Even though the sample was small (54 mothers, half of whom gave birth alone), this study also pointed out that mothers who gave birth unaccompanied experienced higher levels of anxiety, post-traumatic stress symptoms, and depression, especially those who had a cesarean section. These mothers also perceived restrictions more negatively and suffered more from their partner’s absence.
Although limited, the results of these studies in the pandemic period confirm the importance of the partner’s support both at the time of birth and in the postpartum period in relation to the mother’s risk of developing PPD. The partner’s support becomes more important at such a critical time as the pandemic and, therefore, requires a specific, in-depth investigation with a large sample to allow adequate generalization of the results.
The Italian context
In addition, relatively few studies have been conducted in Italy on women’s mental health (anxiety, depression, and post-traumatic stress symptoms) in the postpartum period during the COVID-19 pandemic. For instance, Ostacoli et al. (2020) investigated the prevalence of depressive and post-traumatic stress symptoms among 163 women who gave birth during the first wave of the COVID-19 pandemic (between March 8 and June 15, 2020) as well as the associations with lockdown measures, obstetric factors, and attachment style. As the study revealed, depressive symptoms were found in 44.2% of women using a cut-off score of ≥ 11 on the EPDS (Smith-Nielsen et al., 2018), while the rate of post-traumatic stress symptoms was 42.9% using a cut-off score of ≥ 24 on the Impact of Event Scale-Revised (Asukai et al., 2002).
Orsolini et al. (2022) evaluated the influence of anxiety and fear related to the COVID-19 pandemic on perinatal depression in a sample of 184 Italian postpartum women screened from March 2020 to March 2021. According to the results, 45.7% of participants experienced clinically relevant perinatal depression, and there was a positive correlation between COVID-19-related fear and anxiety and perinatal depression. Spinola et al. (2020) investigated how the COVID-19 pandemic influenced postpartum depressive symptoms in 243 Italian mothers with children less than a year old during the first wave of the pandemic (between May and June 2020). They reported that 44% of the mothers showed symptoms of postpartum depression as per the EPDS (cut-off score > 12).
A limitation of the reported studies is that the vast majority of research on this topic in Italy has focused on relatively small samples, often conducted in specific areas of the country, particularly in northern Italy, and during particular stages of the pandemic, without making a comparison between different waves of the pandemic and between different levels of severity of restrictive measures.
Study aims
Given the existing gap in the literature, it is interesting to investigate the pandemic’s impact on the postpartum period in more detail using a large sample of Italian women. Furthermore, it is essential to compare the women’s experiences during different stages of the pandemic, as these stages are characterized by varying degrees of restrictive measures that can be expected to affect women’s mental health.
Therefore, the first aim of this study was to investigate how COVID-19-related hospital restrictions affected mental health variables (depression, post-traumatic stress, psychological well-being) and obstetric characteristics of a comprehensive cohort of Italian women who gave birth during the pandemic and how these effects changed during the different phases (3 years) of the pandemic. As the hospital restrictions during the pandemic included that the women’s partners were not allowed to be present at the time of birth, the second objective was to examine whether women with and without their partner present at childbirth differed in their levels of psychological distress and well-being and whether these effects varied according to the stage of the pandemic during which the women gave birth. The third objective was to investigate the extent to which variables explicitly related to the COVID-19 experience, such as fear of infection, mode of birth, discomfort with hospital restrictions, and alignment with COVID-19 measures, influenced levels of postpartum depression, post-traumatic stress, and psychological well-being in the different waves of the pandemic. Finally, we aimed to detect risk and protective factors related to postpartum depression, focusing on birth-related variables, COVID-19 pandemic-related variables, and partner-related variables.
Materials and methods
Study design and participants
The present cross-sectional, observational study is part of a larger research project on the psychological well-being and postpartum attachment of Italian women who gave birth during the COVID-19 pandemic. The inclusion criteria for the study were Italian women who gave birth following the restrictions imposed on hospitals to contain the spread of the COVID-19 infection and could provide informed consent. In contrast, the exclusion criteria ruled out women with previous psychiatric comorbidities and/or undergoing psychopharmacological therapy.
The study was conducted between 2020 and 2022, covering the main phases of the COVID-19 pandemic in Italy, characterized by different types of restrictive measures and varying degrees of severity. In particular, during the first wave of the pandemic, hospitals implemented visitation restrictions that prohibited the presence of any accompanying persons, including the partners of women, during childbirth. Restrictive measures were gradually relaxed from 2021 and throughout 2022, and the presence of the partners or supporting persons during birth was expected in case of possession of the Green Pass (a certificate required in Italy to gain access to certain activities and certifications of COVID-19 vaccinations or recovery from the disease or a negative COVID-19 test). However, many hospitals continued to maintain the strictest restrictive measures even in the later stages of the pandemic. Based on these considerations, we classified the women in our sample into three groups based on their baby’s birth time. The first group included women who gave birth from March 9 to December 31, 2020, during the most challenging period of the restrictions; the second group included women who gave birth from January 1 to December 31, 2021, during a period of gradual relaxation of COVID-19 rules; the third group included women who gave birth from January 1 to June 13, 2022, a period characterized by a gradual return to normalcy with more limited restrictions.
