
Abstract
Positive psychology (PP) interventions are treatment methods or intentional activities aiming to develop positive feelings, behaviors or cognitions. This study was conducted to determine the effect on mental well-being, life attitude and depression levels of PP program applied to patients diagnosed with depression. The pre, post and follow-up test were conducted as a quasi-experimental study. Patients who diagnosis of depression for at least 6 months constituted the population of the study, and a total of 53 patients, 26 were in the experimental and 27 in the control group. Data were collected using Personal Information Form,Beck Depression Inventory,Warwick-Edinburgh Mental Well-Being Scale and Life Attitude Profile Scale. After the analysis,it has been determined that the online PP program is effective in reducing the level of depression, increasing mental well-being and developing a positive life attitude. It is recommended that the PP program be used by psychiatric nurses in the treatment of depression and the execution of studies comparing online positive psychology practices with face-to-face positive psychology practices are recommended.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Major depressive disorder (MDD) is the most common psychiatric disorder that significantly reduces the quality of life (Burns, 2015). It is thought that approximately 280 million people in the world may be depressed (WHO-Depression, 2021). MDD is a mental condition that starts at an early age and impairs the functionality of the individual (Lam, 2018). By 2030, MDD is thought to be the leading cause of the disease burden globally (Mental Health Action Plan, 2013-2020). On the other hand, depression can cause thoughts of death and suicide (Kleinman, 2013; Keck, 2010). Additionally, failure to treat depression is costly. For such reasons, one of the main problems that WHO focuses on in terms of mental health is taking precautions regarding depression and suicide (WHO-Depression, 2021).
Positive psychology was developed by Seligman et al. (2006) (Seligman et al., 2006). There are three main points that positive psychology focuses on. These are satisfaction (enjoyment with positive emotions), participation (using your strengths effectively), and meaning (being part of something bigger than yourself) (Leimon, 2009). Seligman (2011) further expanded these three dimensions and proposed a fivefold structure for mental health and happiness. These five structures are; positive emotions, engagement, relationships, meaning, and accomplishment. He named this quintuple structure the PERMA model (Seligman, 2011).
Symptoms such as lack of pleasure, decreased appetite and weight loss, sleep problems, psychomotor agitation or retardation, decreased energy, fatigue, feeling of worthlessness, low self-esteem, thoughts of guilt, difficulty in concentration, and suicidal thoughts may occur in depression (Gilbert, 2009). As can be seen, there is a decrease in positive emotions and an increase in negative emotions in depression.
Positive psychology interventions (PPIs), developed by Seligman et al. (2006), are based on the theory that depression can be effectively treated not only by focusing on negative symptoms, but also by experiencing more positive emotions, revealing and enhancing individuals’ strengths, and adding meaning to their lives. (Seligman et al., 2006). According to Sin and Lyubomirsky (2009), PPIs are “therapeutic methods or intentional activities aimed at improving positive emotions, positive behaviors, or positive cognitions” (Sin & Lyubomirsky, 2009). Increasing these positive resources in depression makes it possible to effectively cope with negative symptoms and to take precautions against future recurrences (Seligman et al. 2006). Symptoms of depression often include a lack of positive emotion, a lack of participation, and a lack of meaning in life, but these are often seen as consequences of depression. Seligman et al. (2006) suggest that these may be the cause of depression, and therefore, developing positive emotion, participation, and meaning may alleviate depression (Seligman et al., 2006).
The most important feature of PPIs is to reveal positive emotions, thoughts, and behaviors among people. In this direction, some exercises (gratitude, enjoyment, etc.) have been developed to reveal these thoughts, feelings, and behaviors (Eryılmaz, 2017). The idea behind PPIs is to increase well-being and build up the individual’s positive resources, often automatically weakening or eliminating many factors that can cause depression to persist, such as pessimism or low self-esteem (Akhtar, 2012).
Rapid changes and developments in information and communication technologies have led to serious changes in the needs of individuals in the fields of health, as in many other fields. This change has been effective in the creation of new service areas such as telehealth and telenursing, which are methods supported by technology (Işık & Güler, 2010; Pazar et al., 2015; Ogueji et al., 2022). It is thought that it would be advantageous to reduce depressive symptoms by interviewing patients at home or at any place or time convenient for them through online channels. Thus, it is thought that society can access practices of positive psychology in an economical, fast, effective, and widespread way and a positive contribution can be made directly to coping with depression. It is extremely critical to provide effective treatment because depression is prevalent (4.6% in Turkey, according to 2019 Global Health Data) (Turkey, GHD, 2022), reduces quality of life and causes suicide. In this respect, it is important to examine whether or how the positive psychology program can be used as an evidence-based practice in the treatment of depression. In addition, positive psychology approaches have been shown to play a vital role in maintaining mental health in challenging times, and there are studies that suggest it is important to include when examining the psychological consequences of COVID-19 (Waters et al., 2021). In case of re-experiencing such pandemic processes, online meetings may be preferred. It is considered important to evaluate the effectiveness of these meetings. Although there are studies in the world showing that positive psychology interventions decrease depression and increase well-being (Sin & Lyubomirsky, 2009; Hanson, 2019), no experimental study has been found in this context in Turkey as far as has been reached. The study is the first in this regard at the national and international level in terms of applying online positive psychology interventions to depression patients. The aim of the study is to determine the effect of the positive psychology program applied to depression patients on mental well-being, life attitudes, and depression levels.
Materials and methods
The research is quasi-experimental research with a pre-test, post-test, follow-up-test, and control group.
