
Abstract
The purpose of this study was to examine the reliability and validity of the Turkish version of the Brief Suicide Cognitions Scale (BSCS-T) and to explore the mediating role of emotional problems in the relationship between psychological vulnerability and suicide cognitions and quality of life among Turkish young adults. Participants were 418 students in Türkiye. The sample included 181 female (43.3%) and 237 male (56.7%) students aged 18–35 years (mean = 22.86, SD = 3.03). The results provided evidence to support the use of the BSCS-T as a means of identifying young people at high risk of suicide. Furthermore, the results showed that psychological vulnerability significantly and positively predicted emotional problems and suicidal cognitions among college students. In addition, psychological vulnerability negatively predicted students’ quality of life, and emotional problems played a mediating role between psychological vulnerability and both suicide cognitions and quality of life. These findings highlight the need for targeted interventions to reduce suicide risk and improve psychological well-being. Further research in this area can contribute to suicide prevention efforts and the development of effective strategies to support at-risk individuals in college settings.
Similar content being viewed by others


Suicide is a significant public health problem that poses a serious threat to human life. According to the World Health Organization, suicide accounts for more than 800,000 deaths worldwide each year. It is also a leading cause of death among young adults aged 15–29 years (WHO, 2023). While suicide rates are high in some countries, they are relatively low in others, such as Turkey. In 2023, Turkey recorded its highest crude suicide rate ever at 4.94 per 100,000 (Karkın & Eskin, 2023). Mental health professionals are particularly concerned about this significant increase in suicide rates in the country. Therefore, studies need to be conducted to develop protective and preventive factors for suicide. These factors have been identified and explained through various suicide models and approaches (e.g., Baumeister, 1990; Schneidman, 1998; Van Orden et al., 2010).
One of the approaches to understanding suicide is the fluid vulnerability theory (Rudd, 2006), which builds on Beck’s (1996) cognitive theory and focuses on cognitive issues. According to this theory, while all individuals possess a suicidal belief system, some individuals are more vulnerable to suicide than others. Rudd (2006) argues that suicidality results from suicide cognitions embedded in the suicide belief system. Suicidal ideation involves the planning stage, while suicide cognition encompasses acute and chronic life events, including suicidal ideation (Rudd, 2010). The outlined suicide cognitions have been defined by the subdimensions of unlovability and unbearability, which form the core of suicide cognitions (Gibbs, 2010). In addition, Ellis and Rufino (2015) distinguish three subdimensions of suicide cognitions: unlovability, unsolvability, and unbearability. Unlovability refers to feelings of inadequacy and unworthiness, unsolvability involves the belief that life problems are unsolvable, and unbearability refers to the inability to cope with stress and difficulties.
In contrast to resilience (Arslan & Wong, 2024; Khalaf et al., 2020; Khalaf & Al-Said, 2021), which is also referred to as invulnerability (Satici, 2016), intolerability is characterized as a concept that shares similarities with psychological vulnerability (Christophers et al., 2021). The term “psychological vulnerability” was coined by Sinclair and Wallston (1999) and refers to “the pattern of cognitive beliefs that reflect the individual’s reliance on achievement or external sources of approval for a sense of self-worth.” Vulnerable individuals are more susceptible to psychopathology and are easily triggered by stressful or adverse events (Papmeyer et al., 2016). Psychological vulnerability is also an important factor that increases the risk of suicide (Barros et al., 2020). The Integrated Motivational Volitional (IMV) model (O’Connor & Kirtley, 2018), one of the suicide models, explains that individuals are more vulnerable to suicide due to their biological, genetic, and cognitive characteristics. When vulnerability is combined with negative family and environmental conditions, individuals may lose the ability to endure, leading them to view suicide as an escape from difficulties (Bonfanti et al., 2022).
Emotional problems are one of the challenges that individuals face (Arslan, 2021), and they are associated with psychological vulnerability (Kaur et al., 2018). Psychologically vulnerable individuals experience emotional problems more quickly and easily (Manna et al., 2016). These emotional problems refer to difficulties in regulating and experiencing emotions, and they significantly impact an individual’s well-being and functioning (Eisenberg et al., 2001). Internalizing and externalizing problems are two types of emotional problems that are defined as developmental problems with behavioral dimensions (Arslan, 2019). Externalizing problems are outwardly focused, such as aggression, hyperactivity, and conduct problems, whereas internalizing problems are inwardly focused, such as withdrawal, anxiety, and psychosomatic symptoms (Arslan, 2023; Achenbach et al., 2016; Lyons et al., 2014). Depression, anxiety, and somatization, all internalized behaviors, are major risk factors for suicide (Donnelly et al., 2021; Soto-Sanz et al., 2019). Depressed individuals may develop a perception that they are unlovable due to feelings of inadequacy and decreased self-worth (Wiblin et al., 2021). Individuals with anxiety (e.g., situational, persistent) and severe somatization symptoms may have weakened endurance (Tacchini & Vismara, 2019). The activation of suicidal cognitions by these situations makes the individual’s life dysfunctional and reduces life satisfaction (Nock et al., 2009). The lack of life satisfaction negatively affects the individual’s quality of life (Vinsalia & Handajani, 2021).