A web-based survey was shared through the leading social media platforms (Twitter, Facebook, and Instagram) and online groups dedicated to perinatal mental health. The survey was made available for one year, from June 1, 2021, to June 30, 2022, until a sufficient number of responses had been reached to ensure a comprehensive analysis and enhance the robustness of the study findings. On average, the survey required 20 min to complete. Participants completed the survey anonymously, voluntarily, and without remuneration or incentives. The survey platform was configured to prevent multiple responses from the same IP address. In addition, a thorough manual examination of the collected data was conducted to identify and eliminate potential duplicates based on a review of demographic information and response patterns.
All study participants provided online informed consent by filling out a specific form. The Ethics Committee of the Department of Educational Sciences of the University of Catania approved the study protocol.
Measures
The online survey included first a section in which the participants provided socio-demographic and childbirth-related information. The second section of the survey collected a selection of obstetric variables, such as infant Apgar index, pregnancy-related hospitalizations, risk factors, complications during childbirth, preterm births, and prior miscarriages. Then, mothers responded to a series of questions about the importance they placed on their partner’s presence and support during childbirth, their knowledge of and agreement with restraint measures during childbirth, and their concerns about COVID-19 restrictions. Finally, participants completed a battery of standardized questionnaires to assess postpartum depression, post-traumatic stress symptoms related to the birth experience during the COVID-19 pandemic, and psychological well-being.
Impact of Event Scale-Revised (IES-R)
The IES-R (Creamer et al., 2003) measures distress following exposure to traumatic events and was adapted for the specific aims of this study, focusing on the birth event during the COVID-19 pandemic. It consists of 22 items (e.g., “Any reminders brought back feelings about it,” “Other things kept making me think about it,” “I felt as if it hadn’t happened or wasn’t real”) rated on a 5-point rating scale ranging from 0 (Not at all) to 4 (Extremely). The questionnaire assesses the total post-traumatic stress score and sum scores of three subscales corresponding to the three main clusters of post-traumatic stress (i.e., intrusion, avoidance, and hyperarousal). In this study, the total score is used. A total score ≥ 24 is considered indicative of the presence of post-traumatic stress symptoms. The Italian version of the questionnaire (Craparo et al., 2013) was used in this study. The reliability of the IES-R total score in this study was ωFootnote 1 = 0.91.
Edinburgh Postnatal Depression Scale (EPDS)
The EPDS (Cox et al., 1987) is an often-used scale for screening PPD. It consists of 10 items (e.g., “I have been able to laugh and see the funny side of things,” “I have been so unhappy that I have had difficulty sleeping,” “I have been so unhappy that I have been crying”) that women had to answer on a 4-point rating scale referring to how they felt during the last week. Typically, a sum score of 12 or above is considered a cut-off for further assessment of depressive symptoms in the postpartum period, as reported in the recent study by Orsolini et al. (2022). The reliability of EPDS in this study was ω = 0.85.
World Health Organization Well-Being Index (WHO-5)
The WHO-5 is a self-report questionnaire used to assess subjective psychological well-being (World Health Organization Regional Office for Europe & Psychiatric Research Unit, 1998). First published in 1998, it has been translated into 30 different languages (including Italian) and used in numerous studies worldwide. It consists of 5 items considering the last 14 days (e.g., “I have felt cheerful and in good spirits,” “I have felt calm and relaxed,” “I have felt active and vigorous”) that the subject is asked to answer on a 6-point Likert-type scale ranging from 0 (At no time) to 5 (All of the time). The total score is calculated by summing the responses to the five items. The total score ranges from 0 to 25, where 0 represents the worst possible quality of life, and 25 represents the best possible quality of life. According to the literature, a score below 13 indicates a poor state of psychological well-being (World Health Organization Regional Office for Europe & Psychiatric Research Unit, 1998). The reliability of WHO-5 in this study was ω = 0.84.
Statistical analyses
Statistical analyses were conducted using the Statistical Package for the Social Sciences (SPSS), version 25.0 (IBM Corporation, Armonk, NY). McDonald’s ω (McDonald, 1999) was calculated to evaluate the reliability of the scales used in this study since the assumption of τ-equivalent items, which Cronbach’s α is based on, is seldom fulfilled in empirical data (Sijtsma, 2009). Means (M) and standard deviations (SD) were provided for continuous variables, while categorical variables were expressed as frequencies and percentages. Two-way ANOVAs were conducted to examine the effect of the year of birth and the presence of the partner during childbirth on psychological constructs and COVID-19 pandemic-related variables (fear of COVID-19 infection and agreement with hospital restrictions). Finally, a binary logistic regression analysis with a blockwise entry of the independent variables was conducted to identify the primary risk and protective factors for PPD among mothers who gave birth during the pandemic. The first model included childbirth mode (spontaneous vaginal birth as reference category, planned cesarean section, unplanned cesarean section, and vaginal birth with episiotomy), the second model added COVID-19 pandemic-related variables (birth year, fear of COVID-19 infection, discomfort with COVID-19 restrictions, agreement with COVID-19 restrictions), and the third model added partner-related variables (years of relationship with the partner, satisfaction with partner relationship, presence of the partner during childbirth, importance given to partner’s support during birth, importance given to partner’s support in the ward). The odds ratios (ORs) and 95% confidence intervals (CI) are reported. A p-value < 0.05 was considered statistically significant.
