
Abstract
We examined person-centered heterogeneity in the longitudinal co-development of depression and alcohol problems during the COVID-19 outbreak. We also investigated the risk factors (personality and coping) for being in “higher” relative to “lower” risk subgroups of combined depressive symptoms and alcohol problems. Canadian participants (N = 364, Mage = 32.16, 54.67% male) completed questionnaires four times every three months, starting approximately 2 months after Canada announced its COVID-19 State-of-Emergency. Parallel-process latent class growth analysis found evidence for three latent subgroups: a “moderate increasing depression and alcohol problems” subgroup (Class 1); a “moderate stable depression, moderate decreasing alcohol problems” subgroup (Class 2); and a “low-risk normative” subgroup (with mild depression that was stable and mild alcohol problems that decreased; Class 3). Multinomial logistic regressions found that higher levels of hopelessness, impulsivity, and boredom proneness distinguished Class 1 from Class 3. Further, lower levels of general self-efficacy distinguished Class 1 from Classes 2 and 3. Linear mixed models found that Class 1 increasingly used maladaptive avoidant coping strategies (denial, drugs/alcohol, behavioural disengagement) as the pandemic progressed, whereas Class 2 increasingly used adaptive approach-oriented strategies (planning, seeking emotional support from others). We analyzed longitudinal data to detect classes of individuals with depressive and alcohol-related difficulties during COVID-19 and to characterize the vulnerability factors for increased difficulties. Highlighting the heterogeneity in the co-trajectory of depression and alcohol problems during COVID-19 and the personality and coping factors associated with combined increases in these mental health difficulties can inform treatment practices and bolster peoples’ preparedness and resilience for future pandemics.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
The global coronavirus (COVID-19) pandemic has significantly impacted the mental health of people worldwide. Among 1,803 Canadian adults surveyed in late-April 2020, roughly two months after Canada announced its COVID-19 State-of-Emergency, the percentage of respondents with high self-reported depression had increased from 4 percent to 10 percent since the beginning of the pandemic. One-third of respondents with depression additionally reported increased alcohol consumption since the beginning of COVID-19 (Dozois, 2021), and a separate study (McPhee et al., 2020) found that depression severity and risky drinking were greater in May 2020, after social distancing guidelines were introduced, relative to pre-social distancing. Although some studies found increases in alcohol consumption and alcohol problems during the pandemic (e.g., Pollard et al., 2020; Tucker et al., 2022), the results of studies have been mixed, with most finding that certain subgroups, such as those with depressive symptoms, report an increase in their alcohol consumption and alcohol problems (Acuff et al., 2022; Baptist-Mohseni et al., 2022; Capasso et al., 2021; Shield et al., 2022). This underscores the need to study depression and alcohol-related difficulties jointly for a well-rounded understanding of how the pandemic has impacted peoples’ mental health and well-being.
The complexity in the comorbidity of depression and alcohol problems
Importantly, while much of the literature supports an associative link between depression and alcohol consumption (Khantzian, 1997, 2012), many individuals who struggle with depression symptoms do not problematically consume alcohol (e.g., Pedrelli et al., 2016). Indeed, some studies find a low-to-moderate comorbidity prevalence (4–37 percent) between major depressive disorder and alcohol use disorder within the general population (see Castillo-Carniglia et al., 2019 for a review). Notably, longitudinal research suggests that even over time, the co-trajectories of depression and alcohol problems (the adverse consequences of alcohol consumption) is not uniform or consistent across all adults. In particular, Frohlich and colleagues (2018) and Orui and colleagues (2020) conducted longitudinal studies examining the heterogeneity in the co-trajectories of depressive symptoms and alcohol problems among Canadians after and during university, respectively. In both studies, participants completed measures of depression and alcohol problems over the course of 12–18 months and the authors used parallel-process latent class growth analysis (LCGA) to classify groups of individuals based on the simultaneous growth of these difficulties. This novel analysis has advantages relative to other statistical analyses because it studies the comorbidity of psychological processes over time, which allows researchers to identify distinct unobserved (latent) classes of individuals with the same developmental trajectories (see Muthen & Muthen, 2000). This person-centered analytical approach models heterogeneous longitudinal data by classifying individuals into smaller classes or subgroups with homogenous co-patterns of psychological processes over time.
