
Abstract
Nature-based walking interventions represent a low-cost, eco-friendly activity, designed to assist people in maintaining physical well-being and improving their mental-health status. This systematic review aims to evaluate the evidence regarding the effectiveness of nature-based walking interventions in the improvement of mental health outcomes in adults. This paper draws upon Applied Social Sciences Index & Abstracts (ASSIA), PsycINFO, MEDLINE, EMBASE, the Web of Science Core Collection, Doctoral thesis databases (ProQuest), and manual searches. Due to the heterogeneity of the eligible studies, a narrative synthesis was employed. The present review includes 1,209 adult participants, of whom 336 were female; it also involves 17 discrete studies. The evidence from this systematic review suggests that nature-based walking interventions can indeed improve adults’ moods, sense of optimism, mental well-being, and nature connectedness. They simultaneously mitigate stress, anxiety, and negative rumination. In addition, compared with urban walking, nature-based walking interventions may bring greater benefits vis-à-vis anxiety and rumination. This review contributes to the synthesis of evidence for nature-based walking interventions, and identifies several research gaps around the topic. In clinical practice, nature-based interventions may be used to relieve one’s negative mood, stress, and anxiety. To enhance treatment efficacy, however, they should be combined with formal modes of psychotherapy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Background
A variety of risk factors in relation to urbanisation and urban lifestyles (such as overcrowding, physical inactivity, and a lack of nature connection) have led to negative health outcomes, including the increasing prevalence of mental health disorders (Ventriglio et al., 2021; World Health Organization, 2022). Unhealthy lifestyles have been shown to lead to a variety of psychological and physical health problems. For example, the association of physical inactivity and sedentary lifestyles with obesity is well established (Martínez-González et al., 1999), but the same factors also drive type-2 diabetes, cardiovascular problems, hypertension, heart disease, dementia, and chronic pain (Knight, 2012; Lavie et al., 2019). They are, furthermore, linked to anxiety and depression (Moselhy et al., 2012). Prevention and amelioration of these serious health issues are necessary in order to reduce health-care demands and treatment costs (Health, 2020).
Physical exercise, such as walking in natural settings, has been proposed as a novel and desirable approach to mental-illness prevention and health promotion (Bird, 2007; Frumkin et al., 2017). There is substantial evidence, on the one hand, that cognitive function and mood may be elevated by physical exercise (Kelly et al., 2018a), while the latter may also mitigate depression and anxiety (Carter et al., 2021; Gaia et al., 2021; Kanning & Schlicht, 2010; Lam & Riba, 2016; Xiang et al., 2020). Walking is more accessible and convenient than other forms of physical activity. Easily incorporated into everyday life (Marselle et al., 2014), it confers benefits regarding cardiovascular fitness, physical resilience, psychological-stress reduction, and positive mood (Kelly et al., 2018b; Sianoja et al., 2018; Song et al., 2015; Sturm et al., 2012). On the other hand, the use of outdoor spaces, including natural settings, has been recognised as a determinant of public health (Department of Health, 2014).
The positive influence of “nature contact” on well-being and mental health is supported by a growing evidential corpus, which several reviews have addressed (e.g., Bowler et al., 2010; Capaldi et al., 2015; Gascon et al., 2015; Hartig et al., 2014; Health Council Netherlands, 2004; Ohly et al., 2016; Pritchard et al., 2020; Richardson et al., 2017; van den Berg et al., 2015; World Health Organization, 2016). Indeed, there is substantial evidence for the direct beneficial effects of nature contact on mental health, such as: (1) restorative benefits, including reduction of psychological stress, depression and anxiety, and attention restoration (also reduction in mental fatigue and improvement in cognitive function); and (2) mental well-being improvement (Lovell et al., 2018). The advantages of different forms of nature exposure for psychological welfare are also increasingly confirmed (Beute et al., 2020; Sandifer et al., 2015; Townsend et al., 2018). Moreover, there is evidence (despite mixed outcomes) that physical activities, encouraged by natural settings, play a mediatory role between nature and mental health (Hartig et al., 2014).
It is suggested that there is a synergistic relationship between the benefits of physical exercise and the benefits of nature connection (Shanahan et al., 2016). Evidential quality and research design may vary, but, as noted by Hartig (2014) and numerous others (Bowler et al., 2010; Dzhambov et al., 2019), the mental-welfare advantages associated with nature contact are diverse, and they exploit several pathways. This remains true, although types, frequency, duration and intensity vary.
A range of theories have been proposed to explain why walking in nature might have a positive effect on well-being. Attention Restoration Theory (ART) (Kaplan & Kaplan, 1989) proposes that connections with nature engage people in “effortless” attention towards their environments. “Effortless attention” is also associated with “involuntary attention”, i.e., attention that inherently captures stimuli. This contrasts with “direct” or “voluntary” attention, which is controlled, and which requires greater consumption of mental energy (Berman et al., 2012). Excessive direct attention may lead to mental fatigue and stress (Hartig et al., 1991). Nature walking, conversely, provides respite from voluntary attention, which (subliminally or passively) is replaced by the involuntary form.
Other theories regarding the mental-health benefits of nature connection are the Biophilia Hypothesis (Kellert & Wilson, 1993) and the Stress Reduction Theory (Ulrich et al., 1991). These propose that, since humans have evolved in a natural habitat, their love of nature is innate and instinctive. Furthermore, Stress Reduction Theory originated from an empirical study, which demonstrated that looking at scenery with natural features, such as vegetation or water, generates pleasant emotions, as well as sentiments such as curiosity, enjoyment, and tranquillity. These are restorative, and they promote alertness after stress (Ulrich, 1984).
In addition to these theories, research on place attachment and its relationship with mental health (see, e.g., Ramkissoon et al., 2013; Townsend et al., 2018) has provided valuable insights into how the environment, including natural spaces, can shape individuals’ perceptions and experiences, ultimately impacting their well-being.
In the context of extant theory and the possible psychological advantages of nature exposure, it is clear that walking in natural environments, as opposed to artificial ones, may confer particular benefits. There are, in fact, a growing number of studies to confirm this hypothesis. According to a systematic review of 23 published studies (Thompson, Coon et al., 2011), promising effects for self-reported mental well-being after exercise in nature were not, by contrast, found after the same exercise indoors. Affectively and cognitively, a 50-minute walk in a natural setting may confer superior benefits to a similar walk in a non-natural environment, according to one experimental study (Bratman, Daily et al., 2015). Another experimental study found that group walks in nature may be associated with a variety of mental health benefits, such as lower depression and enhanced mental well-being (Marselle et al., 2014). Similarly, Roe and Aspinall (2011) found restorative benefits in rural walking but not in town-based walking. Still, because of dubious methodological quality, heterogeneous measures of outcome and the sheer variety of settings examined, these findings cannot be seen as conclusive (Barton et al., 2009; Thompson Coon et al., 2011). For instance, a recent systematic review found that nature walks were useful for state anxiety but not for generalised anxiety, and the effects on depression were mixed (Kotera et al., 2021). The same review, however, failed to examine other mental-health outcomes potentially associated with nature walks.