Results
Socio-demographic and obstetric characteristics of the sample
A total of 2027 women answered the survey. Participants with past (n = 308) and current (n = 140) psychiatric comorbidities were excluded from the sample. In addition, women taking psychopharmacological therapy before (n = 140) and at the time of the study (n = 36) were also excluded from the sample. Therefore, the final sample included 1636 mothers. The mean age of the participants was 32.45 (SD = 4.38, range = 19–50). Table 1 reports all the sample socio-demographic characteristics.
In 2020, 388 women gave birth. Within this group, 49.2% experienced birth through spontaneous vaginal delivery. Planned cesarean sections were conducted in 10.1% of the cases, while unplanned cesarean sections accounted for 17.3%. Additionally, 23.5% of the deliveries were vaginal births that necessitated an episiotomy. Most women in our sample gave birth in 2021 (n = 961). Of these childbirths, 55.8% were spontaneous vaginal births. The rate of planned cesarean sections was 10.4%, whereas the rate of unplanned cesarean sections remained constant at 17.3%. The prevalence of vaginal births requiring episiotomies was 16.5%. Two hundred fifty-six women gave birth in 2022. Of these, 59.8% had a spontaneous vaginal birth, 8.2% had a planned cesarean section, 14.5% had an unplanned cesarean section, and 17.6% had a vaginal birth with episiotomy. Table 2 shows these and other main obstetric characteristics of the sample.
COVID-19 restrictions during childbirth
One-third of the women in our sample gave birth alone without their partner, with the highest percentage recorded in 2020 during the first phase of the pandemic (41.8%). Partner absence during birth was due to the COVID-19 restrictions in two-thirds of the mothers, and the rest was unrelated to restrictive measures. Again, 2020 showed the highest percentage of women who gave birth alone due to COVID-19-related restrictions (69.9%) compared to 2021 (56.1%) and 2022 (59.2%). In addition, nearly all women who underwent cesarean section gave birth alone, without significant differences in the three pandemic years. Almost all mothers were aware of the restrictions adopted in the hospital, and 72.7% would still have given birth in the same hospital. Furthermore, 71.4% of the women said restrictions during childbirth did not affect their relationship with their partner, while 19.3% said restrictions affected it negatively. All data are reported in the Supplementary Table 1.
Effects of partner presence during childbirth and year of birth on psychological well-being, depression, and post-traumatic stress
Table 3 reports all the prevalence rates of psychological well-being, depression, and post-traumatic stress during the pandemic years. Overall, a high prevalence of low psychological well-being, depression, and post-traumatic stress can be observed in the general sample along the three-year pandemic period. However, the highest rates are reported by the group of women who gave birth without their partners. More specifically, the highest prevalence of depression is recorded in women who gave birth alone during 2020 (48.8%), as well as for low psychological well-being (64.2%) and post-traumatic stress (55.6%).
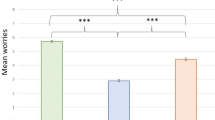
Two-way ANOVAs were conducted to explore the influence of the partner’s presence during childbirth and the year of birth on maternal psychological outcomes, including psychological well-being, depression, and post-traumatic stress, across the three years of the COVID-19 pandemic. The main effect of the variable partner presence during childbirth was significant concerning both psychological well-being (F = 7.26; df = 1; p =.007) and post-traumatic stress (F = 21.38; df = 1; p <.001). In particular, Table 3 shows that women who gave birth without their partners reported lower levels of psychological well-being (M = 11.36; SD = 5.29) and higher levels of post-traumatic stress (M = 29.04; SD = 18.54) across all three years of the study (Fig. 1). While the overall effect of the year of birth was not significant for psychological well-being and post-traumatic stress (all p’s > 0.05), the impact of the year of birth on depression was significant (F = 8.99; df = 2; p <.001), with the highest rates of depression observed in the first year of the pandemic (Fig. 1). The interaction between the partner’s presence and year of birth was significant in the context of depression. The highest prevalence of depression was reported among women who gave birth alone during the first phase of the pandemic (M = 11.52; SD = 5.82). The non-significant interaction effect for psychological well-being and post-traumatic stress (all p’s > 0.05) suggests that the impact of partner presence on these outcomes was consistent, regardless of the pandemic year.

Mean differences in psychological well-being, postpartum depression and post-traumatic stress scores based on the year of childbirth and the partner presence at childbirth
ANOVA statistics are reported in the Supplementary Table 2.
COVID-19-related variables
Regarding COVID-19-related variables, two-way ANOVAs were conducted to examine the effects of the partner’s presence during childbirth and year of birth on the fear of COVID-19 infection and the agreement with hospital restrictions. Regarding the fear of COVID-19, the main effect of the partner’s presence during childbirth (F = 3.87; df = 1; p =.04) and that of the year of birth (F = 5.04; df = 1; p =.007) were significant. More in detail, women who gave birth alone during the first year of the pandemic reported higher levels of fear of COVID-19 (M = 3.44; SD = 1.13) (Fig. 2). Regarding the agreement with hospital restrictions, the main effect of the partner’s presence during childbirth was statistically significant (F = 10.53; df = 1; p =.001) but not that of the year of birth (F = 2.15; df = 2; p =.12). In particular, women who gave birth with their partner present during childbirth reported higher levels of agreement with COVID-19 restrictions (M = 2.78; SD = 1.32) (Fig. 2). ANOVA statistics are reported in the Supplementary Material, Table 3.