The concept of quality of life is multidimensional, encompassing various aspects of well-being and satisfaction with different domains of life. Psychological functioning is one of the most important predictors of QoL (Fteropoulli et al., 2013; Murgaš et al., 2022). Individuals with high quality of life are more resilient to challenging life events as their well-being increases (Rink et al., 2022). Resilience strengthens self-esteem, and individuals’ perceptions of being lovable are enhanced (Yang et al., 2020). Resilient individuals also view problems as solvable and use effective coping strategies (Chen, 2016). Quality of life has a protective effect on suicide based on the relationships among quality of life, resilience, lovability, and solvability (Le et al., 2023). Several studies have examined the relationship between suicide and quality of life and found a negative significant association between quality of life and suicidal ideation and behavior (Melo et al., 2022). Accordingly, interventions that improve quality of life may effectively prevent suicide and promote resilience by helping individuals cope with and manage suicidal cognitions.
Present Study
Based on Rudd’s (2006) fluid vulnerability theory, activating life events are thought to trigger suicide cognitions in vulnerable individuals. According to the theory, suicidal cognition and behavior are characterized by chronic identity-based perceptual beliefs (Rudd, 2006). Therefore, the structure of psychological vulnerability, including persistent cognitive beliefs about achievement and external evaluation, can be compared to the structure of suicidal behavior. Suicidal individuals with psychological vulnerability typically have emotional problems and a low quality of life (Alves et al., 2016; Martínez-Monteagudo et al., 2020). Individuals’ psychological vulnerability may lead to emotional problems in the face of challenging or traumatic events, resulting in low quality of life and suicidal ideation. While many studies have examined the relationship between psychological vulnerability, emotional problems, quality of life, and suicidal thoughts and behaviors (Gruber et al., 2021; Xiao et al., 2019), few have examined how these variables influence suicidal cognitions. Therefore, it is imperative to examine the factors associated with suicide cognitions in order to develop effective intervention strategies to promote mental health and well-being.
In this study, we had two primary objectives. First, we examined the reliability and validity of the Turkish version of the Brief Suicide Cognitions Scale. Second, we examined the mediating role of emotional problems in psychological vulnerability and suicide cognitions and quality of life in young adults. The research hypotheses were structured as follows: (i) B-SCS will show adequate psychometric properties in Turkish; (ii) Psychological vulnerability will have a direct effect on emotional problems, quality of life, and suicide cognitions; (iii) Emotional problems and quality of life will have a direct effect on suicide cognitions; (iv) Emotional problems will mediate the relationship between psychological vulnerability and quality of life, and (v) Emotional problems will mediate the relationship between psychological vulnerability and suicide cognitions.
Method
Participants
Participants in this study were undergraduate college students from a state university in Türkiye. A total of 418 students (181 females, 237 males) volunteered to participate in the study. The age range of the participants was between 18 and 41 years, with a mean age of 22.86 years (SD = 3.03). Since the majority of students were between the ages of 20 and 35 (approximately 97%), the participants in this study were generally defined by the concept of young adults. Convenience sampling involves selecting participants based on their availability and accessibility, such as students who are easily accessible in a particular setting, rather than through a random method. In this study, students at a state university were invited to participate in the study. A web-based survey was developed, comprising demographic items and study measures. Participants were informed about the purpose and procedures of the study and provided informed consent before participating. To maintain anonymity and confidentiality, each participant was assigned a unique identification number, and their personal information was kept separate from their survey responses.
Measures
Suicide Cognitions
The Brief Suicide Cognitions Scale (BSCS) was employed to measure suicidal thoughts and beliefs (Rudd & Bryan, 2021). The scale comprises six items, and participants rated each item on a 5-point Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree). The total score on the scale ranges from 6 to 30, with higher scores indicating a greater level of suicide cognition. Despite previous examinations of the long version of the scale, which is a 16-self-report scale, with Turkish people (Bekaroğlu et al., 2024), the current version’s validity and reliability have not been assessed specifically for college students. Hence, this study aimed to evaluate the psychometric properties of the BSCS to improve its suitability for research and practical use among college students. The Turkish version of the BSCS was developed using a translation and back-translation process (Hernández et al., 2020). By following the translation and back-translation steps, the Turkish version of the BSCS was created. In light of the results, the BSCS can be concluded that it is a psychometrically valid and reliable instrument for evaluating suicide thoughts and beliefs among young adults in Türkiye.
Quality of life
Quality of life was assessed using a three-item scale, which measured participants’ physical health, social relationships, and overall quality of life (Arslan, 2024). Responses were rated on a 5-point scale, ranging from 0 (poor) to 5 (excellent). To obtain the overall quality of life score, the scores from these three questions were summed.
Emotional problems
Emotional problems were assessed using the Brief Symptom Inventory (BSI-18; Derogatis and Fitzpatrick in 2004). This self-report measure consists of 18 items, divided into three six-item subscales: depression, anxiety, and somatization. Participants were asked to rate the extent to which they experienced each symptom on a 5-point Likert scale, ranging from “not at all” (0) to “very much” (4). The scale and its subscales have demonstrated strong internal reliability (α) estimates in previous research with a Turkish sample (Arslan et al. 2022).
Psychological vulnerability
Psychological vulnerability was assessed using the Psychological Vulnerability Scale (PVS) developed by Sinclair and Wallston in 1999. The PVS consists of 6 items, and participants responded to each item on a 5-point Likert scale, ranging from “Unsuitable to me” (1) to “Suitable to me” (5). Higher scores on the scale indicate higher levels of psychological vulnerability. Akin and Eker (2011) reported that the Turkish version of the PVS demonstrated an acceptable internal reliability (α) estimate.