For a better understanding of the extra benefits conferred by nature-based walking, this paper aims systematically to review and evaluate the evidence for the efficacy of green space-based walking interventions on adult mental health. To control features of the natural environment, the study will specifically address green space, while other spaces, such as “blue-space”, may require additional investigation. For the sake of convenience, non-green space and urban space are treated as synonymous within this review.
Review questions
The aim of this systematic review is to evaluate the effectiveness of nature-based walking interventions in improving mental health outcomes amongst adults. The review questions are as follow:
-
a.
Do adults’ mental-health outcomes improve after nature-based walking interventions, compared to the period before the intervention?
-
b.
Is there a greater improvement in people’s mental health following nature-based walking interventions, compared with walks in non-green spaces?
Methods and materials
This systematic review has been registered in the PROSPERO systematic review database (ID: CRD42018091431). The first search for the present review occurred in August 2018. The latest update took place in January 2023. The Cochrane database was screened to ensure there were no similar reviews in this field.
Inclusion and exclusion criteria
In line with the PICOS guidance, which was developed from the Cochrane Handbook for Systematic Reviews of Interventions (Higgins et al., 2019), and the PRISMA statement (Liberati et al., 2009), studies were included if they were based on randomised controlled trials, between-subject experimental or quasi-experimental designs, or within-subject designs with control groups/conditions that compared the effects of nature-based walking interventions on mental health, on the one hand, with those of a suitable control. To be eligible, studies were obliged to contain group comparisons for well-being-related outcomes, and/or pre-post discrepancies. The studies were analysed to identify within-subject and between-subject designs.
The participants included in the studies had to be adults, but there was no restriction on their mental health condition. In other words, they may or may not have presented with active mental illness. Studies comprising participants with a diagnosable physical-health condition were excluded from this review, because the latter mainly focuses on changes for mental health-related outcomes, rather than those of physical ability. Any interventions involving indoor walking and/or virtual experimental settings, with pictures or videos of natural green environments, were excluded. The eligible studies might thus be concerned with a) mental-health improvements in the nature-based walking intervention, and/or b), whether well-being improvements in the nature-based walking intervention are greater than those in the control group. Table 1, below, provides a summary of the criteria for inclusion and exclusion.
Search strategy and selection process
The formal search involved use of a range of bibliographic databases, as follows: Applied Social Sciences Index & Abstracts (ASSIA), PsycINFO, MEDLINE, EMBASE, the Web of Science Core Collection, and Doctoral thesis databases (ProQuest).
The following keywords were used with commands “AND” and “OR”: “natural green space*” OR “green*” OR “natural green area*” OR “natural surrounding*” OR leafy OR grassy OR verdant OR “natural environment*” OR outdoor* OR outside OR country* OR rural OR nature * OR walk* OR ramble* OR stroll* AND “well-being” OR wellbeing OR “well being” OR mental health* OR “sleep quality” OR mindfulness OR anxi* OR depress* OR distress* OR stress* AND “adult” NOT “qualitative” NOT “cross-sectional” NOT “review”. Manual searches were also applied to the reference lists for the screened studies, in order to mitigate possible impediments deriving from selection bias. No additional, qualifying studies were found through manual searches, although one relevant unpublished dissertation was identified (Goulding et al., 2018).
Rayyan was used to manage references. Citations retrieved were downloaded, and duplicates were removed. Independent eligibility screening was applied to abstracts and titles. A second reviewer (Peilin Lin) then independently assessed the articles for eligibility.
Data extraction
The data extraction was independently completed by the author and the second reviewer. In order to support reliability and consistency, a discussion was held before the final version was agreed upon. The following items are pertinent to the review question: study design, participants’ characteristics, the nature of intervention and the control, the number of walking sessions, measurements, pre-post effect size, main findings, and key limitations.
Quality assessment
The Revised Cochrane Risk of Bias Tools for Randomised Trials (ROB-2) were deployed to assess RCT bias risk. This generated categories of high bias risk, “some concerns”, and low risk (Sterne et al., 2019). For the non-randomised studies, observational studies, existing criteria and guidelines were adapted from the SIGN 50 Checklist (Scottish Intercollegiate Guidelines Network, 2019). The applicability of this tool was discussed with co-authors, to ensure the suitability of using it in the present review.
The rating of each quality criterion was classified as follows: well-covered (3 points); adequately addressed (2 points); poorly addressed (1 point); and not addressed (0 points). The rating “well-covered” was assigned when the evaluation categories were clearly reported and could be identified by the reviewers. When detailed descriptions were absent, but the article provided sufficient information for identification, this was deemed “adequately addressed”. “poorly addressed” was assigned when there was no relevant, or only limited, information provided in the article. For the sake of accuracy, nonetheless, the numerical ratings were not deemed final, because the criteria were not of genuinely equal importance. The ratings were finally stated as “++”, “+”, or “-”, in order to represent high quality (overall rating ranging from 18 to 24), medium quality (overall rating ranging from 12 to 17), and relative low quality (overall rating ranging from 0 to 11), respectively. Each of the included studies was assessed independently by the second reviewer and the author. The agreement of quality ratings between these two appraisers reached 75%, and final ratings were decided after discussions.
Results
Included studies
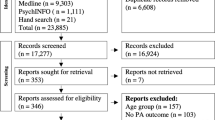
There were 5,710 studies identified during the initial search phase, and one dissertation was requested for inclusion by the authors. Studies were excluded during the initial title and abstract screening. After duplication, 4,222 studies were found, and of these, 118 studies with full texts were screened for further eligibility. Finally, and overall, 17 studies were deemed suitable for inclusion in this systematic review. The selection process for the included studies is shown in a PRISMA flow chart (see Fig. 1). Additional information on exclusions can be found in Appendix A.

Flow chart of study selection
Study characteristics
Key characteristics of the included studies are outlined in Table 2, below. The included studies (n = 17) contained 1,209 participants, among whom 336 participants were female. Most of the studies included the general population, without diagnosed mental illness (n = 15). Only two studies included participants with a major depressive disorder (MDD) (Berman et al., 2012) or those who experienced depression or anxiety (Keenan et al., 2021). The participants ranged in mean age from 19.6 to 40.34 years, and the overall number of male participants in the included studies exceeded that of females. The included studies were mostly conducted in the USA (n = 6), Japan (n = 4), and the U.K (n = 3). More details can be found in Fig. 2.