Mean differences in fear of COVID-19 and agreement with COVID-19 restrictions based on the year of childbirth and the partner presence at childbirth
Risk and protective factors for PPD during the COVID-19 pandemic
Table 4 lists the logistic regression odds ratios with the binary dependent variable PPD (0/1). Hosmer-Lemeshow χ2 indicates a good model fit (all p’s > 0.05) with increasing Nagelkerke’s R2 values for all three models. Because of multicollinearity, odds ratios can only be interpreted with all other variables in the blocks held constant. Model 1 assessed the relationship between different childbirth modes and the odds of being depressed compared to the odds of the outcome occurring for spontaneous vaginal birth. The results show that women with planned cesarean section or vaginal birth with episiotomy had significantly higher odds of being depressed than women with spontaneous vaginal birth. Adding COVID-19 pandemic-related variables in model 2 revealed that women who gave birth in 2021 or 2022 had lower odds of PPD than those giving birth in 2020. In contrast, women with a stronger fear of COVID-19 had higher odds of being depressed than women with lower fear.
In model 3, in which partner-related variables were added to the model, women who were satisfied with their partner relationship had 58.4% lower odds of being depressed than women who were less satisfied with their relationship. Furthermore, women whose partner was present at childbirth had 28.4% lower odds of PPD than those with no partner present. Neither the importance given to the partner’s support during birth nor in the ward was significantly related to the outcome variable.
The only significant birth mode was now vaginal birth with episiotomy. Women with this birth mode increased the odds of PPD by 36.5% compared to women with spontaneous vaginal birth. COVID-19 pandemic-related variables were now all significantly associated with the outcome, except for agreement with COVID-19 restrictions. Higher levels of fear of COVID-19 increased the odds of PPD (45.5%), as well as higher levels of discomfort with COVID-19 restrictions (15.3%) compared to lower levels of these variables. The results also revealed that women who gave birth in 2021 had 38% lower odds of experiencing PPD, and those who gave birth in 2022 had 32.4% lower odds of PPD compared to women who gave birth in 2020.
Discussion
This study explored depression, post-traumatic stress symptoms, and psychological well-being in a large sample of Italian mothers who gave birth during the years of the COVID-19 pandemic. In particular, we investigated the relationship between these mental health variables, obstetric variables, social support, and the COVID-19 restrictions during childbirth, differentiating between three different pandemic periods between 2020 and 2022.
In general, the Italian women in our sample showed high mental distress in all psychological variables (depression, post-traumatic stress, low well-being). The prevalence of depression, post-traumatic stress, and low well-being are much higher than those known in the postpartum period in general and even comparable to the prevalence known for risk groups of mothers with, e.g., preterm birth or pregnancy/delivery complications (Nguyen et al., 2023; Sommerlad et al., 2021). The high prevalence detected in our study underlines the suffering of mothers who gave birth during the pandemic and confirms the high impact of the pandemic on mothers’ and families’ mental health.
In particular, our results show differences between the pandemic years and the presence of the partner at birth. In this regard, we found that giving birth in the first year of the pandemic, when restrictions were more severe, was related to higher levels of depression but not to post-traumatic stress or psychological distress. Furthermore, the absence of the partner during childbirth was associated with higher levels of depression and post-traumatic stress and lower levels of psychological well-being. Further, women who gave birth alone during the first year of the pandemic reported higher levels of fear of COVID-19. The opportunity for women to have their partner by their side during childbirth facilitated the acceptance of hospital restrictions against COVID-19.
One of our study’s most compelling findings was identifying the main risk factors for PPD during the pandemic. We showed that the variables related to the COVID-19 pandemic were significantly associated with the odds of being depressed in the postpartum period. Specifically, women who gave birth in 2021 or 2022, years with less severe COVID-19 restrictions, had lower odds of PPD than women who gave birth in the first wave of the pandemic. This finding is noteworthy because it suggests that depressive symptoms were more prevalent than stress symptoms among women who gave birth during the most severe lockdown periods. One possible explanation for this finding is that the stricter COVID-19 restrictions resulted in increased isolation and reduced social support, which may have contributed to depressive feelings (Jones et al., 2022). Other significant risk factors for PPD in women of our sample were higher fear of COVID-19 infection and discomfort with COVID-19 restrictions.
Besides the higher depression in women during the first pandemic year, in our study, a considerable percentage of participants reported high levels of post-traumatic stress (49.8%). Compared to studies before the pandemic, which usually reveal a prevalence of post-traumatic stress following childbirth of 3–4% (Grekin & O’Hara, 2014; Williams et al., 2022; Yildiz et al., 2017), our sample reported post-traumatic stress to a considerable extent. Furthermore, 53.9% of the mothers in our sample reported low psychological well-being, with many attributing their symptoms to pandemic-related stressors such as social isolation, COVID-19 restrictions, and concerns about the health and safety of themselves and their newborns. These data align with the international literature on the psychological impact of the pandemic on the postpartum period, which shows that women who gave birth during the pandemic reported adverse mental health outcomes, especially traumatic childbirth, and psychological distress (Mayopoulos et al., 2021; Ostacoli et al., 2020). Furthermore, a preliminary study conducted in Germany in the early stages of the pandemic also confirmed that women who gave birth alone during that period reported significantly higher levels of post-traumatic stress symptoms, anxiety, depression, and psychological discomfort (Oddo-Sommerfeld et al., 2022). In this regard, there are no differences between the experiences of Italian mothers and those of other countries.