Participants
The population of the study consisted of patients who were treated with a diagnosis of MDD according to DSM-5 in the psychiatry outpatient clinic of a research and practice hospital at the time of the study. This study was conducted during the COVID-19 pandemic. The criteria for inclusion in the study were having no obstacle in communication, being over the age of 18, being literate, being followed up with a diagnosis of MDD according to the DSM-5 criteria, having been receiving treatment for depression for at least 6 months, and having participated in no positive psychology program for the disease in the last 5 years. Exclusion criteria were being diagnosed with another comorbid mental disorder, having mental retardation or dementia, which makes it impossible to cooperate, having psychotic symptoms in addition to depression, being illiterate, and receiving inpatient treatment. In the present study, a prior power analysis was performed by using the G Power program in calculating the sample size. Previous studies were reviewed (Button et al. 2015) and the expected confidence intervals of the “Beck Depression Inventory” were determined, while the confidence interval was α = 0.05, the power of the test (1-β) was 0.95, and the effect size was d = 1.0340835, and a total of 52 patients were calculated, 26 participants for the experimental group, 26 participants for the control group. The patients were assigned to the experimental and control groups according to the order in which they came to the outpatient clinic. Without using a sampling method, 61 patients with depression who met the inclusion criteria, volunteered to participate in the study, and applied to the clinic at the data collection date of the study constituted the sample of the study. Furthermore, 30 depressive patients were included in the experimental group and the other 31 patients were included in the control group. However, the unsuitability of the home environment for the online interview with a patient in the experimental group could not be maintained, psychotic features were added to the depression table of one patient, two patients did not want to continue the interview, and the study was completed with 53 patients due to reasons such as one patient in the control group did not want to continue with the study and three patients could not be reached through their contact information.
Measures
Personal Information Form (PIF)
The personal information form prepared by the researcher (gender, age, educational level, marital status, employment status, cohabitation, history of hospitalization, suicidal ideation or attempt, and drug use) consists of a total of 10 questions.
Beck Depression Inventory (BDI)
The BDI was developed by Beck et al. (1979) and intended to measure somatic, emotional, cognitive, and motivational symptoms seen in depression. There are four options in each item of the BDI, which consists of 21 items. Each item gets a score between 0 and 3. By summing these scores, the depression score is obtained. The highest score that can be obtained is 63, and a high total score indicates a high level of depression. The BDI was adapted to Turkish society by Hisli (1988, 1989a, b). In the validity and reliability study of the BDI, the Cronbach’s α reliability coefficient was determined as 0.80. The Cronbach’s α reliability coefficient of BDI was found to be 0.94 in the present study.
Warwick-Edinburgh Mental Well-being Scale (WEMWBS)
It was developed by Tennant et al. (2007) to measure the mental well-being of individuals. The adaptation of the scale to Turkish society was made by Keldal in 2015. The WEMWBS consists of 14 items and deals with positive mental health levels of individuals, including psychological well-being and subjective well-being. The scale is in the form of 5-point Likert type and a minimum of 14 and a maximum of 70 points can be obtained from the scale. All items on the scale are positive. An increase in the score obtained from the scale indicates that the level of mental well-being increases. The Cronbach’s Alpha reliability coefficient of the scale was found 0.89 (Keldal, 2015). The Chronbach’s Alpha reliability coefficient of WEMWBS in the present study was found to be 0.97.
Life Attitude Profile-Revised Scale (LAP-R scale)
The LAP-R is a multidimensional life meaning scale developed to explore life motivation, the purpose and meaning of life. The scale was developed by Reker (1992). The scale was adapted to Turkish society by Erci (2008). The scale has 4 sub-dimensions: “Purpose, Coherence, Choice/Responsibleness, and Goal Seeking”. The scale is in the form of 7-point Likert type. The maximum total score on this scale is 210 and the minimum score is 30. As the score increases, the meaning in life and positive attitude towards life also increase (Erci, 2008). In the current study, the Chronbach’s alpha reliability coefficient was determined as 0.96.
Research process
Pre-tests (PIF, BDI, WEMWBS, and LAP-R Scale) were applied to the patients in the experimental and control groups included in the study before the program. In the first interview with the patients in the experimental group, information about the program was given and the days and hours of the program sessions were determined. The program was applied to the patients in the experimental group once a week for eight weeks. The program was implemented by the researcher (RK) who received training in positive psychology (received a certificate in positive psychology), with each session of 40–45 min. Sessions were held in the form of individual interviews. After the first face-to-face interview with the patients in the experimental group in which the program was applied, the interviews were continued in the form of online interviews (zoom, WhatsApp video call, etc.) using free software. Before the session, patients were called by phone and reminded of the time of the program. Post-tests of the experimental group (BDI, WEMWBS, and LAP-R Scale) were administered immediately after the program sessions were completed. In addition, follow-up tests (BDI, WEMWBS, and LAP-R Scale) were administered one month after the program was completed. In the control group, no intervention was made after the pre-test was applied; two months later, the post-tests and one month after the post-tests, follow-up tests were applied. The tests were applied in the form of Google Forms. The positive psychology program was applied in addition to the routine clinical treatment of the patients in the experimental group, and the patients in the control group continued to receive routine clinical treatment. At the end of the study, the training guide prepared according to the positive psychology program was shared with the patients in the control group in the digital environment.