Regional distribution of the included studies
Intervention characteristics varied among the studies in multiple aspects. Variations occurred, for example, in frequency and duration of walking, and location. The nature-based walking interventions took place in forests (Hassan et al., 2018; Keenan et al., 2021; Koselka et al., 2019; Shin et al., 2011; Song et al., 2018, 2019), urban parks (Aspinall et al., 2015; Berman et al., 2012; Bratman et al., 2015a; Goulding et al., 2018; Johansson et al., 2011; Song et al., 2014, 2015), landfill (Geniole et al., 2016), and other natural landscapes with grassland (Bratman, Daily et al., 2015; de Brito et al., 2019; Mayer et al., 2009b). Conversely, the comparator walking took place downtown (Berman et al., 2012; Johansson et al., 2011; Shin et al., 2011; Song et al., 2019), in urban areas (Bratman, Daily et al., 2015; Bratman, Hamilton, Bratman et al., 2015a, b; Geniole et al., 2016; Hassan et al., 2018; Song et al., 2014, 2015, 2018), in busy shopping streets (Aspinall et al., 2015; Goulding et al., 2018; Koselka et al., 2019), in residential areas with traffic roads (Koselka et al., 2019), and in concrete areas with buildings (Keenan et al., 2021; Mayer et al., 2009a). In terms of length, the walking sessions varied between 90 min and 15 min. Two studies employed multiple walking sessions, namely, 30-minutes sessions for five consecutive days (Keenan et al., 2021), and once-weekly sessions for three weeks (de Brito et al., 2019). All the other studies included here, however, deployed single walking sessions only.
For the measured mental-health outcomes, mood was the most frequently measured outcome. This was generally evaluated either via the Positive Affect and Negative Affect Schedule (PANAS) (Berman et al., 2012; Bratman et al., 2015a; de Brito et al., 2019; Goulding et al., 2018; Keenan et al., 2021; Koselka et al., 2019; Mayer et al., 2009a) and/or the Profile of Mood State (POMS) (Shin et al., 2011; Song et al., 2014, 2015, 2018, 2019). The State-Trait Anxiety Inventory (STAI) was also used to assess anxiety (Bratman, Daily et al., 2015; de Brito et al., 2019; Hassan et al., 2018; Koselka et al., 2019; Song et al., 2014, 2015, 2018, 2019). Rumination and mindfulness levels were measured, respectively, by the Reflection Rumination Questionnaire (RRQ) (Bratman, Daily et al., 2015; Bratman, Hamilton, Bratman et al., 2015a, b; Goulding et al., 2018), and the State Mindfulness Scale (SMS) (Goulding et al., 2018). To measure distress and stress levels, the Bodily Distress Syndrome (BDS) (de Brito et al., 2019; Koselka et al., 2019) checklist and the Perceived Stress Scale (PSS-10) (Koselka et al., 2019) were used.
To evaluate overall mental health and positive emotions, respectively, some authors deployed the Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS) (Goulding et al., 2018; Keenan et al., 2021) and the Eight-item Flourishing Scale (EFI) (Johansson et al., 2011). Only one included study measured the degree of nature connection via the Connectedness to Nature Scale (CNS) (Keenan et al., 2021). Other measurements included EEG (Aspinall et al., 2015; Hassan et al., 2018), and arterial spin labelling (ASL, a neuroimaging method to record brain activity in prefrontal cortex) (Bratman, Hamilton et al., 2015). This facilitated the measurement of meditation, attention, mood, and rumination.
Quality assessment
Amongst the included studies, four were randomised controlled trials (RCT) with two of these being rated as “low risk” of bias (Bratman, Daily et al., 2015; Goulding et al., 2018). For the remaining two, “some concerns” were registered regarding bias (Bratman, Hamilton et al., 2015; Shin et al., 2011). See Fig. 3.

Risk of bias for RCT studies
Ten studies used observational repeated measures, including within-subject design and time-series design with single group participants. Addressing the same groups of participants, these studies compared changing mental-health outcomes over time. Amongst these studies, two were rated as having relatively high quality (“++”) (de Brito et al., 2019; Keenan et al., 2021), whereas four studies were rated as medium quality (“+”) (Berman et al., 2012; Geniole et al., 2016; Koselka et al., 2019; Mayer et al., 2009a) and the rest were rated as low quality (“-”). More details can be found in Table 3.
The included studies evinced only modest quality overall. Nonetheless, due to the limited availability of studies in the research field, the authors elected not to exclude relatively low-quality or medium-quality research. Conversely, the reviewers have taken the quality of each study into account, in order to synthesise the evidence and draw an objective conclusion. Due to a lack of homogeneity in terms of intervention structures and measured outcomes, a meta-analysis was not appropriate. Hence, the data are synthesised narratively.
The effect of nature-walking on mental health
All the details of pre-to-post effect size were reported in Table 2.
Review question one: changes in mental health after nature-based walking intervention
Mood Participants’ mood was measured in twelve studies, by using POMS, PANAS, and the Affect Grid. For those studies that used non-randomised observational studies, four reported significant decrease in negative mood after nature-based green walking, but no changes in positive mood (Song et al., 2014, 2015, 2018, 2019). Two studies reported that positive mood significantly improved after nature-based green walking, but there were no changes in negative mood (de Brito et al., 2019; Mayer et al., 2009b). In the four studies cited above, however, effect sizes were not registered, and the calculation of such size was impossible, given the insufficient information provided. The other two included studies that measured mood outcomes reported that nature-based walking interventions can significantly improve positive, and decrease negative mood, with medium (Koselka et al., 2019) and large effect sizes (Keenan et al., 2021), respectively.
Moreover, a further study that evaluated mood via the Affect Grid (Geniole et al., 2016) detected an increase in participants’ positive mood after green space walking, with medium effect sizes. Nevertheless, the psychometric properties of the Affect Grid have not been clearly reported (Russell et al., 1989), and this reduces the reliability of its results. One study reported significantly different emotional change from two walking locations, having measured emotion via EEG (Aspinall et al., 2015). This study may have yielded relatively invalid results, however, because it only used mobile EEG instruments to measure emotion. The sample size (n = 12) was also particularly small. Johansson and his colleagues (Johansson et al., 2011) used the Eight-item Flourishing Scale (EFI) to measure emotion, and significant changes were found after the nature-based walking intervention. This included decreased negative emotion and increased positive emotion, with medium effect sizes.
Additionally, of three RCT studies that measured mood, two indicated that positive mood improved, and negative mood reduced, after nature-based walking, with small to medium effect sizes (Bratman, Daily et al., 2015; Goulding et al., 2018). One RCT study, conversely, found a large effect size of changes in negative mood decrease and positive mood improvement (in vigorous activity) (Shin et al., 2011).
Amongst those studies, participants in two experienced depression and anxiety, alongside both negative and positive mood changes after nature-based walking. The effect sizes in this case ranged from small to large (Berman et al., 2012; Keenan et al., 2021). Overall, taking the results of quality assessment and participants’ characteristics into account, the included studies show that changes of positive and negative mood after nature-based walking can be effectively detected.
Anxiety Of the included studies, eight examined participants’ levels of anxiety via STAI. Seven of these were non-randomised observational studies, but only one was an RCT study, and this detected lower levels of anxiety (with medium effect size) after greenspace walking. Nevertheless, only one of the included observational studies reported effect size (Koselka et al., 2019). The remainder did not report effect sizes in anxiety variation, or at least, they failed to do so appropriately. For the RCT study (Bratman, Daily et al., 2015), a significant effect of time was found, with small effect size, indicating that participants’ anxiety level decreased after nature-based green-walking interventions.