Data analyses
To examine the structural validity of responses to the BSCS-T, confirmatory factor analysis (CFA) was performed using the maximum likelihood estimator. Factor loadings (λ) greater than or equal to 0.50 were considered strong, indicating that they account for at least 25% of the variance extracted fit indices. Fit indices such as the comparative fit index (CFI), goodness of fit index (GFI), and Tucker Lewis index (TLI) values ranging from 0.90 to 0.95, as well as root mean square error of approximation (RMSEA) and standardized root mean square residual (SRMR) values between 0.05 and 0.08, were considered indicative of adequate data-model fit (Hooper et al., 2008). Latent construct reliability coefficients (H) of 0.70 or higher, similar to internal consistency coefficients derived from observed scores, were also desirable. After establishing the structural validity of the BSCS-T responses, descriptive analyses were conducted to explore the observed characteristics of scores derived from the measure.
Next, the association between BSCS-T scores and concurrent variables was investigated through two phases of analyses. To begin, a sequence of bivariate correlation analyses was performed examining the associations between suicide cognitions and psychological vulnerability, emotional problems, and quality of life. Secondly, a series of independent samples t-tests were conducted to examine differences in these outcomes based on the presence of suicide cognitions, which were defined using the recommended BSCS cutoff score (≥ 13) for identifying individuals at risk for suicide. Rudd and Bryan (2021) proposed this cutoff score to identify persistent suicide risk. Therefore, we divided students into two groups (at-risk and non-risk). The Bonferroni correction was also used to reduce the probability of Type I error. The effect sizes for these between-group differences were evaluated using Cohen’s effect size (d) with the ranges: small (0.20-0.49), moderate (0.50-0.79), and large (0.80 or more) (Cohen, 1988). Finally, a structural equation model was conducted to examine the mediating role of emotional problems in the relationship between psychological vulnerability and suicide cognitions, as well as quality of life among college students. Prior to testing the model, the assumptions of structural equation analysis were examined, such as normality, missing date (Kenny et al., 2015; Kline, 2015). Skewness and kurtosis scores were examined to assess the assumption of normality. The same data-model fit indices were also utilized to evaluate the outcomes of the structural model. Additionally, it was employed the bootstrap approach with 5000 resamples to estimate the confidence intervals (95% CI). All data analyses were performed using SPSS v27 and AMOS v24.
Results
Factor analyses
Findings from the baseline CFA using the maximum likelihood estimator for the BSCS-T measurement model, which structured each of the six items as indicators of a single latent structure (representing overall suicide cognitions), provided mixed data–model fit statistics, with some indices indicating poor fit and others indicating adequate fit (χ2 = 74.30, df = 9, p < .001, CFI = 0.94, TLI = 0.90, GFI = 0.94, SRMR = 0.046, RMSEA [90% CI] = 0.132 [0.105, 0.160]). In order to improve the data–model fit statistics, a procedure was conducted to redefine the measurement model. Although using the RMSEA to evaluate the model fit with a small degree of freedom (df) can indicate a poor fit (Kenny et al., 2015), further analyses were carried out to achieve a better fit between the data and the model. This involved examining specific parameters in the model that were contributing to a suboptimal fit of the data (Byrne, 2001; Kenny, 2011). Initially, the factor loadings and error variances were assessed and found to be acceptable, indicating that items were functioning adequately (see Table 1). Additionally, modification indices were examined to identify potential correlations between sets of item errors. Based on this review, it was found that incorporating a covariance between the error terms of items BSCS4 and BSCS3 would significantly enhance the data–model fit. Results from this respecified measurement model indicated better data–model fit across all indices (χ2 = 46.22, df = 8, p < .001, CFI = 0.97, TLI = 0.94, GFI = 0.96, SRMR = 0.035, RMSEA [90% CI] = 0.107 [0.078, 0.138]).
After redefining the model, we examined the modification indices to determine if additional covariances between item error terms were needed to further improve the measurement model. The analysis revealed that including an additional covariance between the error terms of items BSCS5 and BSCS6 would enhance the fit between the data and the model. Consequently, we revised the measurement model and re-ran the CFA, which resulted in an even better data-model fit (χ2 = 29.43, df = 7, p < .001, CFI = 0.98, TLI = 0.96, GFI = 0.98, SRMR = 0.031, RMSEA [90% CI] = 0.088 [0.056, 0.122]). As no further parameter changes were found to be justified based on empirical and conceptual reasons, this particular model was considered the most suitable measurement model for the BSCS-T in the current sample. Additional findings from the model indicated that the factor loadings for both factors were robust, ranging from 0.53 to 0.87, and that the reliability coefficients for the latent construct were strong (H = 0.88).
Descriptive statistics and correlation results
Following determining the optimal measurement model for the BSCS-T, descriptive characteristics of all measures used in the study were examined. The findings indicated that all measures demonstrated relatively normal distributions (see Table 2). The measures also had adequate-to-strong internal reliability (α) estimates. Once these assumptions were verified, concurrent validity analyses were deemed appropriate. The results from the bivariate correlations, which is statistical measures used to assess the relationship between two variables, used to show relationships between variables. It revealed that the observed scores on the BSCS-T showed positive associations with psychological vulnerability, depressive symptoms, anxiety, and somatization. Additionally, the BSCS-T displayed negative relationships with social relationships, physical health, and quality of life, as seen in Table 3.