A good relationship with the partner and the partner’s presence during childbirth were protective factors against the PPD risk, confirming the crucial role of emotional support from the partner already documented in other studies (Redshaw & Henderson, 2013). Therefore, the predictive model of PPD during the pandemic confirmed that the partner’s presence at birth is an essential factor influencing maternal psychological outcomes. Indeed, according to our results, women who gave birth alone without their partner reported higher depression and post-traumatic stress symptoms and lower psychological well-being than women who gave birth with their partner present. Indeed, the partner is essential during labor to provide information and emotional support and facilitate communication between mothers and health professionals (Ecker & Minkoff, 2020). In this sense, the birth event implies not only the involvement of the mother-child couple but also of the family’ triad’ (Backstrom & Hertfelt Wahn, 2011; Redshaw & Henderson, 2013). Therefore, it is crucial to ensure partner support for the woman during labor and birth, even during the post-pandemic period, to reduce the potentially traumatic impact of this experience.
In general, our results indicate that the impact of the pandemic on women’s mental health in the postpartum period may not be directly related to COVID-19 itself but rather to the traumatic experience of childbirth with reduced social support caused by COVID-19 restrictions. However, the literature on this matter reported conflicting information. On the one hand, Ostacoli et al. (2020) suggested that postpartum psychological distress was more closely tied to prenatal experiences and individual factors rather than pandemic-related hospital restrictions. On the other hand, Zanardo et al. (2020) highlighted that COVID-19 exposure concerns and quarantine measures during the pandemic had adverse effects on new mothers’ thoughts and emotions, worsening depressive symptoms.
Therefore, our results are significant because they provide evidence that allows the identification of women most at risk of poor mental health after childbirth. Indeed, considering the potentially traumatic impact of the pandemic on the experience of becoming a mother, the findings of this study can help ensure comprehensive and adequate support in the post-pandemic period to provide a positive attachment relationship and the harmonic development of the child in a longer-term perspective. However, also beyond the pandemic, the present data can be transferred to other traumatic events that have an impact on mental health. If we see the pandemic as an example of crucial live events with a high risk for causing mental distress, then our data give evidence that social support and good coping strategies against anxiety might be necessary preventive steps in the perinatal period.
Strengths and limitations
This study has some important strengths. First, it provides a comprehensive overview of the psychological experience of women who gave birth during the years of the pandemic in Italy by highlighting the different impacts of the childbirth event based on the varying degree of severity of hospital restraints and the presence or absence of the partner at the time of birth. Another strength is the large sample size, with more than 1,600 Italian women. However, there are also several limitations. First, an internet-based questionnaire with self-reported measures was used, making it impossible to assess the accuracy of the answers and the effect of self-report bias. Secondly, since this was a cross-sectional study, causal relationships between variables could not be established. For this purpose, a longitudinal design would have allowed for a better understanding of the effects of the COVID-19 pandemic on postpartum women. Still, applying this study design was difficult due to the restrictions caused by the pandemic.
Moreover, we assessed risk factors during pregnancy, complications during delivery, and hospitalization. Still, we did not go into details regarding the type of complications and duration of hospitalization that maybe could have an impact on the mental health outcome. We also did not analyze in detail the mothers who had cesarean sections and mostly gave birth alone in the operation room. Finally, time since birth was variable in our sample, and the different time distance from the traumatic event of childbirth may have resulted in a variation in the intensity of the symptoms detected.
Conclusion
This study highlights the importance of providing support and resources to women who give birth during times of crisis, such as a pandemic. This support can include providing mental health resources, practical help, and encouraging self-care practices. By supporting the psychological well-being of women who give birth during the COVID-19 pandemic, it is possible to mitigate the adverse effects of psychological distress on both mothers and their babies. More specifically, this study highlights the importance of integrating comprehensive mental health screening into routine postpartum care, ensuring that such assessments are sensitive to the unique stressors introduced by the pandemic and other similar crises. The data also support the development of targeted support mechanisms, including telehealth services, to address barriers to mental health care that were exacerbated during the pandemic. Training for health care providers should also be improved, emphasizing the recognition and management of mental health problems in postpartum women, with particular attention to the nuanced ways in which global crises can affect maternal well-being. Incorporating these changes into clinical protocols and training programs may enable more robust preparation to support maternal mental health during current and future challenges, thereby reducing the long-term psychological impact on mothers and their families.
Future research should also investigate the developmental trajectories of children born during such crisis periods, exploring potential effects on their growth and relationships with caregivers. This insight can better inform our response to other traumatic life events that new mothers may face.
Data Availability
The dataset generated and analyzed during the current study is not publicly available due to the Department's privacy policies but is available from the corresponding author upon reasonable request.
Notes
Reliability for all scales used in this study was estimated by McDonald’s ω instead of Cronbach’s α.