Structure of the positive psychology program
The program emphasized the importance of using positive emotions, personal strengths, and meaningful relationships to promote relief from depression, distress, and life problems (Carr, 2016). From the beginning, patients were asked to introduce themselves by telling the real-life story that best presented them, and real and positive relationships were established. Individuals were asked to identify their strengths, and they were trained to find practical ways to use these strengths more frequently in the fields of work, love, play, friendship, and parenting, and various applications were made (Seligman et al., 2006). The program started with an orientation on how the absence of positive resources leads to depression. Positive psychology concepts are discussed (such as satisfaction, participation, and meaning). Participants were informed about the development of personal strengths and positive emotions and their impact on well-being. The effects of accumulating anger and pain on individuals’ depression and well-being were mentioned. The importance of forgiveness, appreciation, and gratitude in developing positive emotions was discussed. Participants were encouraged to gratification rather than the hedonic cycle. The place of hope and optimism in depression was mentioned. The importance of recognizing the strengths of family members was discussed. Ways to serve a greater purpose than oneself and to find meaning in life were discussed. Various assignments were used in the sessions, and feedback was received from these assignments and evaluated (Seligman et al., 2006) (Table 1).
Data analysis
The data of the study was analyzed in SPSS (Statistical Package for Social Sciences) 26 package program. In the analysis of the data, percentage distribution, mean and standard deviation, chi-square, t-test in dependent and independent groups, and variance analysis in repeated measurements, post hoc: Bonferroni method were used and the level of p < 0.05 was accepted as significant.
Results
The study included 53 participants, 26 of which were allocated to the experimental group, and 27 of them were allocated to the control group. The sociodemographic characteristics of the participants are presented in Table 2. No statistically significant difference was observed between the experimental and control groups, except for the time of diagnosis. It was seen that both groups were homogeneous in terms of these characteristics (Table 2).
When the BDI, WEMWBS, and LAP-R Scale pre-test, post-test, and follow-up test total mean scores of the experimental and control groups were examined between the groups, in the pre-test, the total mean score of the subscale of the purpose of those in the experimental group was lower than the total mean score of the participants in the control group (p = 0.036; p < 0.05). No statistically significant differences were observed between the other pre-test scores of the experimental and control groups (p > 0.05). In the post-test results, it was observed that the BDI (p < 0.001) total mean score of the participants in the experimental group was lower than the control group (p < 0.05). The experimental group’s total mean scores from the WEMWBS (p < 0.001), the LAP-R’s subscales of purpose (p < 0.001), coherence (p = 0.001), choice/responsibleness (p < 0.001), goal seeking (p < 0.001), and total LAP-R Scale (p < 0.001) were found to be significantly higher than the control group (p < 0.05). Considering the follow-up test results, it was determined that the BDI (p < 0.001) total mean scores of the participants in the experimental group were lower than the BDI total mean scores of the participants in the control group (p < 0.05). It was determined that the participants in the experimental group had higher total mean scores in the WEMWBS (p < 0.001), the LAP-R’s subscales of purpose (p < 0.001), coherence (p = 0.002), choice/responsibleness (p < 0.001), and the total LAP-R Scale (p = 0.003) than the participants in the control group (p < 0.05). No significant difference was observed between the experimental and control groups’ total mean scores on the subscale of goal-seeking (p = 0.292; p > 0.05) (Table 3).
The experimental group’s within-group comparisons of the total mean scores from the pre-test, post-test, and follow-up test BDI, WEMWBS, and LAP-R Scale are given in Table 4. The difference between the pre-test, post-test, and follow-up tests’ total mean scores from the BDI, WEMWBS, and LAP-R Scale of the patients in the experimental group was found to be statistically significant (p < 0.05). In the Bonferroni correction made to determine which group caused this difference, a significant difference was found between the BDI, WEMWBS, LAP-R Scale’s pre-test, post-test, and follow-up test total mean scores (p < 0.001).
As a result of the examination, the differences between the pre-test and post-test scores of the participants in the experimental group in the p1 column were examined. The experimental group’s post-test BDI total mean score was lower than the pre-test BDI total mean scores (p < 0.001); however, the experimental group’s post-test WEMWBS (p < 0.001), the LAP-R’s subscales of Purpose (p < 0.001), Coherence (p < 0.001), Choice/Responsibleness (p < 0.001), Goal Seeking (p < 0.001), and the total LAP-R Scale (p < 0.001) total mean scores were found to be significantly higher (p < 0.05).
In the p2 column, the differences between the pre-test and follow-up test scores of the participants in the experimental group were examined. The experimental group’s follow-up test BDI total mean score was significantly lower compared to the pre-test (p < 0.001); however, the follow-up test WEMWBS (p < 0.001), the LAP-R’s subscales of purpose (p < 0.001), coherence (p < 0.001), choice/responsibleness (p < 0.001), and the total LAP-R Scale (p < 0.001) total mean scores were significantly higher compared to the pre-test (p < 0.05). In the total mean score of the LAP-R’s subscale of Goal Seeking, the pre-test and post-test results were found to be homogeneous (p = NA).
In the p3 column, the differences between the post-test and follow-up test results of the participants in the experimental group were examined. As a result of the examination, it was determined that the post-test total mean scores of the experimental group from the total LAP-R Scale (p = 0.002) and its subscale of goal seeking (p < 0.001) were significantly higher compared to the follow-up test (p < 0.05). No significant difference was observed between the post-test and the follow-up test results of the other scales (p > 0.05) (Table 4).
The within-group comparisons of the pre-test, post-test, and follow-up test BDI, WEMWBS, and LAP-R Scale total mean scores of the control group are presented in Table 5. The difference between the pre-test, post-test, and follow-up test total mean scores from the BDI, WEMWBS, and LAP-R Scale of the patients in the control group was not statistically significant (p > 0.05). In the Bonferroni correction made to determine which group caused this difference, no significant difference was found between the pre-test, post-test, and follow-up test BDI, WEMWBS, and LAP-R Scale total mean scores (p > 0.05) (Table 5).