Rumination and Mindfulness Amongst the included studies, three evaluated rumination using the Rumination and Reflection Questionnaire (RRQ), and all of these employed the RCT experimental design. These studies showed lower rumination after nature-based green walking than before, with small (Bratman, Daily et al., 2015; Bratman, Hamilton, Bratman et al., 2015a, b) to medium effect sizes (Goulding et al., 2018). Mindfulness was also measured by the State Mindfulness Scale (SMS). This evinced a large effect of time, suggesting an improvement in state mindfulness following green space walking (Goulding et al., 2018).
Other mental-health outcomes First, mental well-being was measured in two studies via WEMWBS. One study failed to detect a significant effect of time (Goulding et al., 2018), although the other, in terms of mental well-being change, indicated large effect of time (Keenan et al., 2021). The latter also involved more subjects (n = 60) than the Goulding study (n = 36). Nevertheless, Goulding’s study employed RCT, and only single walking sessions were delivered, with green walking taking place in an urban park. Keenan’s study deployed a non-RCT between-group study, and the authors ran a consecutive five-day walking intervention in a forest park. As both studies were rated as either “low risk” or “high quality”, it is very likely that nature-based green walking could improve one’s mental well-being.
Second, two observational studies addressed the issue of stress levels. Changes in both perceived stress and body stress of the participants were found, with medium effect size (Koselka et al., 2019). One study, however, failed to report effect size (de Brito et al., 2019).
Third, the degree of nature connection was measured by only one non-RCT between-group designed study, and here, a large effect of time was found (Keenan et al., 2021). This implies an affective improvement following nature-based walking interventions.
Lastly, three of the included studies used either EEG or a brain-imaging tool (ASL) to measure changes of rumination, emotion, and meditation (Aspinall et al., 2015; Bratman et al., 2015b; Hassan et al., 2018). These studies reported medium to large effect size of changes, in the reduction of rumination and increased meditation and optimistic emotion.
The synthesised findings, in summary, indicate that optimistic emotion, mental well-being, positive mood and nature connectedness effectively improved after nature-based green walking. Meanwhile, levels of rumination, anxiety and stress were effectively reduced.
Review question two: the effectiveness of nature-based walking interventions on mental health outcomes
Only four RCT studies were included in the present systematic review, which measured participants’ mood, anxiety, rumination, mindfulness, and mental well-being. First, two studies measured mood using PANAS and POMS; these reported an interaction effect in time*group. The same two studies comprised only a single session of walking, while one indicated a statistically significant positive-affect improvement in both walking groups, and no group difference was detected (Goulding et al., 2018). Another RCT study found a significant interaction effect in time*group on mood, indicating that nature-based green walking generated greater levels of positive mood and reduced negative mood, as compared with urban walking (Bratman, Daily et al., 2015). These two studies were rated as “low risk” for bias, and the characteristics of the participants were similar. While the participants in Bratman’s study (Bratman, Hamilton, Bratman et al., 2015a, b) were more numerous (n = 60) than those of Goulding (Goulding et al., 2018; n = 37), these particular findings may have been influenced by discrepancies in sample size and characteristics.
Secondly, only one included RCT study compared differences of anxiety reduction between green and urban walking groups (Bratman, Daily et al., 2015). This study detected a significant interaction effect in time*group in anxiety, indicating that walking in green spaces reduced anxiety compared with walking in urban settings. Effect size, however, was not reported.
Thirdly, three included RCTs compared differences of rumination changes between two walking groups. Of these, two indicated a greater reduction in rumination from green space walking rather than urban walking, since they evinced a significant interaction effect for time*group (Bratman, Daily et al., 2015; Bratman, Hamilton, Bratman et al., 2015a, b). Nonetheless, one RCT study did not find significant group differences in changes in rumination or state mindfulness level between the two walking groups (nature versus urban) (Goulding et al., 2018). As Bratman’s (Bratman, Hamilton, Bratman et al., 2015a, b) study and Goulding’s (Goulding et al., 2018) study employed the same instrument to measure rumination, and their walking settings were similar, the differences in their findings may be a result of sample size and other undetected variables. The study of Goulding et al. (2018) was the only one to conduct a follow-up test for all variables. Nonetheless, no between-group differences were identified for mental well-being, mood, or rumination.
The non-RCT studies reviewed (n = 13) provided consistent evidence that walking in green spaces, such as nature-based environments or forest areas, tends to have a greater positive impact on people’s mental health compared to walking in non-green spaces, such as urban areas or city streets. Following walking in such green environments, reduced negative affect, and improvements in positive affect and mood, were registered by several studies. For instance, Koselka et al. (2019) reported that walking in a forest-path group led to increased positive affect and reduced negative affect, anxiety, and perceived stress. Conversely, fewer positive effects, or even detrimental ones, were generated by walking along an urban roadside. FurthermoreJohansson et al. (2011); Mayer et al. (2009b) noted that nature-based green walking resulted in greater improvements in positive affect and revitalisation, compared to urban walking. Aspinall et al. (2015) found that walking from urban to green spaces reduced arousal, frustration, and engagement, while increasing meditation. Song et al. (2014, 2015, 2018, 2019), meanwhile, conducted multiple studies and consistently found that walking in green spaces not only reduced anxiety, but also improved mood state and decreased negative feelings, as compared to walking in urban areas. After forest-based walking, the same authors noted correlations between variations in particular mood scales (e.g., depression-dejection) and levels of trait-anxiety.
Notwithstanding the heterogeneity of natural settings and research design in the studies, the presence of natural elements and the peaceful environment in greenspaces do seem to contribute to various mental health benefits. Overall, the non-RCT studies under review suggest that a greenspace-based walking intervention is more beneficial for mental health than walking in non-green spaces.
Generally, the evidence suggests that nature-based walking interventions may effectively reduce participants’ anxiety, negative affect, perceived stress, and rumination. They may also enhance meditation and increase positive affect. A significant group difference in the measurement of mental well-being was not found. Nonetheless, in comparison with non-nature walking, there are additional overall advantages in health-related outcomes for nature-walking groups / conditions, as opposed to non-natural environments.
Discussion
The present systematic review aims to investigate the effectiveness of nature-based walking interventions on mental health outcomes in adults. The evidence from 17 studies, 16 of them published in academic journals, has been synthesised, and gaps in the research evidence are discussed below.
Regarding the two review questions, this evidence suggests that adult participants’ positive mood, optimistic emotion, mental well-being, and nature connection effectively improved following nature-based, green-walking interventions. Moreover, in comparison with urban walking, there was a significant decrease in rumination, anxiety and stress. No significant between-group differences were found in mood and measurements of well-being, in terms of the RCT studies. The non-RCT studies in this review indicated that nature walking provided additional benefits in enhanced positive affect and mindfulness level. Overall, then, and to reiterate, nature-based walking interventions would appear to generate significant dividends in mental health, as compared with non-green environments.