Frohlich and colleagues (2018) and Orui and colleagues (2020) identified multiple latent classes of depression and alcohol problems, most consistently: a “high-risk” (comorbid) class, who had high depression that was stable and high alcohol problems that were stable; a “moderate-risk” (depression-only) class, who had high depression that was stable and low alcohol problems (Orui et al., 2020 found that the latter decreased among participants in this class, whereas Frohlich et al., 2018 found that the latter remained stable among participants in this class); and a “low-risk” (normative) class, who had low depression that was stable and low alcohol problems that decreased. Together, these studies highlight the heterogeneity and hence, complexity in the comorbidity of depression and alcohol problems over time.
Unfortunately, at the time of writing the present work, the number of COVID-19 cases and deaths continue to rise, indicating that COVID-19 remains a global health emergency (World Health Organization, 2022). Equally troubling, epidemiological research suggests that the probability of future pandemics that are comparable to COVID-19 in severity is increasing (e.g., Marani et al., 2021). Accordingly, continued scholarship on the impact of the pandemic on peoples’ mental health is important because it can advance prevention and intervention practices and strengthen peoples’ preparedness and resilience during these and other extraordinary times. As depression and problem drinking are clear concerns in the context of COVID-19, the current study meaningfully extended on prior research, using parallel-process LCGA to study the longitudinal co-trajectories of depression and alcohol problems in adults during the pandemic.
Risk factors for comorbid depression and alcohol problems
While identifying specific subgroups of depression and alcohol problems during the pandemic is imperative, it is equally critical to establish the factors that can increase one’s risk for being in the “high-risk” subgroup of elevated depressive symptoms and alcohol problems, in comparison to the other subgroups. Doing so can elucidate which people are at greater risk for combined depression and alcohol problems and which factors are important targets for prevention strategies and intervention approaches during such stressful circumstances. In their study, Orui et al. (2020) found that higher levels of hopelessness, impulsivity, and anxiety sensitivity differentiated the “high-risk” subgroup from the “low-risk” subgroup; higher levels of hopelessness differentiated the “moderate-risk” subgroup from the “low-risk” subgroup; and higher levels of impulsivity and lower levels of hopelessness differentiated the “high-risk” subgroup from the “moderate-risk” subgroup. In addition to these personality traits explored by Orui et al. (2020), the current study examined other factors and mechanisms that are relevant to the pandemic and that may distinguish the “high-risk” subgroup from other subgroups of combined depression and alcohol problems: boredom proneness, general self-efficacy, external stressors, and coping strategies.
Boredom proneness refers to the tendency to frequently and intensely feel bored, which is “the aversive experience of having an unfulfilled desire to engage in satisfying activity” (Fahlman et al., 2013, p. 69). Research during the COVID-19 outbreak, as well as the SARS outbreak, suggest that boredom is one of the most commonly experienced feelings associated with social distancing/quarantine (Barari et al., 2020; Droit-Volet et al., 2020; Reynolds et al., 2008), as well as that boredom proneness impairs peoples’ adherence to such critical public health measures (see Westgate et al., 2022 for a review). Three cross-sectional studies published during COVID-19 suggest a positive relationship between boredom proneness and depression symptoms (McCurdy et al., 2022; Weiss et al., 2022; Yan et al., 2021), while most studies published during COVID-19 suggest that state boredom is positively linked to depressive symptoms and alcohol consumption (e.g., Canadian Centre on Substance Use & Addiction, 2020; Chao et al., 2020; Droit-Volet et al., 2020; Schmits & Glowacz, 2022). Given its characterization, it is plausible that boredom proneness would be a risk factor for “high-risk” depression and alcohol problems. Some work (Danckert et al., 2018) proposes that boredom proneness represents a chronic failure to respond adaptively to the state of boredom, such that people seek unhealthy experiences (e.g., self-harm) to alleviate boredom—even if other negative states are elicited (e.g., Bench & Lench, 2019; Havermans et al., 2015). Other work suggests that boredom proneness represents the general tendency toward maladaptive motivations—irrespective of the state of boredom—such as the desire to act destructively, the desire to act without thinking things through, the desire to avoid one’s emotions, uncertainty (not knowing what to do), and amotivation (not caring to do anything; Bambrah et al., 2020).