Furthermore, the independent samples t-tests showed significant differences between young adults classified as at-risk for suicide (BSCS-T scores ≥ 13) and those classified as non-risk (BSCS-T scores < 13). These differences were characterized by statistically significant effects with small-to-large effect sizes for each of the other concurrent outcomes. Moreover, 28.2% of the young adults (118) who had 13 and higher scores were identified as at risk for suicide. At-risk young adults for suicide experienced higher levels of depression, anxiety, somatization, and psychological vulnerability and lower levels of physical health, positive social relationships, and quality of life, as shown in Table 4.
Structural equation model
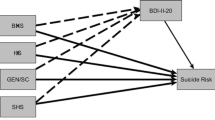
A structural equation model was tested to investigate the mediating role of emotional problems in the relationship between psychological vulnerability and suicide cognitions, as well as quality of life among college students. The latent structures were defined using the items and subscales of the scales. Prior to testing the model, the measurement model was assessed, revealing adequate data-model fit statistics: χ2 = 403.23, df = 127, p < .001, CFI = 0.91, TLI = 0.90, SRMR = 0.068, RMSEA [90% CI] = 0.072 [0.064, 0.080]. Subsequently, the structural equation model was conducted, yielding a similar data-model fit. The standardized regression weights indicated that psychological vulnerability had a significant and positive predictive effect on emotional problems and suicide cognitions, as well as a positive predictive effect on quality of life among college students, as seen in Fig. 1. Emotional problems were found to be a significant and positive predictor of suicide cognitions, and a negative predictor of quality of life. Furthermore, they mediated the relationship between psychological vulnerability and both emotional problems and quality of life in college students. The results also demonstrated that quality of life significantly and negatively predicted suicide cognitions among students, mediating the link between psychological vulnerability and suicide. Overall, these findings highlight the importance of addressing psychological vulnerability and emotional problems in college students’ well-being. They also emphasize the significance of promoting a positive quality of life to reduce suicide risk and enhance the overall mental health of college students.

the proposed model indicating the association between the variables of the study
Discussion
The purpose of this study was to examine the reliability and validity of the Turkish version of the BSCS and test the mediating role of emotional problems in the link between psychological vulnerability and suicide cognitions, as well as quality of life in a sample of Turkish young adults. Overall, the results provide evidence supporting the use of the BSCS-T as a tool for identifying at-risk young adults for suicide, justifying the provision of interventions and support in college settings. The analyses on structural validity demonstrated that the BSCS-T can be described by a single-factor measurement model, aligning with the latent structure of the English version (Rudd & Bryan, 2021). However, it should be noted that two covariances were added between sets of item error terms to enhance the model’s performance. Similar to these findings, Rudd and Bryan (2021) reported satisfactory data-model fit statistics after incorporating three additional covariances (BSCS1 and BSCS4, BSCS3 and BSCS4, and BSCS2 and BSCS6). Furthermore, the results of the concurrent validity analyses revealed significant associations between the responses to the BSCS-T and various concurrent outcomes that are consistent with relevant theoretical constructs. Specifically, young adults classified as at-risk for suicide exhibited higher levels of psychological vulnerability, depressive symptoms, anxiety, and somatization, while also reporting lower levels of quality of life indicators. Collectively, these findings offer support for utilizing the BSCS-T as a means of identifying young adults who are at risk for suicide, underscoring the importance of implementing interventions and providing support specifically tailored for this population within college settings (Arango et al., 2021).
The present study has several limitations that should be addressed in future studies. The study used a cross-sectional approach in which participants reported on a single time period, which may introduce bias. In addition, the use of a cross-sectional method limits the inferences that can be made about causality between the variables analyzed or over time. The structure and eligibility criteria of the sample prevent generalization of emerging findings to the general population. The use of convenience samples from an online survey limits the generalizability of findings to other populations because the sample is not representative of other populations. Therefore, future research could be conducted using other sampling methods, such as convenience sampling, to gain a more complete understanding of these variables. The study did not exclude participants based on clinical diagnosis, which is critical to understanding participant demographics and the potential applicability of findings to clinically diagnosed populations. Future research could examine the association between variables using clinical samples. Finally, this study used self-report measures. Self-report measures, in which participants overestimate or underestimate their responses, often produce either negative or positive attitudes as a result of social desirability. The validity of the current findings may be enhanced by the use of additional methods (e.g., longitudinal studies).
Subsequent results have shown that psychological vulnerability has a significant and positive impact on emotional distress and suicidal ideation among college students. This suggests that individuals with higher levels of psychological vulnerability are more likely to experience emotional distress and have suicidal thoughts. Psychological vulnerability also has a negative impact on college students’ quality of life, suggesting that individuals with higher levels of psychological vulnerability may have a lower overall quality of life, possibly due to the challenges and distress associated with their psychological state. Psychological vulnerability, a type of cognitive vulnerability characterized by dependency, perfectionism, and the need for external approval (Sinclair & Wallston, 1999), can lead people to feel overwhelmed, insecure, and anxious, making it difficult for them to manage their emotions and vulnerable to developing emotional problems such as depression, anxiety, and somatization. Accordingly, several studies have shown that psychological vulnerability is positively correlated with emotional problems (e.g., depression, anxiety, and somatization), suggesting that individuals who experience higher levels of psychological vulnerability are more likely to suffer from emotional problems (Kaur et al., 2018). Similarly, one study found that psychological vulnerability predicted an increase in depressive symptoms (Sinclair & Wallston, 2010). In addition, another study found that psychologically vulnerable individuals who fear negative evaluations are more likely to develop social anxiety (Rodebaugh et al., 2017). These individuals may also experience depression, anxiety, or somatization disorders due to the distress that causes emotional problems (Terluin et al., 2006). The presence of emotional problems and psychological vulnerability is associated with an increased risk of suicidal ideation (Barros et al., 2020; Kaur et al., 2018). A review of empirical studies on psychological vulnerability to suicide conducted by Conner et al. (2001) found that psychological factors such as aggression, depression, anxiety, and hopelessness are consistently associated with completed suicide.