Discussion
The most important contribution of positive psychology to practice is ‘Positive Psychology Interventions’. (Sin & Lyubomirsky, 2009). Bolier et al. (2013a, b) suggested that interventions should be developed in accordance with the theoretical tradition of positive psychology (Bolier et al., 2013a). Parks and Biswas-Diener (2013) added that in order for an intervention to be considered as a PPI, there must be empirical evidence for the effectiveness of that intervention (Hendriks et al., 2020). As a result of their research, Lopez-Gomez et al. (2017a, b) stated that more research is needed on the applicability of PPI in clinical settings in order to offer a wider variety of acceptable and appropriate treatments for depression patients (Lopez-Gomez et al., 2017a). It has been determined that there is a deficiency in the national literature on this subject. In the international literature, it has been seen that the effects of PPI on depression and/or well-being have been examined by applying it to different sample groups (such as employees and students) as programs with internet-based modules (not as online live interviews) (Yuan et al., 2014; Chilver & Gatt, 2022; Zhang et al., 2020). However, studies examining the effectiveness of a positive psychology program on depression, well-being, and life attitude in individuals diagnosed with depression in the form of online live interviews could not be found. Therefore, the results of the study were discussed in this direction.
In this study, before the application of the positive psychology program, the BDI total mean score of the patients in the experimental group was 30.5 ± 12.2, and 23.3 ± 14.2 in the control group. In line with the analysis, it can be said that the depression scores of the patients in this study were quite high before the positive psychology program. When the pre-test, post-test, and follow-up test BDI total mean scores of the experimental group that received the positive psychology program and the control group that did not receive the positive psychology program were compared between the groups, it was determined that there was no significant difference in depression levels between the experimental and control groups before the positive psychology program. After the program, when the post-test BDI total mean scores of the experimental and control groups were compared between the groups, a significant decrease was observed in the depression level of the experimental group compared to the control group. It was determined that this significant decrease continued in the comparison of the follow-up test BDI total mean scores of the experimental and control groups one month after the end of the program. In this study, when the within-group comparisons of the experimental group were examined, it was observed that there was a decrease in the post-test and follow-up test BDI total mean scores compared to the pre-test. When the within-group comparisons of the control group were examined, no decrease was found in the total mean scores of the post-test and follow-up test BDI compared to the pre-test. The significant decrease in the experimental group’s BDI total mean scores in the post-test and follow-up test indicates that the positive psychology program applied to patients with depression was successful.
In meta-analysis studies conducted to evaluate the effectiveness of positive psychology interventions, it was determined that interventions reduced depressive symptoms (Sin & Lyubomirsky, 2009; Bolier et al., 2013a; Pan et al., 2022). In addition, the results of studies in the literature presented that it would be good if the researchers offered positive psychology interventions as individual (versus group) therapy and for relatively longer durations (Sin & Lyubomirsky, 2009; Bolier et al., 2013a; Pan et al., 2022). In the present study, sessions of the positive psychology program were applied online individually. It was thought that online individual interviews provide an opportunity for patients to express themselves more easily.
In the literature, studies that included individuals with symptoms of depression or patients diagnosed with major depression and dysthymia were reported to reduce depression levels with positive psychology interventions (Seligman et al., 2006; Carr et al. 2017; Hanson 2019; Lopez-Gomez et al., 2017a, b, Furchtlehner et al., 2020).
Shapira and Mongrain (2010) applied a program that included positive psychology practices such as self-compassion and optimism to individuals in their study, which included individuals with depressive characteristics. As a result of the study, a decrease in depressive symptoms was observed (Shapira & Mongrain, 2010). Again, Cheavens et al. (2006) measured the effectiveness of hope therapy on 32 participants with various mental disorders (such as Major Depression, Dysthymia, Remission MD, and Single-episode MD) and determined that individuals in the intervention group had a decrease in depressive symptoms compared to individuals in the control group (Cheavens et al., 2006). It is known that individuals have a negative view of the future when they are depressed. In our study, patients were asked to write about how they see themselves in the best possible place in the future, with applications on optimism and hope (thinking about the best scenario, asking questions about hope). Immediately after the exercise, patients reported that although the activity was easy to do, it provided them with serious benefits. It was observed that they continued this activity in the follow-up phase.
In studies on the effectiveness of positive psychology interventions in different populations with mild and moderate depressive symptoms, it was reported that interventions significantly reduced depression (Bolier et al., 2013b; Hernandez et al., 2018; Taghvaienia & Zonobitabar, 2020; Gao et al., 2021).
Freedman and Enright (1996) investigated the effectiveness of forgiveness therapy in their study. As a result of the research, they found a significant decrease in the symptoms of depression in the individuals (Freedman & Enright, 1996). Our research sessions also focused on the subject of ‘forgiveness’. In our exercise on forgiveness (forgiveness letter), we received feedback from some patients that they had some difficulty in starting and completing the exercise. Furthermore, they reported that it was difficult to express their thoughts on both the issues they could not forgive themselves and the issues related to those around them. However, they stated that they experienced serious ‘relaxation’ after the practice. Feelings of guilt can arise in depression. In line with the feedback received from the patients participating in the study, it is thought that the exercise of forgiveness contributes to revealing and managing “the feelings of guilt”.