These findings are consistent with a recent systematic review, which indicated that various physical activities in nature (i.e., hiking, jogging, walking, etc.) enabled people to reduce their anxiety and negative affect, while improving positive affect (Wicks et al., 2022). The current systematic review also found effects of green walking on mental well-being, mindfulness, stress, nature connectedness, and rumination.
The findings of mood enhancement and restorative benefits, such as fatigue reduction after greenspace walking interventions, may support the Attention Restoration Theory (ART), to the effect that the natural environment can restore human attention (from directed attention) and reduce fatigue (Kaplan, 1995). Nonetheless, one study indicated that, from pre-walk to post-walk, there was no improvement in directed attention for either condition (de Brito et al., 2019b). Moreover, another study reported that nature exposure was not associated with improved attentional control (Geniole et al., 2016). Therefore, although there may be some synergistic benefits of walking and nature exposure for mood improvements, the mechanism proposed by ART may need further investigation.
It is, furthermore, possible to situate the findings of the present study in a wider context, notably in terms of mental health improvements in a post-COVID world. For instance, Ramkissoon (2021) proposed a conceptual framework of integrative body-mind interventions for well-being improvement, using the COVID-19 place confinement as the context. In a similar vein, Ramkissoon (2022) developed and proposed “a single integrative model of adaptive social bonding interventions (psycho-social, nature, and digital), wellbeing and quality of life.” This emphasised the role of nature-based therapies as a means of enhancing mental health. The framework and model proposed by Ramkissoon provides valuable perspectives on the multidimensional aspects of well-being, and the potential benefits of interventions that integrate mind-body approaches. This expansion allows us to appreciate how nature-based walking can contribute to various dimensions of well-being beyond mental health, such as physical and spiritual well-being.
The present study has reaffirmed the efficacy of nature-located green walking in the context of various mental health outcomes. Nonetheless, there was either a lack of external validity in, or an inconsistency between, the studies included in this review. Although all the deployed measurements related to mental health, the experimental designs that the studies employed were heterogeneous, so that no definite conclusions could be reached. More specifically, the reviewed studies conducted experiments to examine whether green walking brings greater psychological benefits than non-green walking, due to the effects of connectedness with nature. Conversely, the degree of nature connectedness for participants, in the two situations, was only evaluated by one study (Keenan et al., 2021). Therefore, it is not possible to assess the extent to which environmental differences (green versus non-green) contributed to the different psychological outcomes of walking. Further studies are required to explore whether the degree of connectedness with nature predicts differences in psychological outcomes, vis-à-vis walking in nature versus walking in urban environments.
In some of the included studies, sample sizes were extremely small. Four studies mentioned this weakness as a limitation that may lead to inconclusive results. Secondly, in the Song et al. studies (Song et al., 2014, 2015), only male participants were involved, which reduced the sample’s representativeness vis-à-vis a realistic population (Song et al., 2014, 2015). Third, result validity may be reduced by the assessment techniques deployed by some of the studies. For example, the Aspinall study (Aspinall et al., 2015) used a low-cost headwear EEG recorder that occasionally failed to stream data, causing some data to be missed. It is also possible that this headwear negatively influenced mood while walking. Goulding (Goulding et al., 2018), meanwhile, noted that some vocabulary in PANAS may be outdated, and this may have caused some confusion amongst participants. The Johansson study (Johansson et al., 2011) noted the low internal consistency of certain measurements employed. Lastly, Geniole (Geniole et al., 2016) and Shin (Shin et al., 2011) observed that different types of environment may generate different results, and that we should consider the pro-environmental behaviour of participants before their walking interventions. Improvements in mental well-being, for instance, may be related to previous, environmentally friendly lifestyles.
Each study employed controlled trials to test the differences between walking in greenspaces and non-greenspaces. Nonetheless, synthesis of the results via meta-analysis remains challenging, due to discrepancies in research design (e.g., the review included both between-subject and within-subject studies). The authors decided not to run a meta-analysis to display the overall effect size of green walking amongst adults, for several reasons. First, the two Bratman RCT studies did not provide SD and mean values, which are prerequisites for such an analysis. Second, the included studies used various measurements that could not be combined. Even though the fix-effect model may address some of these issues, there were still a few studies that poorly presented the descriptive data, while evincing some missing values.
Well-being may also be affected by other vectors, such as weather or the duration of walking. The included studies in this review were conducted in very different countries, with distinctive weather patterns and natural features. Accordingly, weather conditions should be considered and controlled as an important variable, in order properly to interpret the results of these studies.
In order to assess the mental-health efficacy of nature-based, green walking more precisely, additional randomised/controlled trials will be needed. These should be done with a randomisation process, pre/post and follow-up test, as well as valid measurements implemented to control for external variables and experimental biases. Most importantly, it is necessary to explore the mediators between green walking and the improvement of mood, and other measures of mental well-being.
RCTs for nature-based walking may reveal what types of green space are most beneficial for mental well-being. The studies included in this review varied in many ways, making the mechanisms through which nature walking influences mood difficult to discern. For most of the included studies, total intervention durations varied, and there were frequent disparities in the type of green space utilised. Although it is believed that natural environments are beneficial, one study argued that natural green spaces are not always restorative: densely wooded areas, and the natural environment, may even trigger stress and fear (Gatersleben & Andrews, 2013). In fact, in most of the included studies, there was little discussion of the natural environments in question, and the latter were often poorly described.
While the overall conclusion may align with existing literature in this field, our review specifically focuses on the effects of nature-based walking on mental health outcomes, consolidating the evidence from a range of studies. By systematically synthesising the available evidence, we provide a comprehensive overview of the specific mental health benefits associated with this intervention. Meanwhile, the current review acknowledges that our second research question yielded a null result. Null findings, while they present interpretative challenges, can still contribute to the corpus of knowledge by indicating fields where further research is required. By reporting these null results, we aim to encourage future research to explore potential factors that may influence the overall well-being outcomes of nature-based walking.
The contribution of this systematic review extends beyond the immediate findings. The systematic review approach we have employed allows researchers, practitioners and policymakers to access a consolidated and critically appraised body of literature on this topic. This can serve as a valuable resource for evidence-based decision-making, and the development of interventions to promote mental health.
Conclusions
Nature-based walking is an environmentally responsible and relatively inexpensive intervention. This review demonstrates that it helps people maintain and improve their mood and mindfulness, and it also reduces anxiety and rumination. While further research is certainly needed, the present results confirm the desirability of supporting mental health by providing accessible green spaces (e.g., additional urban parks). Nonetheless, nature-based walking should not only be viewed as an “intervention” in terms of public health. Rather, people in general should be encouraged to incorporate green walking into their normal lifestyles. Meanwhile, there is a need for additional research on the use of nature-based interventions within formal psychotherapies, to enhance creativity and increase therapeutic benefits.