Emotional problems play a mediating role between psychological vulnerability and both suicide cognitions and quality of life. This suggests that emotional problems partially explain the relationship between psychological vulnerability and adverse outcomes by acting as a mediating factor. The findings of Klonsky et al. (2013) provide support for this finding by examining the relationship between non-suicidal self-injury (NSSI) and suicide attempts. Their results indicate that emotional problems are a mediator between NSSI and suicide attempts. Therefore, it is reasonable to conclude that emotional problems are associated with an increased risk of suicide attempts among individuals with psychological vulnerability. Furthermore, Ribeiro et al. (2016) examined the longitudinal relationship between self-injurious thoughts and behaviors (SITBs) and future suicidal ideation, suicide attempts, and death. Results indicated that emotional problems mediated the relationship between SITBs and subsequent suicide attempts. The results of this study suggest that emotional problems play an important role in the progression from self-injurious thoughts, behaviors, and outcomes to more severe suicidal outcomes. In addition, one study found that cancer patients with higher levels of psychological vulnerability tend to experience emotional difficulties more often than those with lower levels. They also have a lower quality of life than other cancer patients (Bachmann et al., 2018).
Quality of life has a significant negative impact on suicidal ideation among college students. These findings suggest that individuals with higher quality of life tend to have fewer suicide-related thoughts, while those with lower quality of life may be more susceptible to such thoughts (Alves, 2016). Studies have reported that lower quality of life is associated with higher levels of suicidal ideation and behavior in both clinical and nonclinical samples (Cerutti et al., 2018; Pisula et al., 2015). Skegg (2005) conducted a comprehensive review of self-harm, which is closely related to suicidal ideation. It was found that self-harm is often associated with poor quality of life, including factors such as social isolation, relationship problems, and low self-esteem. As a result of these factors, suicidal thoughts and behaviors may develop, suggesting that quality of life may negatively influence suicide cognitions. In conclusion, quality of life has a significant negative impact on suicide cognition among college students. A lower quality of life is associated with higher levels of suicidal ideation and behavior, while a higher quality of life is associated with fewer suicide-related thoughts. Addressing and improving quality of life is critical to preventing suicide and promoting mental well-being among college students. These findings underscore the importance of developing therapies that focus on emotional problems to reduce suicide-related thoughts, feelings, and actions. For example, mental health practitioners may have the opportunity to utilize the emotional problem-focused approach throughout the therapy process. In addition, individuals with high levels of psychological vulnerability can be prioritized as a sample for these programs. Improving quality of life and increasing coping strategies with emotional problems in interventions may have a buffering effect on the relationship between psychological vulnerability and suicide cognitions. School-based prevention and intervention programs may also be beneficial for parents, adolescents, and educators. Future research may benefit from further investigation of the factor structure of the measure using diverse samples, as this may provide additional insight and ensure the generalizability of the findings.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Achenbach, T. M., Ivanova, M. Y., Rescorla, L. A., Turner, L. V., & Althoff, R. R. (2016). Internalizing/externalizing problems: Review and recommendations for clinical and research applications. Journal of the American Academy of Child & Adolescent Psychiatry, 55(8), 647–656. https://doi.org/10.1016/j.jaac.2016.05.012
Akın, A., & Eker, H. (2011). Turkish version of the psychological vulnerability scale: A study of validity and reliability. Paper presented at the 32th international conference of the stress and anxiety research society (STAR), July, 18–20, Munster, Germany.
Alves, V. D. M., Francisco, L. C. F. D. L., Belo, F. M. P., de-Melo-Neto, V. L., Barros, V. G., & Nardi, A. E. (2016). Evaluation of the quality of life and risk of suicide. Clinics, 71, 135–139. https://doi.org/10.6061/clinics/2016(03)03
Arango, A., Gipson, P. Y., Votta, J. G., & King, C. A. (2021). Saving lives: Recognizing and intervening with youth at risk for suicide. Annual Review of Clinical Psychology, 17, 259–284. https://doi.org/10.1146/annurev-clinpsy-081219-103740
Arslan, G. (2019). Development and validation of the Youth Externalizing Behavior Screener: A brief and effective measure of behavioral problems. International Journal of School & Educational Psychology, 7(sup1), 64–74.
Arslan, G. (2021). Measuring emotional problems in Turkish adolescents: Development and initial validation of the Youth Internalizing Behavior Screener. International Journal of School & Educational Psychology, 9(2), 198–207.