When the effects of nine strength-based positive psychology interventions on well-being and depression by Gander et al. (2013) were examined within the framework of an internet-based randomized placebo-controlled study, it was stated that in a population of 622 adult individuals, all of the interventions reduced the level of depression (Gander et al., 2013). In our study, it is thought that the practices performed to determine the strengths of family members contribute to the regulation of partner relations in particular. Again, it has been seen that the identification of personal strengths and the exercise of using these characteristics are beneficial in the management of feelings of worthlessness that occur in depression.
According to the results obtained as a result of the research, it has been seen that the positive psychology program can be used as an effective method in the treatment of depression. The ideas behind positive psychology interventions can be listed as increasing well-being, building positive resources for the individual, and weakening or eliminating many factors that can cause depression to persist, such as pessimism or low self-esteem (Akhtar, 2012). These interventions are based on Seligman’s conceptualizations of happiness and well-being (Wood & Johnson, 2021).
In this study, before the positive psychology program, the WEMWBS total mean score of the patients in the experimental group was 30.0 ± 13.1 and 37.1 ± 15.9 in the control group. Before the program, in the pre-test, when the experimental and control groups were compared between the groups, no significant difference was found in terms of mental well-being. After the program, when the experimental and control groups were compared between the groups, the mental well-being level of the experimental group was found to be significantly higher than the control group. It was determined that this difference persisted in the follow-up test performed one month later. In the within-group comparisons of the patients in the experimental group, significant differences were found in the pre-test, post-test, and follow-up tests. No significant differences were found in the pre-test, post-test, and follow-up tests when the patients in the control group were compared within the group.
In the study of Shapira and Mongrain (2010), in which they applied positive psychology interventions (self-compassion, optimism) and included individuals with depressive symptoms, an increase in well-being was observed as well as a decrease in depressive symptoms (Shapira & Mongrain, 2010). In the systematic review and meta-analysis studies conducted by Carr et al. (2021) on the effectiveness of positive psychology interventions, positive psychology interventions were reported to have small to moderate significant effects on well-being (g = 0.39), strengths (g = 0.46), quality of life (g = 0.48). ), depression (g = -0.39) and anxiety (g = -0.62) (Carr et al., 2021). Additionally, according to the meta-analysis results of Bolier et al. (2013a, b), positive psychology interventions were effective in increasing subjective and psychological well-being (Bolier et al., 2013a). In the same meta-analysis studies of Sin and Lyubomirsky (2009), it was stated that positive psychology interventions significantly increased well-being (Sin & Lyubomirsky, 2009). In the literature, it is possible to come across studies indicating that PPI increases the well-being of patients in studies including patients with depression symptoms or diagnosed with major depression and dysthymia (Asgharipoor et al., 2012; Lopez-Gomez et al., 2017b).
In the same study, Freedman and Enright (1996) stated that there was an increase in the well-being of individuals as a result of the application of forgiveness therapy (Freedman & Enright, 1996).
In the literature, there are studies showing that when depressive symptoms increase, well-being decreases (Ahmed et al., 2020). Our study has presented that positive psychology program has increased mental well-being. Well-being includes many factors such as contentment, life satisfaction, and positive emotions. Factors related to well-being were discussed in our positive psychology program sessions (e.g. the subject of gratitude). People who are more grateful for life appreciate both their self and positive values in the world, as well as the future. Considering Beck et al’s model of depression, which includes the “negative triad” of negative views about the self, the world, and the future, this suggests that gratitude plays a key role in determining mental health. Gratitude can form a “positive triad” of positive views on self, the world, and (depending on the variance it shares with optimism) the future (Wood & Johnson, 2021). In this context, it is thought that adding positive psychology practices that address these issues to the treatment of depression may contribute to the management of depression by increasing well-being.
Positive psychology practices do not suggest treatment by focusing only on negative symptoms; it also recommends treatment by promoting positive emotions, psychological strengths, and meaningful living (Bolier et al., 2013a; Chaves et al., 2017). Positive psychology strategies, such as increasing positive emotions, develop personal strengths. Patients’ seeking direction, meaning, and participation in their daily lives appear to be potential tools for the prophylaxis and treatment of depression as well as the prevention of recurrences by reducing symptoms (Santos et al., 2013).
There are studies indicating that interventions based on enjoyment, participation, and meaning are effective in increasing well-being and relieving depressive symptoms for longer periods of time (Gander et al., 2016), and there are sessions for these components in the positive psychology program we implemented.
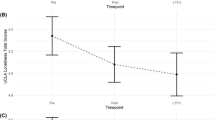
In this study, in the comparison of the pre-test LAP-R Scale total mean score of the experimental group to which the positive psychology program was applied and the control group’s patients who were not applied to the positive psychology program, no significant difference was found in the total mean scores, except for the subscale of ‘Purpose’. After the program, in the comparison of the experimental and control groups, the LAP-R Scale total mean score of the experimental group was found to be significantly higher than the control group. It has been seen that this significant difference continues in the total mean scores of the subscales, except for the subscale of ‘Goal Seeking’ in repeat measurements made at the one-month follow-up. In the within-group comparisons of the patients in the experimental group, significant differences were found in the pre-test, post-test, and follow-up test. In the within-group comparison of the control group, no significant differences were found between the LAP-R Scale total mean scores in the pre-test, post-test, and follow-up test.
Cheavens et al. (2006), in their study in which they measured the effectiveness of hope therapy, which is a positive psychology intervention, determined that there was a greater increase in the meaning of life in the individuals of the intervention group compared to the individuals of the control group (Cheavens et al., 2006).