References
Asukai, N., Kato, H., Kawamura, N., Kim, Y., Yamamoto, K., Kishimoto, J., Miyake, Y., & Nishizono-Maher, A. Y. A. (2002). Reliability and validity of the japanese-Language Version of the impact of event scale-revised (Ies-R-J): Four studies of different traumatic events. The Journal of Nervous and Mental Disease, 190(3), 175–182. https://doi.org/10.1097/00005053-200203000-00006
Backstrom, C., & Hertfelt Wahn, E. (2011). Support during labour: First-time fathers’ descriptions of requested and received support during the birth of their child. Midwifery, 27(1), 67–73. https://doi.org/10.1016/j.midw.2009.07.001
Beigi, M., Salehi, A., & Fahami, F. (2016). The effect of presence of trained husbands beside their wives during childbirth on women’s anxiety. Iranian Journal of Nursing and Midwifery Research, 21(6). https://doi.org/10.4103/1735-9066.197672
Blount, A. J., Adams, C. R., Anderson-Berry, A. L., Hanson, C., Schneider, K., & Pendyala, G. (2021). Biopsychosocial factors during the Perinatal period: Risks, preventative factors, and implications for Healthcare professionals. International Journal of Environmental Research and Public Health, 18(15). https://doi.org/10.3390/ijerph18158206
Bohren, M. A., Hofmeyr, G. J., Sakala, C., Fukuzawa, R. K., & Cuthbert, A. (2017). Continuous support for women during childbirth. Cochrane Database of Systematic Reviews, 7(7), CD003766. https://doi.org/10.1002/14651858.CD003766.pub6
Britton, J. R. (2008). Maternal anxiety: Course and antecedents during the early postpartum period. Depression and Anxiety, 25(9), 793–800. https://doi.org/10.1002/da.20325
Calandri, E., Graziano, F., Begotti, T., Cattelino, E., Gattino, S., Rollero, C., & Fedi, A. (2021). Adjustment to COVID-19 Lockdown among Italian University students: The role of concerns, change in peer and Family relationships and in learning skills, emotional, and academic self-efficacy on depressive symptoms. Frontiers in Psychology, 12, 643088. https://doi.org/10.3389/fpsyg.2021.643088
Carmichael, S. L., Shaw, G. M., Yang, W., Abrams, B., & Lammer, E. J. (2007). Maternal stressful life events and risks of birth defects. Epidemiology (Cambridge, Mass.), 18(3), 356–361. https://doi.org/10.1097/01.ede.0000259986.85239.87
Chen, Q., Li, W., Xiong, J., & Zheng, X. (2022). Prevalence and risk factors Associated with Postpartum Depression during the COVID-19 pandemic: A Literature Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 19(4). https://doi.org/10.3390/ijerph19042219
Commodari, E., & La Rosa, V. L. (2020). Adolescents in Quarantine during COVID-19 pandemic in Italy: Perceived Health risk, beliefs, psychological experiences and expectations for the future. Frontiers in Psychology, 11, 559951. https://doi.org/10.3389/fpsyg.2020.559951
Cox, J. L., Holden, J. M., & Sagovsky, R. (1987). Detection of postnatal depression. Development of the 10-item Edinburgh postnatal depression scale. The British Journal of Psychiatry, 150, 782–786. https://doi.org/10.1192/bjp.150.6.782
Craparo, G., Faraci, P., Rotondo, G., & Gori, A. (2013). The Impact of Event Scale - Revised: Psychometric properties of the Italian version in a sample of flood victims. Neuropsychiatric Disease and Treatment, 9, 1427–1432. https://doi.org/10.2147/NDT.S51793
Craparo, G., La Rosa, V. L., Marino, G., Vezzoli, M., Cinà, G. S., Colombi, M., Arcoleo, G., Severino, M., Costanzo, G., & Mangiapane, E. (2022). Risk of post-traumatic stress symptoms in hospitalized and non-hospitalized COVID-19 recovered patients. A cross-sectional study. Psychiatry Research, 308, 114353. https://doi.org/10.1016/j.psychres.2021.114353
Creamer, M., Bell, R., & Failla, S. (2003). Psychometric properties of the impact of event scale - revised. Behaviour Research and Therapy, 41(12), 1489–1496. https://doi.org/10.1016/j.brat.2003.07.010
Ding, X., Liang, M., Wu, Y., Zhao, T., Qu, G., Zhang, J., Zhang, H., Han, T., Ma, S., & Sun, Y. (2021). The impact of prenatal stressful life events on adverse birth outcomes: A systematic review and meta-analysis. Journal of Affective Disorders, 287, 406–416. https://doi.org/10.1016/j.jad.2021.03.083
Ecker, J. L., & Minkoff, H. L. (2020). Laboring alone? Brief thoughts on ethics and practical answers during the coronavirus disease 2019 pandemic. American Journal of Obstetrics & Gynecology MFM, 2(3). https://doi.org/10.1016/j.ajogmf.2020.100141
Ford, E., & Ayers, S. (2011). Support during birth interacts with prior trauma and birth intervention to predict postnatal post-traumatic stress symptoms. Psychology & Health, 26(12), 1553–1570. https://doi.org/10.1080/08870446.2010.533770
Ford, E., Ayers, S., & Bradley, R. (2010). Exploration of a cognitive model to predict post-traumatic stress symptoms following childbirth. Journal of Anxiety Disorders, 24(3), 353–359. https://doi.org/10.1016/j.janxdis.2010.01.008
Grekin, R., & O’Hara, M. W. (2014). Prevalence and risk factors of postpartum post-traumatic stress disorder: A meta-analysis. Clinical Psychology Review, 34(5), 389–401. https://doi.org/10.1016/j.cpr.2014.05.003
Hendry, L. B., & Kloep, M. (2002). Lifespan development: Resources, challenges and risks. Thomson Learning.