The pandemic has additionally engendered significant difficulties with self-efficacy, which are the beliefs in one’s abilities to meet given situational demands (Wood & Bandura, 1989). Indeed, several published studies found that self-efficacy was low or declined (compared to before the pandemic) across various samples (e.g., teachers, nurses, mental health workers, first-time parents; Cataudella et al., 2021; Pressley & Ha, 2021; Simonetti et al., 2021; Sun et al., 2020; Xue et al., 2021; Yildirim & Güler, 2020). General self-efficacy, a trait-like dimension of self-efficacy conceptualized as the propensity to view oneself as capable of meeting the demands or challenges of tasks within a wide range of contexts (Chen et al., 2001), has been consistently and positively associated with greater psychological resilience among adults during the pandemic, including less severe depressive symptoms and less hazardous alcohol use (e.g., Dogan-Sander et al., 2021; Kohls et al., 2021; Spoorthy et al., 2020; Volken et al., 2021). As evidence across multiple countries shows that people with low general self-efficacy tend to experience self-doubt when they encounter environmental challenges, think in self-debilitating ways, cope less functionally with stressors, and avoid demands that are perceived as threatening (e.g., Luszczynska et al., 2005), it follows that this trait would be a risk factor for “high-risk” depression and alcohol problems.
Additionally, positive links between external stressors and depression and alcohol problems have emerged during the pandemic. For example, research has found that income loss/financial worry, having children under 18 years of age at home, and living alone were related to increased depression, alcohol consumption, and problematic drinking (e.g., binge drinking) at the beginning of the pandemic (e.g., Fancourt et al., 2021; Wardell et al., 2020) and throughout the pandemic (e.g., Acuff et al., 2022; Centre for Addiction and Mental Health, 2020). While these relationships suggest that these external stressors may distinguish “high-risk” from “low-risk” subgroups of depression and alcohol problems, it is alternatively possible that these external stressors are of less importance to comorbidity in comparison to internal factors. Indeed, a longitudinal study of drinking habits among adults over the course of COVID-19 found that a combined increase in alcohol use and related problems was unrelated to the aforementioned external stressors, but was related to pre-pandemic hazardous alcohol use and solitary drinking, as well as possessing a higher alcohol demand prior to COVID-19 (Baptist-Mohseni et al., 2022).
Finally, there is a clear relevance to understanding peoples’ coping strategies during stressful circumstances, as in the case of the pandemic (see Kar et al., 2021), which may mechanistically distinguish high- and low-risk subgroups of depression and alcohol problems. To reduce psychological distress, a range of coping styles can be adopted, such as avoidant coping characterized by cognitive or physical efforts to disengage from stressors, problem-focused coping characterized by doing something to modify the source of the stress or problem-solving, and emotion-focused coping characterized by managing and easing the emotional distress that is linked to the situation (Carver et al., 1989). Several studies examining the relationships of depression and alcohol consumption during the pandemic with these coping patterns suggest that these difficulties are positively associated with avoidant coping (e.g., using substances to cope, self-distraction, behavioural disengagement) and negatively associated with approach-oriented problem-focused coping (e.g., positive reframing, active coping) and emotion-focused coping (e.g., religion, low self-blame, low venting; e.g., Chodkiewicz et al., 2020; Gurvich et al., 2021; Shamblaw et al., 2021). Although these studies examined only the one-to-one cross-sectional relations of avoidant, problem-focused, and emotion-focused coping with depression and alcohol misuse, these patterns suggest that increased avoidant coping over time might distinguish a “high-risk” subgroup of depression and alcohol problems from a “low-risk” subgroup.