Data Availability
A data-availability statement is not available, as the present study is a systematic review.
Reference list
Aspinall, P., Mavros, P., Coyne, R., & Roe, J. (2015). The urban brain: Analysing outdoor physical activity with mobile EEG [Article]. British Journal of Sports Medicine, 49(4), 272–276. https://doi.org/10.1136/bjsports-2012-091877
Barton, J., Hine, R., & Pretty, J. (2009). The health benefits of walking in greenspaces of high natural and heritage value [Article]. Journal of Integrative Environmental Sciences, 6(4), 261–278. https://doi.org/10.1080/19438150903378425
Berman, M. G., Kross, E., Krpan, K. M., Askren, M. K., Burson, A., Deldin, P. J., Kaplan, S., Sherdell, L., Gotlib, I. H., & Jonides, J. (2012). Interacting with nature improves cognition and affect for individuals with depression [Article]. Journal of Affective Disorders, 140(3), 300–305. https://doi.org/10.1016/j.jad.2012.03.012
Beute, F., Andreucci, M. B., Lammel, A., Davies, Z. G., Glanville, J., Keune, H., Marselle, M., O’Brien, L. A., Olszewska-Guizzo, A., Remmen, R., Russo, A., & de Vries, S. (2020). Types and characteristics of urban and peri-urban green spaces having an impact on human mental health and wellbeing: A systematic review [Technical report]. EKLIPSE Expert Working Group. UK Centre for Ecology & Hydrology, Wallingford, UK. https://kar.kent.ac.uk/89644/
Bird, W. (2007). Natural thinking: Investigating the links between the natural environment, biodiversity and mental health. Royal Society for the Protection of Birds, 1, 3–116.
Bowler, D. E., Buyung-Ali, L. M., Knight, T. M., & Pullin, A. S. (2010). A systematic review of evidence for the added benefits to health of exposure to natural environments. Bmc Public Health, 10(1), 456. https://doi.org/10.1186/1471-2458-10-456
Bratman, G. N., Daily, G. C., Levy, B. J., & Gross, J. J. (2015a). The benefits of nature experience: Improved affect and cognition [Article]. Landscape and Urban Planning, 138, 41–50. https://doi.org/10.1016/j.landurbplan.2015a.02.005
Bratman, G. N., Hamilton, J. P., Hahn, K. S., Daily, G. C., & Gross, J. J. (2015b). Nature experience reduces rumination and subgenual prefrontal cortex activation [Article]. Proceedings of the National Academy of Sciences - PNAS, 112(28), 8567–8572. https://doi.org/10.1073/pnas.1510459112
Capaldi, C. A., Passmore, H. A., Nisbet, E., Zelenski, J., & Dopko, R. (2015). Flourishing in nature: A review of the benefits of connecting with nature and its application as a wellbeing intervention. International Journal of Wellbeing, 5(4), 1–16. https://doi.org/10.5502/ijw.v5i4.449
Carter, T., Pascoe, M., Bastounis, A., Morres, I. D., Callaghan, P., & Parker, A. G. (2021). The effect of physical activity on anxiety in children and young people: A systematic review and meta-analysis. Journal of Affective Disorders, Vol. 285, https://doi.org/10.1016/j.jad.2021.02.026
de Brito, J. N., Pope, Z. C., Mitchell, N. R., Schneider, I. E., Larson, J. M., Horton, T. H., & Pereira, M. A. (2019). Changes in psychological and cognitive outcomes after green versus suburban walking: A pilot crossover study. International Journal of Environmental Research and Public Health, 16(16), https://doi.org/10.3390/ijerph16162894
Department of Health (2014). Improving outcomes and supporting transparency (Part 2): Summary technical specifications of public health indicators. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/382115/PHOF_Part_2_Technical_Specifications_Autumn_2014_refresh_02.12.2014_FINAL.pdf
Dzhambov, A. M., Hartig, T., Tilov, B., Atanasova, V., Makakova, D. R., & Dimitrova, D. D. (2019). Residential greenspace is associated with mental health via intertwined capacity-building and capacity-restoring pathways. Environmental Research, 178, 108708. https://doi.org/10.1016/j.envres.2019.108708
Frumkin, H., Bratman, G. N., Breslow, S. J., Cochran, B., Kahn, P. H., Lawler, J. J., Levin, P. S., Tandon, P. S., Varanasi, U., Wolf, K. L., & Wood, S. A. (2017). Nature contact and human health: A research agenda. In Environmental Health Perspectives (Vol. 125, Issue 7). https://doi.org/10.1289/EHP1663
Gaia, J. W. P., Ferreira, R. W., & Pires, D. A. (2021). Effects of physical activity on the mood states of young students. Journal of Physical Education (Maringa), 32(1), https://doi.org/10.4025/jphyseduc.v32i1.3233
Gascon, M., Triguero-Mas, M., Martínez, D., Dadvand, P., Forns, J., Plasència, A., & Nieuwenhuijsen, M. (2015). Mental Health benefits of long-term exposure to Residential Green and Blue Spaces: A systematic review. International Journal of Environmental Research and Public Health, 12(4), 4354–4379. https://doi.org/10.3390/ijerph120404354
Gatersleben, B., & Andrews, M. (2013). When walking in nature is not restorative-The role of prospect and refuge. Health and Place, 20. https://doi.org/10.1016/j.healthplace.2013.01.001
Geniole, S. N., David, J. P. F., Euzebio, R. F. R., Toledo, B. Z. S., Neves, A. I. M., & McCormick, C. M. (2016). Restoring land and mind: The benefits of an Outdoor Walk on Mood are enhanced in a naturalized landfill area relative to its neighboring Urban Area. Ecopsychology, 8(2), https://doi.org/10.1089/eco.2016.0005
Goulding, A., Morris, Graham, P., Robbins, K., Wang, L., & Espada, L. (2018). The Effect of walking in Nature on Mindfulness, Rumination and Well-being. The University of Edinburgh.
Hartig, T., Mang, M., & Evans, G. W. (1991). Restorative Effects of Natural Environment Experiences [Article]. Environment and Behavior, 23(1), 3–26. https://doi.org/10.1177/0013916591231001
Hartig, T., Mitchell, R., de Vries, S., & Frumkin, H. (2014). Nature and Health. Annual Review of Public Health, 35(1), 207–228. https://doi.org/10.1146/annurev-publhealth-032013-182443
Hassan, A., Tao, J., Li, G., Jiang, M., Aii, L., Zhihui, J., Zongfang, L., & Qibing, C. (2018). Effects of Walking in Bamboo Forest and City Environments on Brainwave Activity in Young Adults. Evidence-Based Complementary and Alternative Medicine, 2018, 9653857–9653859. https://doi.org/10.1155/2018/9653857
Health, T. L. G. (2020). Mental health matters. The Lancet Global Health, 8(11), e1352–e1352. https://doi.org/10.1016/S2214-109X(20)30432-0
Health Council Netherlands (2004). Nature and health: The influence of nature on social, psychological and physical well-being.