Hessami, K., Romanelli, C., Chiurazzi, M., & Cozzolino, M. (2022). COVID-19 pandemic and maternal mental health: A systematic review and meta-analysis. The Journal of Maternal-Fetal & Neonatal Medicine, 35(20), 4014–4021. https://doi.org/10.1080/14767058.2020.1843155
Ip, W. Y. (2001). Relationships between partner’s support during labour and maternal outcomes. Journal of Clinical Nursing, 9(2), 265–272. https://doi.org/10.1046/j.1365-2702.2000.00358.x
Jones, K., Harrison, V., Moulds, M. L., & Lazard, L. (2022). A qualitative analysis of feelings and experiences associated with perinatal distress during the COVID-19 pandemic. BMC Pregnancy and Childbirth, 22(1), 572. https://doi.org/10.1186/s12884-022-04876-9
Koulenti, T., & Anastassiou-Hadjicharalambous, X. (2011). Non-Normative Life Events. In S. Goldstein & J. A. Naglieri (Eds.), Encyclopedia of Child Behavior and Development (pp. 1018–1020). Springer US. https://doi.org/10.1007/978-0-387-79061-9_1977
La Rosa, V. L., Gori, A., Faraci, P., Vicario, C. M., & Craparo, G. (2022). Traumatic distress, Alexithymia, Dissociation, and risk of Addiction during the First Wave of COVID-19 in Italy: Results from a cross-sectional online survey on a non-clinical adult sample. International Journal of Mental Health and Addiction, 20(5), 3128–3144. https://doi.org/10.1007/s11469-021-00569-0
Lin, C., Chen, B., Yang, Y., Li, Q., Wang, Q., Wang, M., Guo, S., & Tao, S. (2023). Association between depressive symptoms in the postpartum period and COVID-19: A meta-analysis. Journal of Affective Disorders, 320, 247–253. https://doi.org/10.1016/j.jad.2022.09.129
Mayopoulos, G. A., Ein-Dor, T., Dishy, G. A., Nandru, R., Chan, S. J., Hanley, L. E., Kaimal, A. J., & Dekel, S. (2021). COVID-19 is associated with traumatic childbirth and subsequent mother-infant bonding problems. Journal of Affective Disorders, 282, 122–125. https://doi.org/10.1016/j.jad.2020.12.101
McDonald, R. P. (1999). Test theory: A unified treatment. L. Erlbaum Associates.
Meister, S., Dreyer, E. M., Hahn, L., Thomann, M., Keilmann, L., Beyer, S., Mayer, C., Prins, G., Hasbargen, U., Mahner, S., Jeschke, U., Kolben, T., & Burges, A. (2022). Risk of postpartum depressive symptoms is influenced by psychological burden related to the COVID-19 pandemic and dependent of individual stress coping. Archives of Gynecology and Obstetrics, 1–12. https://doi.org/10.1007/s00404-022-06854-0
Molgora, S., & Accordini, M. (2020). Motherhood in the time of Coronavirus: The impact of the Pandemic Emergency on Expectant and Postpartum women’s Psychological Well-Being. Frontiers in Psychology, 11, 567155. https://doi.org/10.3389/fpsyg.2020.567155
Nguyen, C. T. T., Sandhi, A., Lee, G. T., Nguyen, L. T. K., & Kuo, S. Y. (2023). Prevalence of and factors associated with postnatal depression and anxiety among parents of preterm infants: A systematic review and meta-analysis. Journal of Affective Disorders, 322, 235–248. https://doi.org/10.1016/j.jad.2022.11.015
Oddo-Sommerfeld, S., Schermelleh-Engel, K., Konopka, M., La Rosa, V. L., Louwen, F., & Sommerlad, S. (2022). Giving birth alone due to COVID-19-related hospital restrictions compared to accompanied birth: Psychological distress in women with caesarean section or vaginal birth - a cross-sectional study. Journal of Perinatal Medicine, 50(5), 539–548. https://doi.org/10.1515/jpm-2021-0368
Orsolini, L., Pompili, S., Mauro, A., Salvi, V., & Volpe, U. (2022). Fear and anxiety related to COVID-19 pandemic may predispose to perinatal depression in Italy. Frontiers in Psychiatry, 13, 977681. https://doi.org/10.3389/fpsyt.2022.977681
Ostacoli, L., Cosma, S., Bevilacqua, F., Berchialla, P., Bovetti, M., Carosso, A. R., Malandrone, F., Carletto, S., & Benedetto, C. (2020). Psychosocial factors associated with postpartum psychological distress during the Covid-19 pandemic: A cross-sectional study. BMC Pregnancy and Childbirth, 20(1), 703. https://doi.org/10.1186/s12884-020-03399-5
Peter, P. J., de Mola, C. L., de Matos, M. B., Coelho, F. M., Pinheiro, K. A., da Silva, R. A., Castelli, R. D., Pinheiro, R. T., & Quevedo, L. A. (2017). Association between perceived social support and anxiety in pregnant adolescents. Brazilian Journal of Psychiatry, 39(1), 21–27. https://doi.org/10.1590/1516-4446-2015-1806
Reblin, M., & Uchino, B. N. (2008). Social and emotional support and its implication for health. Current Opinions in Psychiatry, 21(2), 201–205. https://doi.org/10.1097/YCO.0b013e3282f3ad89