Seligman (2002) later proposed three pathways to well-being, including positive relationship and achievement, namely pleasure-seeking, meaning-seeking, and participation-seeking (Gander et al., 2016). Connecting individuals with something bigger than themselves in their lives (such as helping someone in distress, or doing community service) and creating a source where they can find meaning can prevent them from being aimless. It is thought that individuals can manage depressive symptoms appropriately by developing positive life attitudes in this way. These topics were also included in the sessions of the positive psychology program that we applied in our study. As a result of our study, it is thought that positive psychology practices may create an option in the treatment of depression by contributing to the development of positive life attitudes of the patients. With the addition of these interventions to the treatment of depression, it is predicted that the range of existing interventions used in the treatment will expand.
Conclusion
As a result, it was determined that the online positive psychology program was effective in reducing the depression levels of depressed patients, increasing their well-being and positive life attitude. In this direction, it can be recommended that nurses benefit from PPI and evidence-based guidelines while providing holistic care. It can be suggested that psychiatric nurses increase their knowledge and skills by participating in certificate programs related to positive psychology practices. As a result of preferring more accessible and cost-effective methods together with the advantages of developing technology, the widespread use of online positive psychology programs in the treatment of depression, application of positive psychology practices in the form of online interviews to larger sample groups in order to be an intervention that can be applied in case of re-experiencing of pandemic processes such as COVID-19, and the execution of studies comparing online positive psychology practices with face-to-face positive psychology practices are recommended.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding authors on reasonable request.
References
Ahmed, M. Z., Ahmed, O., Aibao, Z., Hanbin, S., Siyu, L., & Ahmad, A. (2020). Epidemic of COVID-19 in China and associated psychological problems. Asian Journal of Psychiatry, 51, 102092. https://doi.org/10.1016/j.ajp.2020.102092
Akhtar, M. (2012). Positive psychology for overcoming depression: self-help strategies for happiness, inner strength and well-being. Watkins.
Asgharipoor, N., Farid, A., Arshadi, A., & Sahebi, A. (2012). A comparative study on the effectiveness of positive psychotherapy and group cognitive-behavioral therapy for the patients suffering from major depressive disorder. Iranian Journal of Psychiatry and Behavioral Sciences, 6(2), 33–41.
Beck, A. T., Rush, A. J., Shaw, B. F., & Emery, G. (1979). Cognitive therapy of depression. Guilford Press.
Bolier, L., Haverman, M., Westerhof, G. J., Riper, H., Smit, F., & Bohlmeijer, E. (2013a). Positive psychology interventions: a meta-analysis of randomized controlled studies. BMC Public Health, 13, 119. https://doi.org/10.1186/1471-2458-13-119
Bolier, L., Haverman, M., Kramer, J., Westerhof, G. J., Riper, H., Walburg, J. A., Boon, B., & Bohlmeijer, E. (2013b). An internet-based intervention to promote mental fitness for mildly depressed adults: randomized controlled trial. Journal of Medical Internet Research, 15(9), e200. https://doi.org/10.2196/jmir.2603
Burns, D. (2015). Feeling good. İyi Hissetmek, 19. Ed., Karaosmanoğlu HA. Psikonet.
Button, K. S., Kounali, D., Thomas, L., Wiles, N. J., Peters, T. J., Welton, N. J., Ades, A. E., & Lewis, G. (2015). Minimal clinically important difference on the Beck depression inventory–II according to the patient’s perspective. Psychological Medicine, 45(15), 3269–3279. https://doi.org/10.1017/S0033291715001270
Carr, A. (2016). Positive psychology the science of happiness and human strengths. Pozitif Psikoloji-Mutluluğun ve İnsanın Güçlü Yönlerinin Bilimi, 1. Baskı, Şendilek Ü, Kaknüs Yayınları.
Carr, A., Cullen, K., Keeney, C., Canning, C., Mooney, O., Chinseallaigh, E., & O’Dowd, A. (2021). Effectiveness of positive psychology interventions: a systematic review and metaanalysis. The Journal of Positive Psychology, 16(6), 749–769. https://doi.org/10.1080/17439760.2020.1818807
Carr, A., Finnegan, L., Griffin, E., Cotter, P., & Hyland, A. (2017). A randomized controlled trial of the say yes to life (sytl) positive psychology group psychotherapy program for depression: an interim report. Journal of Contemporary Psychotherapy, 47, 153–161. https://doi.org/10.1007/s10879-016-9343-6
Chaves, C., Lopez-Gomez, I., Hervas, G., & Vazquez, C. A. (2017). Comparative study on the efficacy of a positive psychology ıntervention and a cognitive behavioral therapy for clinical depression. Cognitive Therapy and Research, 41, 417–433. https://doi.org/10.1007/s10608-016-9778-9
Cheavens, J. S., Feldman, D. B., Gum, A., Michael, S., & Snyder, C. R. (2006). Hope therapy in a community sample: a pilot ınvestigation. Social Indicators Research, 77, 61–78. https://doi.org/10.1007/s11205-005-5553-0
Chilver, M. R., & Gatt, J. M. (2022). Six-week online multi-component positive psychology ıntervention ımproves subjective wellbeing in young adults. Journal of Happiness Studies, 23(3), 1267–1288. https://doi.org/10.1007/s10902-021-00449-3
WHO-Depression. (2021). https://www.who.int/news-room/fact-sheets/detail/depression. Accessed 20 May 2022
Erci, B. (2008). Meaning in life for patients with cancer: validation of the life attitude profile-revised scala. Journal of Advanced Nursing, 62(6), 704–711.