Arslan, G. (2023). Dysfunctional parenting and emotional problems and substance misuse: Enhancing psychological flexibility in college students. Journal of Ethnicity in Substance Abuse. https://doi.org/10.1080/15332640.2023.2237930
Arslan, G. (2024). Unlocking the Power of Self-Compassion and Psychological Flexibility: Enhancing Emotional Health, Subjective Wellbeing, and Quality of Life in College Students. Studia Psychologica, 66(1), 50–65. https://doi.org/10.31577/sp.2024.01.890
Arslan, G., & Wong, P. (2024). Embracing life’s challenges: Developing a tool for assessing resilient mindset in second wave positive psychology. Journal of Happiness and Health, 4(1), 1–10. https://doi.org/10.47602/johah.v4i1.53
Arslan, G., Yıldırım, M., Karataş, Z., Kabasakal, Z., & Kılınç, M. (2022). Meaningful Living to Promote Complete Mental Health Among University Students in the Context of the COVID-19 Pandemic. International Journal of Mental Health and Addiction, 20(2), 930–942. https://doi.org/10.1007/s11469-020-00416-8
Bachmann, A. S., Zaunbauer, A. C., Tolke, A. M., Siniatchkin, M., Kluck, C., Wiltfang, J., & Hertrampf, K. (2018). Well-being and quality of life among oral cancer patients–psychological vulnerability and coping responses upon entering initial treatment. Journal of Cranio-Maxillofacial Surgery, 46(9), 1637–1644. https://doi.org/10.1016/j.jcms.2018.05.042
Barros, J., Morales, S., García, A., Echávarri, O., Fischman, R., Szmulewicz, M., & Tomicic, A. (2020). Recognizing states of psychological vulnerability to suicidal behavior: A bayesian network of artificial intelligence applied to a clinical sample. Bmc Psychiatry, 20(1), 1–20. https://doi.org/10.1186/s12888-020-02535-x
Baumeister, R. F. (1990). Suicide as escape from self. Psychological Review, 97(1). https://doi.org/10.1037/0033-295X.97.1.90
Beck, A. T. (1996). Beyond belief: A theory of modes, personality, and psychopathology. In P. M. Salkovskis (Ed.), Frontiers of cognitive therapy (pp. 1–25). Guilford Press.
Bekaroğlu, E., Bulut, B. P., & Demirbaş, H. (2024). Reliability and validity of the Suicide Cognitions Scale-Revised (SCS-R) in emerging adulthood in Turkey. Death Studies, 48(5), 500–510. https://doi.org/10.1080/07481187.2023.2240742
Bonfanti, S., Chen, S., & Massa, A. (2022). Vulnerable homes on the move: An introduction. Focaal, 2022(92), 1–14. https://doi.org/10.3167/fcl.2022.920101
Byrne, B. M. (2001). Structural equation modeling with AMOS, EQS, and LISREL: Comparative approaches to testing for the factorial validity of a measuring instrument. International Journal of Testing, 1(1), 55–86. https://doi.org/10.1207/S15327574IJT0101_4
Cerutti, R., Zuffianò, A., & Spensieri, V. (2018). The role of difficulty in identifying and describing feelings in non-suicidal self-injury behavior (NSSI): Associations with perceived attachment quality, stressful life events, and suicidal ideation. Frontiers in Psychology, 9, 318. https://doi.org/10.3389/fpsyg.2018.00318
Chen, C. (2016). The role of resilience and coping styles in subjective well-being among Chinese university students. The Asia-Pacific Education Researcher, 25, 377–387. https://doi.org/10.1007/s40299-016-0274-5
Christophers, B., Nieblas-Bedolla, E., Gordon-Elliott, J. S., Kang, Y., Holcomb, K., & Frey, M. K. (2021). Mental health of US medical students during the COVID-19 pandemic. Journal of General Internal Medicine, 36, 3295–3297. https://doi.org/10.1007/s11606-021-07059-y
Cohen, J. (1988). Statistical power analysis for the behavioralsciences. Lawrence Erlbaum.
Conner, K. R., Duberstein, P. R., Conwell, Y., Seidlitz, L., & Caine, E. D. (2001). Psychological vulnerability to completed suicide: A review of empirical studies. Suicide and Life-Threatening Behavior, 31(4), 367–385. https://doi.org/10.1521/suli.31.4.367.22048
Donnelly, H. K., Richardson, D., & Solberg, S. V. (2021). Understanding somatic symptoms associated with South Korean adolescent suicidal ideation, depression, and social anxiety. Behavioral Sciences, 11(11), 151. https://doi.org/10.3390/bs11110151
Eisenberg, N., Cumberland, A., Spinrad, T. L., Fabes, R. A., Shepard, S. A., Reiser, M., Murphy, B. C., Losoya, S. H., & Guthrie, I. K. (2001). The relations of regulation and emotionality to children’s externalizing and internalizing problem behavior. Child Development, 72(4), 1112–1134. https://doi.org/10.1111/1467-8624.00337
Ellis, T. E., & Rufino, K. A. (2015). A psychometric study of the suicide cognitions Scale with psychiatric inpatients. Psychological Assessment, 27(1), 82. https://doi.org/10.1037/pas0000028
Fteropoulli, T., Stygall, J., Cullen, S., Deanfield, J., & Newman, S. P. (2013). Quality of life of adult congenital heart disease patients: A systematic review of the literature. Cardiology in the Young, 23(4), 473–485. https://doi.org/10.1017/s1047951112002351
Gibbs, D. (2010). Assessing suicidal cognitions in adolescents: Establishing the reliability and validity of the Suicide Cognitions Scale. (Unpublished doctoral thesis). Toledo University.