Redshaw, M., & Henderson, J. (2013). Fathers’ engagement in pregnancy and childbirth: Evidence from a national survey. BMC Pregnancy and Childbirth, 13(1), 70. https://doi.org/10.1186/1471-2393-13-70
Safi-Keykaleh, M., Aliakbari, F., Safarpour, H., Safari, M., Tahernejad, A., Sheikhbardsiri, H., & Sahebi, A. (2022). Prevalence of postpartum depression in women amid the COVID-19 pandemic: A systematic review and meta-analysis. International Journal of Gynaecology and Obstetrics, 157(2), 240–247. https://doi.org/10.1002/ijgo.14129
Samuel, O., & Vilter, S. (2008). La Naissance D’un enfant: Jalon biographique et perception de l’événement. Population, Vol. 62(3), 587–603. https://doi.org/10.3917/popu.703.0587
Schmitt, N., Striebich, S., Meyer, G., Berg, A., & Ayerle, G. M. (2022). The partner’s experiences of childbirth in countries with a highly developed clinical setting: A scoping review. BMC Pregnancy and Childbirth, 22(1). https://doi.org/10.1186/s12884-022-05014-1
Shuman, C. J., Peahl, A. F., Pareddy, N., Morgan, M. E., Chiangong, J., Veliz, P. T., & Dalton, V. K. (2022). Postpartum depression and associated risk factors during the COVID-19 pandemic. BMC Research Notes, 15(1), 102. https://doi.org/10.1186/s13104-022-05991-8
Sijtsma, K. (2009). On the Use, the Misuse, and the very limited usefulness of Cronbach’s alpha. Psychometrika, 74(1), 107–120. https://doi.org/10.1007/s11336-008-9101-0
Smith-Nielsen, J., Matthey, S., Lange, T., & Vaever, M. S. (2018). Validation of the Edinburgh Postnatal Depression Scale against both DSM-5 and ICD-10 diagnostic criteria for depression. Bmc Psychiatry, 18(1), 393. https://doi.org/10.1186/s12888-018-1965-7
Sommerlad, S., Schermelleh-Engel, K., La Rosa, V. L., Louwen, F., & Oddo-Sommerfeld, S. (2021). Trait anxiety and unplanned delivery mode enhance the risk for childbirth-related post-traumatic stress disorder symptoms in women with and without risk of preterm birth: A multi sample path analysis. PLoS One, 16(8), e0256681. https://doi.org/10.1371/journal.pone.0256681
Spinola, O., Liotti, M., Speranza, A. M., & Tambelli, R. (2020). Effects of COVID-19 Epidemic Lockdown on Postpartum depressive symptoms in a sample of Italian mothers. Frontiers in Psychiatry, 11, 589916. https://doi.org/10.3389/fpsyt.2020.589916
Surkan, P. J., Peterson, K. E., Hughes, M. D., & Gottlieb, B. R. (2006). The role of social networks and support in postpartum women’s depression: A multiethnic urban sample. Maternal and Child Health Journal, 10(4), 375–383. https://doi.org/10.1007/s10995-005-0056-9
Williams, M. E., Strobino, D. M., & Holliday, C. N. (2022). Measuring post-traumatic stress after childbirth: A review and critical appraisal of instruments. Journal of Reproductive and Infant Psychology, 1–15. https://doi.org/10.1080/02646838.2022.2030052
World Health Organization Regional Office for Europe, & Psychiatric Research Unit. (1998). Mastering depression in primary care. World Health Organization.
Yildiz, P. D., Ayers, S., & Phillips, L. (2017). The prevalence of post-traumatic stress disorder in pregnancy and after birth: A systematic review and meta-analysis. Journal of Affective Disorders, 208, 634–645. https://doi.org/10.1016/j.jad.2016.10.009
Zanardo, V., Manghina, V., Giliberti, L., Vettore, M., Severino, L., & Straface, G. (2020). Psychological impact of COVID-19 quarantine measures in northeastern Italy on mothers in the immediate postpartum period. International Journal of Gynaecology and Obstetrics, 150(2), 184–188. https://doi.org/10.1002/ijgo.13249
Acknowledgments
We thank the Department Project “Piano di Incentivi per la Ricerca, Pia.ce.ri” of the University of Catania.
Funding
Open access funding provided by Università degli Studi di Catania within the CRUI-CARE Agreement. The work was not supported by any fund/grant.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Valentina Lucia La Rosa. The first draft of the manuscript was written by Valentina Lucia La Rosa, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Research involving human participants and/or animals
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all subjects.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
La Rosa, V.L., Oddo-Sommerfeld, S., Schermelleh-Engel, K. et al. From lockdown to cradle: Navigating the psychological challenges of childbirth during the COVID-19 pandemic in Italy– Evidence from a 3-year analysis. Curr Psychol (2024). https://doi.org/10.1007/s12144-024-06603-3
Accepted:
Published:
DOI: https://doi.org/10.1007/s12144-024-06603-3