Eryılmaz, A. (2017). Pozitif psikoterapiler. Psikiyatride Güncel Yaklaşımlar, 9(3), 346–362. https://doi.org/10.18863/pgy.288667
Freedman, S. R., & Enright, R. D. (1996). Forgiveness as an intervention goal with incest survivors. Journal of Consulting and Clinical Psychology, 64(5), 983–992. https://doi.org/10.1037/0022-006X.64.5.983
Furchtlehner, L. M., Schuster, R., & Laireiter, A. R. (2020). A comparative study of the efficacy of group positive psychotherapy and group cognitive behavioral therapy in the treatment of depressive disorders: a randomized controlled trial. The Journal of Positive Psychology, 15, 832–845. https://doi.org/10.1080/17439760.2019.1663250
Gander, F., Proyer, R. T., & Ruch, W. (2016). Positive psychology interventions addressing pleasure, engagement, meaning, positive relationships, and accomplishment increase well-being and ameliorate depressive symptoms: a randomized, placebo-controlled online study. Frontiers in Psychology, 7, 686. https://doi.org/10.3389/fpsyg.2016.00686
Gander, F., Proyer, R. T., Ruch, W., & Wyss, T. (2013). Strength-based positive ınterventions: further evidence for their potential in enhancing well-being and alleviating depression. Journal of Happiness Studies, 14, 1241–1259. https://doi.org/10.1007/s10902-012-9380-0
Gao, X. J., Sun, J. J., & Xiang, M. (2021). Positive psychological intervention for anxiety, depression and coping in subjects addicted to online games. World Journal of Clinical Cases, 9(14), 3287–3293. https://doi.org/10.12998/wjcc.v9.i14.3287
Gilbert, P. (2009). Depression-overcoming depression. Depresyon-Üstesinden Gelmek (2, 29–35). Baskı, & Yener, N. Kuraldışı Yayıncılık.
Hanson, K. (2019). Positive psychology for overcoming symptoms of depression: a pilot study exploring the efficacy of a positive psychology self-help book versus a cbt self-help book. Behavioural and Cognitive Psychotherapy, 47, 95–113. https://doi.org/10.1017/S1352465818000218
Hendriks, T., Schotanus-dijkstra, M., Hassankhan, A., de Jong, J., & Bohlmeijer, E. (2020). The efficacy of multi-component positive psychology interventions: a systematic review and Meta-analysis of Randomized controlled trials. Journal of Happiness Studies, 21(1), 357–390. https://doi.org/10.1007/s10902-019-00082-1
Hernandez, R., Burrows, B., Wilund, K., Cohn, M., Xu, S., & Moskowitz, J. T. (2018). Feasibility of an internet-based positive psychological intervention for hemodialysis patients with symptoms of depression. Social Work in Health Care, 57(10), 864–879. https://doi.org/10.1080/00981389.2018.1523268
Hisli, N. (1988). Beck depresyon envanterinin geçerliği üzerine bir çalışma. Psikoloji Dergisi, 6(22), 118–122.
Hisli, N. (1989a). Validity and reliability of Beck depression scale in university students. Turkish Journal of Psychology, 7(3), 13–19.
Hisli, N. (1989b). Beck depresyon envanterinin üniversite öğrencileri için geçerliği güvenirliği. Psikoloji Dergisi, 23, 3–1.
Işık, A. H., & Güler, İ. (2010). Teletıpta mobil uygulama çalışması ve mobil iletişim teknolojilerinin analizi. Bilişim Teknolojileri Dergisi, 3(1), 1–10.
Keck, M. E. (2010). Depresyon, nasıl ortaya çıkar? Nasıl tedavi edilir? Stresle bağlantısı nedir? Version 1.0.
Keldal, G. (2015). Warwick-Edinburgh mental iyi oluş ölçeği’nin Türkçe formu: geçerlik ve güvenirlik çalışması. The Journal of Happiness & Well-Being, 3(1), 103–115.
Kleinman, P. (2013). Psych101-psychology facts, basics, statistics, tests and more. Psiko101-Psikolojinin Gerçekleri, Temel Ögeler, İstatistikler, Testler ve Daha Fazlası!., 2. Basım, Kaplan H, Okyanus Yayınları.
Lam, R. W. (2018). Depression (3rd Edition). Oxford University Press.
Leimon, A., & McMahon, G. (2009). Positive psychology for dummies. Pozitif Psikoloji for Dummies, 1. Baskı, Tanıl E, Nobel Yaşam, Ankara, 2018.
Lopez-Gomez, I., Chaves, C., Hervas, G., & Vazquez, C. (2017a). Comparing the acceptability of a positive psychology intervention versus a cognitive behavioural therapy for clinical depression. Clinical Psychology & Psychotherapy,24(5), 1029–1039. https://doi.org/10.1002/cpp.2129
Lopez-Gomez, I., Chaves, C., Hervas, G., & Vazquez, C. (2017b). Pattern of changes during treatment: a comparison between a positive psychology ıntervention and a cognitive behavioral treatment for clinical depression. The Spanish Journal of Psychology, 20. https://doi.org/10.1017/sjp.2017.44
Mental Health Action Plan. (2013–2020). https://www.who.int/mental_health/publications/action_plan/en/. Accessed: 13.12.2018.