Higgins, J. P. T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M. J., & Welch, V. A. (2019). Cochrane handbook for systematic reviews of interventions. In Cochrane Handbook for Systematic Reviews of Interventions. https://doi.org/10.1002/9781119536604
Johansson, M., Hartig, T., & Staats, H. (2011). Psychological benefits of walking: Moderation by Company and Outdoor Environment [Article]. Applied Psychology: Health and Well-Being, 3(3), 261–280. https://doi.org/10.1111/j.1758-0854.2011.01051.x
Kanning, M., & Schlicht, W. (2010). Be active and become happy: An ecological momentary assessment of physical activity and mood. Journal of Sport and Exercise Psychology, 32(2), https://doi.org/10.1123/jsep.32.2.253
Kaplan, S. (1995). The restorative benefits of nature: Toward an integrative framework. Journal of Environmental Psychology, 15(3), https://doi.org/10.1016/0272-4944(95)90001-2
Kaplan, R., & Kaplan, S. (1989). In Kaplan (Ed.), The experience of nature: A psychological perspective. Cambridge University Press.
Keenan, R., Lumber, R., Richardson, M., & Sheffield, D. (2021). Three good things in nature: A nature-based positive psychological intervention to improve mood and well-being for depression and anxiety. Journal of Public Mental Health, 20(4), https://doi.org/10.1108/JPMH-02-2021-0029
Kellert, S. R., & Wilson, E. O. (1993). In R. Kellert, & E. O. Wilson (Eds.), The Biophilia hypothesis. Island Press.
Kelly, P., Williamson, C., Niven, A. G., Hunter, R., Mutrie, N., & Richards, J. (2018a). Walking on sunshine: Scoping review of the evidence for walking and mental health. British Journal of Sports Medicine (Vol, 52(12), https://doi.org/10.1136/bjsports-2017-098827
Kelly, P., Williamson, C., Niven, A. G., Hunter, R., Mutrie, N., & Richards, J. (2018b). Walking on sunshine: Scoping review of the evidence for walking and mental health. British Journal of Sports Medicine, 52(12), https://doi.org/10.1136/bjsports-2017-098827
Knight, J. A. (2012). Physical inactivity: Associated Diseases and Disorders [Article]. Annals of Clinical and Laboratory Science, 42(3), 320–337.
Koselka, E. P. D., Weidner, L. C., Minasov, A., Berman, M. G., Leonard, W. R., Santoso, M. V., de Brito, J. N., Pope, Z. C., Pereira, M. A., & Horton, T. H. (2019). Walking green: Developing an evidence base for nature prescriptions. International Journal of Environmental Research and Public Health, 16(22), https://doi.org/10.3390/ijerph16224338
Kotera, Y., Lyons, M., Vione, K. C., & Norton, B. (2021). Effect of nature walks on depression and anxiety: A systematic review. In Sustainability (Switzerland) (Vol. 13, Issue 7). https://doi.org/10.3390/su13074015
Lam, C. W. L., & Riba, M. (2016). Physical Exercise Interventions for Mental Health. In L. C. W. Lam, & M. Riba (Eds.), Physical Exercise Interventions for Mental Health. Cambridge University Press. https://doi.org/10.1017/CBO9781316157565
Lavie, C. J., Ozemek, C., Carbone, S., Katzmarzyk, P. T., & Blair, S. N. (2019). Sedentary Behavior, Exercise, and Cardiovascular Health. In Circulation Research (Vol. 124, Issue 5). https://doi.org/10.1161/CIRCRESAHA.118.312669
Liberati, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gøtzsche, P. C., Ioannidis, J. P. A., Clarke, M., Devereaux, P. J., Kleijnen, J., & Moher, D. (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. In PLoS Medicine (Vol. 6, Issue 7). https://doi.org/10.1371/journal.pmed.1000100
Lovell, R., Depledge, M., & Maxwell, S. (2018). Health and the natural environment: A review of evidence, policy, practice and opportunities for the future.
Marselle, M. R., Irvine, K. N., & Warber, S. L. (2014). Examining group walks in nature and multiple aspects of well-being: A large-scale study. Ecopsychology, 6(3), https://doi.org/10.1089/eco.2014.0027
Martínez-González, M., Martínez, J. A., Hu, F. B., Gibney, M. J., & Kearney, J. (1999). Physical inactivity, sedentary lifestyle and obesity in the European Union. International Journal of Obesity, 23(11), https://doi.org/10.1038/sj.ijo.0801049
Mayer, F. S., Frantz, C. M., Bruehlman-Senecal, E., & Dolliver, K. (2009a). Why Is Nature Beneficial? Environment and Behavior, 41(5), 607–643. https://doi.org/10.1177/0013916508319745
Mayer, F. S., Frantz, C. M. P., Bruehlman-Senecal, E., & Dolliver, K. (2009b). Why is nature beneficial?: The role of connectedness to nature. Environment and Behavior, 41(5), https://doi.org/10.1177/0013916508319745
Moselhy, H. F., Ghubach, R., El-Rufaie, O., Zoubeidi, T., Badrinath, P., Sabri, S., & Yousef, S. (2012). The association of depression and anxiety with unhealthy lifestyle among United Arab Emirates adults. In Epidemiology and Psychiatric Sciences (Vol. 21, Issue 2). https://doi.org/10.1017/S2045796011000709
Ohly, H., White, M. P., Wheeler, B. W., Bethel, A., Ukoumunne, O. C., Nikolaou, V., & Garside, R. (2016). Attention restoration theory: A systematic review of the attention restoration potential of exposure to natural environments. Journal of Toxicology and Environmental Health Part B Critical Reviews, 19(7), 305–343. https://doi.org/10.1080/10937404.2016.1196155
Pritchard, A., Richardson, M., Sheffield, D., & McEwan, K. (2020). The relationship between Nature Connectedness and Eudaimonic Well-Being: A Meta-analysis. Journal of Happiness Studies, 21(3), 1145–1167. https://doi.org/10.1007/s10902-019-00118-6
Ramkissoon, H. (2021). Body-mind Medicine Interventions in COVID-19 Place Confinement for Mental, Physical and spiritual wellbeing. OBM Integrative and Complementary Medicine, 6(2), 1–1. https://doi.org/10.21926/obm.icm.2102016
Ramkissoon, H. (2022). COVID-19 adaptive interventions: Implications for Wellbeing and Quality-of-life. Frontiers in Psychology, 13, 810951. https://doi.org/10.3389/fpsyg.2022.810951
Ramkissoon, H., Smith, G., L. D., & Weiler, B. (2013). Testing the dimensionality of place attachment and its relationships with place satisfaction and pro-environmental behaviours: A structural equation modelling approach. Tourism Management, 36, 552–566. https://doi.org/10.1016/j.tourman.2012.09.003
Richardson, M., Maspero, M., Golightly, D., Sheffield, D., Staples, V., & Lumber, R. (2017). Nature: A new paradigm for well-being and ergonomics. Ergonomics, 60(2), 292–305. https://doi.org/10.1080/00140139.2016.1157213
Roe, J., & Aspinall, P. (2011). The restorative benefits of walking in urban and rural settings in adults with good and poor mental health. Health & Place, 17(1), 103–113. https://doi.org/10.1016/j.healthplace.2010.09.003
Russell, J. A., Weiss, A., & Mendelsohn, G. A. (1989). Affect Grid: A single-item scale of pleasure and arousal. Journal of Personality and Social Psychology, 57, 493–502.