Current study
Most prior studies have reported on the overall relations between depressive problems and alcohol problems and posit that individuals with elevated depression have elevated alcohol-related difficulties (Grant et al., 2015). During the pandemic, there has been a limited number of longitudinal findings related to depression and alcohol problems and many studies use cross-sectional designs that fail to examine both depression and alcohol problems as related (but distinct) aspects of psychological adjustment that can both change dynamically over time. Whereas previous studies (Baptist-Mohseni et al., 2022; Leventhal et al., 2022; Tucker et al., 2022) have examined the trajectories of alcohol consumption and alcohol problems over the course of the pandemic, the current four-wave longitudinal study extended upon this work, using data from Baptist-Mohseni et al. (2022) and conducting parallel-process LCGA to characterize the co-trajectories of depression and alcohol problems among Canadians during the first nine months of the COVID-19 outbreak. Based on prior research (i.e., Frohlich et al., 2018; Orui et al., 2020), we expected to find multiple subgroups of depression and alcohol problems, at minimum a high-risk (comorbid) subgroup; a moderate-risk (depression-only) subgroup; and a low-risk (normative) subgroup. Further, informed by previous literature, we expected personality risk factors measured at baseline (namely, anxiety sensitivity, hopelessness, impulsivity, boredom proneness, and low general self-efficacy) to increase the likelihood of combined (i.e., comorbid) depression and alcohol problems over time during the pandemic. Drawing on Baptist-Mohseni et al. (2022), we also examined the relative predictive importance of external stressors (namely, experiencing a loss of income during the pandemic, being a parent who lives with a child under 18 years of age, and living alone). Given the noted sex differences in depression and alcohol difficulties (e.g., Karpyak et al., 2016; Polak et al., 2015; Tucker et al., 2022), we also explored differences between males and females in the co-trajectories of depression and alcohol problems. Finally, based on prior research, we expected that the high-risk depression and alcohol problems subgroup would be distinguished from the other subgroups based on their increasing use of avoidant coping strategies during the pandemic.
Method
Participant and procedures
We received ethics approval from our institutional research ethics board. Data for this study was drawn from larger longitudinal studies that examined addictive behaviours during COVID-19 (see Baptist-Mohseni et al., 2022 and Wardell et al., 2020 for more details). We recruited participants via Prolific (Palan & Schitter, 2018). Adults who live in Canada, report consuming alcohol (i.e., report having more than 1 standard drink in the three months prior to wave 1), and have a high approval rating from prior studies on Prolific completed the current study. Data was collected for wave 1 between April 30th and May 4th of 2020, roughly 2 months after Canada’s COVID-19 State-of-Emergency and strict public health measures (e.g., extensive closures, stay-at-home guidelines) first went into effect. Data was collected for wave 2, wave 3, and wave 4 in July 2020, October 2020, and January 2021, respectively, during which time many public health measures remained in place throughout Canada. Participants were compensated with $13 CAD at each wave.
For information on data exclusion, please see Wardell et al. (2020) and Baptist-Mohseni et al. (2022). The final sample comprised of 364 participants (Mage = 32.16, SDage = 9.54; 54.67% male). Of this sample, 294 participants (80.77%) completed wave two, 263 participants (72.25%) completed wave three, and 246 participants (67.58%) completed wave four. Most participants identified as White (65.66%) and as a non-student (75.82%), with the majority possessing a College or University degree (53.85%). Half of the participants resided in Ontario (51.65%). The median income reported by participants was $80,000–$99,000. Nearly a quarter of the sample (24.79%) endorsed hazardous alcohol consumption at wave one (based on a score of 8 or more on the 10-item Alcohol Use Disorders Identification Test; MAUDIT = 5.95, SDAUDIT = 5.08). Table S1 in the Supplemental Materials presents the full demographic characteristics of the sample.
Measures
See the Supplemental Materials for a full description of the measures administered in the current study, including example items and how each item was rated. Participants’ depression severity was assessed at all four waves using the Patient Health Questionnaire (PHQ-9; Kroenke et al., 2001, α = 0.87–0.90), with the total score corresponding to different levels of severity (i.e., 5–9 = Mild; 10–14 = Moderate; 15–19 = Moderately Severe; 20–27 = Severe). Participants’ alcohol problems was assessed at all four waves using the Short Inventory of Problems-Revised (SIP-2R; Kiluk et al., 2013; α = 0.91–0.95). With respect to personality factors, participants’ anxiety sensitivity, hopelessness, impulsivity, and sensation seeking were assessed at wave 1 using the Substance Use Risk Profile Scale (SURPS; Woicik et al., 2009; α = 0.71–0.89). Participants’ boredom proneness was assessed at wave 1 using the Short Boredom Proneness Scale (SBPS; Struk et al., 2017; α = 0.90). Participants’ general self-efficacy was assessed at wave 1 using the New General Self-Efficacy Scale (NGSES; Chen et al., 2001; α = 0.90). Drawing from Wardell and colleagues (2020) and Baptist-Mohseni and colleagues (2022), we assessed three pandemic-relevant external stressors; specifically, participants indicated if they experienced a loss of income during the pandemic; are a parent who lives with a child under 18; and live alone (each item was rated as “No” = 0 or “Yes” = 1). Finally, participants’ avoidant coping (characterized by facets of self-distraction, denial, substance use, and behavioural disengagement), problem-focused coping (characterized by facets of active coping, using instrumental supports, positive reframing, and planning), and emotion-focused coping (characterized by facets of using emotional supports, venting, humour, acceptance, religion, and self-blame) were assessed at all four waves using the Brief Coping Orientation to Problems Experienced Inventory (Brief-COPE; Carver, 1997; α = 0.71–0.93; see the Supplemental Materials for a description of the three coping facets that were excluded from data analyses due to poor internal reliability).