Gruber, J., Prinstein, M. J., Clark, L. A., Rottenberg, J., Abramowitz, J. S., Albano, A. M., & Weinstock, L. M. (2021). Mental health and clinical psychological science in the time of COVID-19: Challenges, opportunities, and a call to action. American Psychologist, 76(3), 409. https://doi.org/10.1037/amp0000707
Hernández, A., Hidalgo, M. D., Hambleton, R. K., & Gómez-Benito, J. (2020). International Test Commission guidelines for test adaptation: A criterion checklist. Psicothema, 32(3), 390–398. https://doi.org/10.7334/psicothema2019.306
Hooper, D., Coughlan, J., & Mullen, M. R. (2008). Structural equation modelling: Guidelines for determining model fit. Electronic Journal of Business Research Methods, 6(1), 53–60. https://doi.org/10.21427/D7CF7R
Karkın, A. N., & Eskin, M. (2023). Prevalence, correlates, and risk factors of suicidal ideation and attempts in Turkey. Neuropsychiatric Investigation, 61(1). https://doi.org/10.5152/NeuropsychiatricInvest.2023.22019
Kaur, R., Vinnakota, A., Panigrahi, S., & Manasa, R. V. (2018). A descriptive study on behavioral and emotional problems in orphans and other vulnerable children staying in institutional homes. Indian Journal of Psychological Medicine, 40(2), 161–168. https://doi.org/10.4103/ijpsym.ijpsym_316_17
Kenny, D. A. (2011). SEM: model respecification (David A. Kenny). Respecification of Latent Variable Models. https://davidakenny.net/cm/respec.htm
Kenny, D. A., Kaniskan, B., & McCoach, D. B. (2015). The performance of RMSEA in models with small degrees of freedom. Sociological Methods & Research, 44(3), 486–507. https://doi.org/10.1177/0049124114543236
Khalaf, M. A. (2020). Psychological consequences of COVID-19 and challenges for post-traumatic interventions. Psychology Research, 10(1), 24–29. https://doi.org/10.17265/2159-5542/2020.01.003
Khalaf, M. A., & Al-Said, T. T. (2021). The Egyptian validation study of the resilience scale for adults (RSA) and its utility in predicting depression. The Open Psychology Journal, 14, 83–92. https://doi.org/10.2174/1874350102114010083
Kline, R. B. (2015). Principles and practice of structural equation modeling (4th ed.). Guilford Press.
Klonsky, E. D., May, A. M., & Glenn, C. R. (2013). The relationship between nonsuicidal self-injury and attempted suicide: Converging evidence from four samples. Journal of Abnormal Psychology, 122(1), 231. https://doi.org/10.1037/a0030278
Le, N., Belay, Y. B., Le, L. K., Pirkis, J., & Mihalopoulos, C. (2023). Health-related quality of life in children, adolescents and young adults with self-harm or suicidality: A systematic review. The Australian and New Zealand Journal of Psychiatry, 57, 952–965. https://doi.org/10.1177/00048674231165477
Lyons, M. D., Otis, K. L., Huebner, E. S., & Hills, K. J. (2014). Life satisfaction and maladaptive behaviors in early adolescents. School Psychology Quarterly, 29(4), 553–566. https://doi.org/10.1037/spq0000061
Manna, G., Falgares, G., Ingoglia, S., Como, M. R., & De Santis, S. (2016). The relationship between self-esteem, depression and anxiety: Comparing vulnerability and scar model in the Italian context. Mediterranean Journal of Clinical Psychology, 4(3). https://doi.org/10.6092/2282-1619/2016.4.1328
Martínez-Monteagudo, M. C., Delgado, B., Díaz-Herrero, Á., & García-Fernández, J. M. (2020). Relationship between suicidal thinking, anxiety, depression and stress in university students who are victims of cyberbullying. Psychiatry Research, 286, 112856. https://doi.org/10.1016/j.psychres.2020.112856
Melo, C. D. F., Filho, V., Costa, J. E. D., Cavalcante, I. M., Silva, A. K. S., M. D., S. M., & Freitas Filho, R. A. D. (2022). Assessment and associations between quality of life and risk of suicide. Psico-USF, 27, 61–72. https://doi.org/10.1590/1413-82712022270105
Murgaš, F., Petrovič, F., & Tirpáková, A. (2022). Social capital as a predictor of quality of life: The Czech experience. International Journal of Environmental Research and Public Health, 19(10), 6185. https://doi.org/10.3390/ijerph19106185
Nock, M. K., Hwang, I., Sampson, N., Kessler, R. C., Angermeyer, M., Beautrais, A., & Williams, D. R. (2009). Cross-national analysis of the associations among mental disorders and suicidal behavior: Findings from the WHO World Mental Health Surveys. PLoS Medicine, 6(8), e1000123. https://doi.org/10.1371/journal.pmed.1000123
O’Connor, R. C., & Kirtley, O. J. (2018). The integrated motivational-volitional model of suicidal behaviour. Philosophical Transactions of the Royal Society B: Biological Sciences, 373(1754), 20170268. https://doi.org/10.1098/rstb.2017.0268
Pisula, E., Danielewicz, D., Kawa, R., & Pisula, W. (2015). Autism spectrum quotient, coping with stress and quality of life in a non-clinical sample–an exploratory report. Health and Quality of Life Outcomes, 13(1), 1–9. https://doi.org/10.1186/s12955-015-0370-x
Ribeiro, J. D., Franklin, J. C., Fox, K. R., Bentley, K. H., Kleiman, E. M., Chang, B. P., & Nock, M. K. (2016). Self-injurious thoughts and behaviors as risk factors for future suicide ideation, attempts, and death: A meta-analysis of longitudinal studies. Psychological Medicine, 46(2), 225–236. https://doi.org/10.1017/S0033291715001804
Rink, L. C., Silva, S. G., Adair, K. C., Oyesanya, T. O., Humphreys, J. C., & Sexton, J. B. (2022). The association between well-being behaviors and resilience in health care workers. Western Journal of Nursing Research, 44(8), 743–754. https://doi.org/10.1177/01939459211017515
Rodebaugh, T. L., Levinson, C. A., Langer, J. K., Weeks, J. W., Heimberg, R. G., Brown, P. J., & Liebowitz, M. R. (2017). The structure of vulnerabilities for social anxiety disorder. Psychiatry Research, 250, 297–301. https://doi.org/10.1016/j.psychres.2017.01.073
Rudd, M. D. (2006). Fluid vulnerability theory: A cognitive approach to understanding the process of acute and chronic suicide risk. In T. E. Ellis (Ed.), Cognition and suicide: Theory, research, and therapy (pp. 355–368). American Psychological Association. https://doi.org/10.1037/11377-016
Rudd, M. D., & Bryan, C. J. (2021). The brief suicide cognitions Scale: Development and clinical application. Frontiers in Psychiatry, 12, 737393. https://doi.org/10.3389/fpsyt.2021.737393
Rudd, M. D., Schmitz, B., McClenen, R., Joiner, T., Elkins, G., & Claassen, C. (2010). The suicide cognitions Scale: A suicidespecific measure of hopelessness. Journal of Abnormal Psychology.