Sandifer, P. A., Sutton-Grier, A. E., & Ward, B. P. (2015). Exploring connections among nature, biodiversity, ecosystem services, and human health and well-being: Opportunities to enhance health and biodiversity conservation. Ecosystem Services, 12, 1–15. https://doi.org/10.1016/j.ecoser.2014.12.007
Scottish Intercollegiate Guidelines Network (2019). A guideline developer´s handbook. Edinburgh: SIGN, 50(November 2019).
Shanahan, D. F., Franco, L., Lin, B. B., Gaston, K. J., & Fuller, R. A. (2016). The benefits of natural environments for physical activity. Sports Medicine, 46(7), 989–995. https://doi.org/10.1007/s40279-016-0502-4
Shin, W. S., Shin, C. S., Yeoun, P. S., & Kim, J. J. (2011). The influence of interaction with forest on cognitive function. Scandinavian Journal of Forest Research, 26(6), 595–598. https://doi.org/10.1080/02827581.2011.585996
Sianoja, M., Syrek, C. J., de Bloom, J., Korpela, K., & Kinnunen, U. (2018). Enhancing daily well-being at work through lunchtime park walks and relaxation exercises: Recovery experiences as mediators. Journal of Occupational Health Psychology, 23(3), https://doi.org/10.1037/ocp0000083
Song, C., Ikei, H., Igarashi, M., Miwa, M., Takagaki, M., & Miyazaki, Y. (2014). Physiological and psychological responses of young males during spring-time walks in urban parks [Article]. Journal of Physiological Anthropology, 33(1), 8–8. https://doi.org/10.1186/1880-6805-33-8
Song, C., Ikei, H., Igarashi, M., Takagaki, M., & Miyazaki, Y. (2015). Physiological and psychological effects of a walk in Urban parks in fall. International Journal of Environmental Research and Public Health, 12(11), https://doi.org/10.3390/ijerph121114216
Song, C., Ikei, H., Park, B. J., Lee, J., Kagawa, T., & Miyazaki, Y. (2018). Psychological benefits of walking through forest areas. International Journal of Environmental Research and Public Health, 15(12), https://doi.org/10.3390/ijerph15122804
Song, C., Ikei, H., Kagawa, T., & Miyazaki, Y. (2019). Effects of walking in a forest on young women. International Journal of Environmental Research and Public Health, 16(2), https://doi.org/10.3390/ijerph16020229
Sterne, J. A. C., Savović, J., Page, M. J., Elbers, R. G., Blencowe, N. S., Boutron, I., Cates, C. J., Cheng, H. Y., Corbett, M. S., Eldridge, S. M., Emberson, J. R., Hernán, M. A., Hopewell, S., Hróbjartsson, A., Junqueira, D. R., Jüni, P., Kirkham, J. J., Lasserson, T., Li, T., & Higgins, J. P. T. (2019). RoB 2: A revised tool for assessing risk of bias in randomised trials. The BMJ, 366. https://doi.org/10.1136/bmj.l4898
Sturm, J., Plöderl, M., Fartacek, C., Kralovec, K., Neunhäuserer, D., Niederseer, D., Hitzl, W., Niebauer, J., Schiepek, G., & Fartacek, R. (2012). Physical exercise through mountain hiking in high-risk suicide patients. A randomized crossover trial. Acta Psychiatrica Scandinavica, 126(6), https://doi.org/10.1111/j.1600-0447.2012.01860.x
Thompson Coon, J., Boddy, K., Stein, K., Whear, R., Barton, J., & Depledge, M. (2011). Does participating in physical activity in outdoor natural environments have a greater effect on physical and mental wellbeing than physical activity indoors? A systematic review. Journal of Epidemiology and Community Health (1979), 65(Suppl 2), A38–A38. https://doi.org/10.1136/jech.2011.143586.85
Townsend, M., Henderson-Wilson, C., Ramkissoon, H., & Weerasuriya, R. (2018). Therapeutic landscapes, restorative environments, place attachment, and well-being (pp. 57–62). https://doi.org/10.1093/med/9780198725916.003.0036
Ulrich, R. S. (1984). View through a window may influence recovery from surgery. Science (American Association for the Advancement of Science), 224(4647), 420–421. https://doi.org/10.1126/science.6143402
Ulrich, R. S., Simons, R. F., Losito, B. D., Fiorito, E., Miles, M. A., & Zelson, M. (1991). Stress recovery during exposure to natural and urban environments. Journal of Environmental Psychology, 11(3), 201–230. https://doi.org/10.1016/S0272-4944(05)80184-7
van den Berg, M., Wendel-Vos, W., van Poppel, M., Kemper, H., van Mechelen, W., & Maas, J. (2015). Health benefits of green spaces in the living environment: A systematic review of epidemiological studies. Urban Forestry & Urban Greening, 14(4), 806–816. https://doi.org/10.1016/j.ufug.2015.07.008
Ventriglio, A., Torales, J., Castaldelli-Maia, J. M., De Berardis, D., & Bhugra, D. (2021). Urbanization and emerging mental health issues. CNS Spectrums, 26(1), https://doi.org/10.1017/S1092852920001236
Wicks, C., Barton, J., Orbell, S., & Andrews, L. (2022). Psychological benefits of outdoor physical activity in natural versus urban environments: A systematic review and meta-analysis of experimental studies. In Applied Psychology: Health and Well-Being. https://doi.org/10.1111/aphw.12353
World Health Organization (2016). Urban green spaces and health.
World Health Organization (2022). World mental health report: Transforming mental health for all.
Xiang, M. Q., Tan, X. M., Sun, J., Yang, H. Y., Zhao, X. P., Liu, L., Hou, X. H., & Hu, M. (2020). Relationship of Physical Activity With Anxiety and Depression Symptoms in Chinese College Students During the COVID-19 Outbreak. Frontiers in Psychology, 11. https://doi.org/10.3389/fpsyg.2020.582436
Funding
This study did not receive any fundings.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
There is no conflict of interest to disclose for this manuscript.
Informed consent
This manuscript has not involved human participants, so consent forms are inapplicable for this study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ma, J., Lin, P. & Williams, J. Effectiveness of nature-based walking interventions in improving mental health in adults: a systematic review. Curr Psychol 43, 9521–9539 (2024). https://doi.org/10.1007/s12144-023-05112-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-023-05112-z