Ogueji, I. A., Amusa, A. O., Olofe, O. J., & Omotoso, E. B. (2022). Willingness and barriers to utilizing e-therapy services: a nigerian general population qualitative study. Journal of Human Behavior in the Social Environment, 32(2), 214–228. https://doi.org/10.1080/10911359.2021.1894300
Pan, S., Ali, K., Kahathuduwa, C., Baronia, R., & Ibrahim, Y. (2022). Meta-analysis of positive psychology interventions on the treatment of Depression. Cureus, 14(2), e21933. https://doi.org/10.7759/cureus.21933
Parks, A. C., & Biswas-Diener, R. (2013). Positive interventions: Past, present, and future. In T. B. Kashdan & J. Ciarrochi (Eds.), Mindfulness, acceptance, and positive psychology: The seven foundations of well-being (pp. 140–165). New Harbinger Publications Inc.
Pazar, B., Taştan, S., & İyigün, E. (2015). Tele sağlık sisteminde hemşirenin rolü. Bakırköy Tıp Dergisi, 11(1), 1–4.
Reker, G. T. (1992). The life attitude profile- revised (LAP-R). Student Psychologists Press.
Santos, V., Paes, F., Pereira, V., Arias-Carrión, O., Silva, A. C., Carta, M. G., Nardi, A. E., & Machado, S. (2013). The role of positive emotion and contributions of positive psychology in depression treatment: systematic review. Clinical Practice and Epidemiology in Mental Health: CP & EMH, 9, 221–237. https://doi.org/10.2174/1745017901309010221
Seligman, M. E. P. (2002). Authentic happiness. Free Press.
Seligman, M., & Flourish, A. (2011). Visionary New understanding of happiness and wellbeing- what is well being? Free Press.
Seligman, M. E., Rashid, T., & Parks, A. C. (2006). Positive psychotherapy. American Psychologist, 61(8), 774–788. https://doi.org/10.1037/0003-066X.61.8.774
Shapira, L. B., & Mongrain, M. (2010). The benefits of self-compassion and optimism exercises for individuals vulnerable to depression. The Journal of Positive Psychology, 5(5), 377–389. https://doi.org/10.1080/17439760.2010.516763
Sin, N. L., & Lyubomirsky, S. (2009). Enhancing well-being and alleviating depressive symptoms with positive psychology interventions: a practice friendly meta- 60 analysis. Journal of Clinical Psychology, 65, 467–487. https://doi.org/10.1002/jclp.20593
Taghvaienia, A., & Zonobitabar, A. (2020). Positive intervention for depression and teacher-student relationship in iranian high school girl students with moderate/mild depression: a pilot randomized controlled trial. Child and Adolescent Psychiatry and Mental Health, 14, 25. https://doi.org/10.1186/s13034-020-00331-9
Tennant, R., Hiller, L., Fishwick, R., Platt, S., Joseph, S., Weich, S., Parkinson, J., Secker, J., & Stewart-Brown, S. (2007). The Warwick-Edinburgh mental well-being scale (WEMWBS): Development and UK validation. Health and Quality of Life Outcomes, 5, 63. https://doi.org/10.1186/1477-7525-5-63
Turkey, GHD. (2022). https://www.who.int/data/gho/data/countries/country-details/GHO/turkey?countryProfileId=e15ebd1a-7ed0-4d05-9659-98efa265037a. Accessed: 25.12.
Waters, L., Cameron, K., Nelson-Coffey, S. K., Crone, D. L., Kern, M. L., Lomas, T., Oades, L., Owens, R. L., Pawelski, J. O., Rashid, T., Warren, M. A., White, M. A., & Williams, P. (2021). Collective wellbeing and posttraumatic growth during covid-19: how positive psychology can help families, schools, workplaces and marginalized communities. The Journal of Positive Psychology. Advance online publication. https://doi.org/10.1080/17439760.2021.1940251
Wood, A. M., & Johnson, J. (2021). The Wiley handbook of positive clinical psychology. Pozitif Klinik Psikoloji, İ Dağ, Z Maçkalı (Çev Ed.) Nobel Akademik Yayıncılık.
Yuan, Q., Liu, S., Tang, S., & Zhang, D. (2014). Happy@Work: protocol for a web-based randomized controlled trial to improve mental well-being among an asian working population. BMC Public Health, 14, 685. https://doi.org/10.1186/1471-2458-14-685
Zhang, X. Q., Zhang, B. S., & Wang, M. D. (2020). Application of a classroom-based positive psychology education course for chinese medical students to increase their psychological well-being: a pilot study. BMC Medical Education, 20(1), 323. https://doi.org/10.1186/s12909-020-02232-z
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Strengths and limitations
Strengths of the study; the use of an up-to-date approach (online positive psychology program) in the treatment of depression. The follow-up period is limited to 1 month since the research was conducted between certain dates ve the fact that the sample was obtained from a single center and its limited number is one of the limitations of the study.
Ethical approval
Before starting the research, written and verbal permission was obtained from the center where the research would be conducted. Approval was obtained from Gaziantep University’s Clinical Research Ethics Committee (Ethics Committee Decision Number: 169) to conduct the study. During the collection of the research data, the individuals were made to sign the “Informed Consent Form” about the research. The principle of “Respect for Autonomy” has been fulfilled by stating that they are free to participate in the research and to leave whenever they want after the participation of the individuals, and the principle of “Confidentiality and Protection of Confidentiality” has been fulfilled by stating that the information of the patients participating in the research will be kept confidential. All procedures performed in this study involving human participants were in accordance with the ethical standards of the research team’s organizational Ethics Board and with the 1975 Helsinki Declaration.
Conflict of interest
No potential conflict of interest was reported by the authors.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kaya, R., Tanrıverdi, D. The effect on mental well-being, life attitude and depression levels of positive psychology program applied to patients diagnosed with depression. Curr Psychol 43, 119–131 (2024). https://doi.org/10.1007/s12144-023-04244-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-023-04244-6