Satici, S. A. (2016). Psychological vulnerability, resilience, and subjective well-being: The mediating role of hope. Personality and Individual Differences, 102, 68–73. https://doi.org/10.1016/j.paid.2016.06.057
Schneidman, E. S. (1998). Perspectives on suicidology: Further reflections on suicide and psychache. Suicide and Life-Threatening Behavior, 28(3), 245.
Sinclair, V. G., & Wallston, K. A. (1999). The development and validation of the psychological vulnerability scale. Cognitive Therapy and Research, 23(2), 119–129. https://doi.org/10.1023/A:1018770926615
Sinclair, V. G., & Wallston, K. A. (2010). Psychological vulnerability predicts increases in depressive symptoms in individuals with rheumatoid arthritis. Nursing Research, 59(2), 140–146. https://doi.org/10.1097/NNR.0b013e3181d1a6f6
Soto‐Sanz, V., Castellví, P., Piqueras, J. A., Rodríguez‐Marín, J., Rodríguez‐Jiménez, T., Miranda‐Mendizábal, A., & Alonso, J. (2019). Internalizing and externalizing symptoms and suicidal behaviour in young people: A systematic review and meta‐analysis of longitudinal studies. Acta Psychiatrica Scandinavica, 140(1), 5–19. https://doi.org/10.1111/acps.13036
Tacchini, G., Vismara, M. (2019). Generalized anxiety disorder, somatization, and emotional dysregulation: A possible link. In: Altamura, A., Brambilla, P. (Ed.) Clinical cases in psychiatry: Integrating translational neuroscience approaches. Springer. https://doi.org/10.1007/978-3-319-91557-9_12
Terluin, B., van Marwijk, H. W., Adèr, H. J., de Vet, H. C., Penninx, B. W., Hermens, M. L., & Stalman, W. A. (2006). The four-Dimensional Symptom Questionnaire (4DSQ): A validation study of a multidimensional self-report questionnaire to assess distress, depression, anxiety and somatization. Bmc Psychiatry, 6(1), 1–20. https://doi.org/10.1186/1471-244X-6-34
Van Orden, K. A., Witte, T. K., Cukrowicz, K. C., Braithwaite, S. R., Selby, E. A., & JoinerJr, T. E. (2010). The interpersonal theory of suicide. Psychological Review, 117(2), 575. https://doi.org/10.1037/a0018697
Vinsalia, T., & Handajani, Y. S. (2021). Life satisfaction is the most significant determinant of quality of life in the elderly. Universa Medicina, 40(1), 14–21.
Wiblin, J., Holder, N., Holliday, R., & Surís, A. (2021). Predictors of unbearability, unlovability, and unsolvability in veterans with military-sexual-trauma-related posttraumatic stress disorder. Journal of Interpersonal Violence, 36(7–8), 3814–3830. https://doi.org/10.1177/0886260518777554
World Health Organization (2023). Suicide Worldwide in 2019: Global Health Estimates. https://www.who.int/health-topics/suicide#tab=tab_2
Xiao, L., Zhang, S., Li, W., Wu, R., Wang, W., Wang, T., & Lu, C. (2019). The mediating effect of sleep quality on the relationship between emotional and behavioral problems and suicidal ideation. International Journal of Environmental Research and Public Health, 16(24), 4963. https://doi.org/10.3390/ijerph16244963
Yang, C., Zhou, Y., & Xia, M. (2020). How resilience promotes mental health of patients with DSM-5 substance use disorder? The mediation roles of positive affect, self-esteem, and perceived social support. Frontiers in Psychiatry, 11, 588968. https://doi.org/10.3389/fpsyt.2020.588968
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Open access funding provided by the Scientific and Technological Research Council of Türkiye (TÜBİTAK).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent Informed
Consent was obtained from all participants included in the study.
Disclosure of potential conflicts of interest
The authors declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Arslan, G., Türk, N. & Kaya, A. Psychological vulnerability, emotional problems, and quality-of-life: Validation of the brief suicide cognitions scale for Turkish college students. Curr Psychol (2024). https://doi.org/10.1007/s12144-024-05913-w
Accepted:
Published:
DOI: https://doi.org/10.1007/s12144-024-05913-w