Data analyses
First, the data was inspected for outliers and to verify other statistical testing assumptions (e.g., normality). Outlying values were Winsorized (i.e., replaced with the highest value within ± 3.29 standard deviations of a given variable’s the mean score). We additionally conducted independent t-tests to examine potential baseline differences between participants with complete data across all four waves (n = 246) and participants with incomplete data across all four waves (n = 118) on the continuous variables at wave one.
Second, parallel-process LCGA was used to identify unique latent (unobserved) classes or subgroups of participants based on their initial levels of depression (PHQ-9) and alcohol problems (SIP-2R) and based on the changes in these difficulties over the first nine months of the pandemic. More specifically, models with one latent class to six latent classes were run and tested consecutively to determine how many classes the data best supports. Three fit indices (Jung and Wickrama, 2007) were used to compare the six models. The sample size-adjusted Bayesian Information Criterion (SA-BIC) is a relative fit index, with lower values suggesting better model fit. As reported by Raftery (1995), a difference of 10 between models in the SA-BIC suggests superior fit. Entropy characterizes a model’s quality for classifying participants into smaller subgroups, with values ≥ 0.80 suggesting that the model’s overall classification quality is good (Ram & Grimm, 2009). To determine whether or not a model with “k” latent subgroups fits the data statistically significantly better than a model with “k – 1” latent subgroups, the parametric bootstrapped likelihood ratio test (BLRT) was used (Nylund et al., 2007). Drawing on Wickrama and colleagues (2016), we additionally examined the class size when selecting the class model, ensuring that the size of the smallest class was not less than 5 percent of the overall sample. Finally, to ensure that the latent classes were unique and theoretically meaningful, we examined all six models visually by graphing the co-trajectories of depression and alcohol problems of each class within each model (Williams & Kibowski, 2016).
Third, multinomial logistic regressions were estimated to explore whether personality and pandemic-relevant external stressors predict participants’ membership in the depression-alcohol problems subgroups. The first model examined anxiety sensitivity, hopelessness, impulsivity, and sensation seeking (following Orui et al., 2020), and the second model examined boredom proneness and general self-efficacy. External stressors (i.e., experiencing a loss of income during the pandemic, being a parent who lives with a child under 18, and living alone) were included in these models in order to understand the relative predictive importance of internal versus external factors on class membership. Biological sex was also included as a predictor.
Finally, linear mixed models (LMMs) were estimated to explore differences between the depression-alcohol problems classes on avoidant coping, problem-focused coping, and emotion-focused coping over time during the pandemic. The class (subgrouping) variable was represented with dummy coded variables, which were used to create the “Class by Time” interaction terms. Age, biological sex, and race (non-White versus White) were included in all LMMs as covariates. Prior to these LMMs, we investigated the intercept and the slope of each coping strategy outcome variable and we observed variability across participants in both parameter estimates for each outcome variable, which suggests that these parameter estimates are not fixed across participants. Thus, we specified random intercepts and random slopes within each LMM. Further, in each LMM, we initially modelled the linear effect of time and the quadratic effect of time, as well as their respective interactions with class. As the quadratic effect of time and the “quadratic time by class” interaction were not supported across all models (all p’s > 0.05), these two terms were removed from all of the LMMs in order to streamline the interpretation of the linear effect of time and for parsimony. Full information maximum likelihood was used to estimate the parallel-process LCGAs and the LMMs.
Results
Descriptive statistics
Table S2 in the Supplemental Materials presents descriptive data for the continuous variables included in the parallel-process LCGA, multinomial logistic regressions, and LMMs. With respect to the pandemic-relevant external stressors, 41.21% of participants reported experiencing a loss of income during the pandemic, 20.39% of participants identified as parents who live with at least one child under 18 during the pandemic, and 12.91% of participants reported lived alone during the pandemic. The independent t-tests indicated no significant baseline differences between participants who had data at all four waves and participants who had missing data at one or more waves on all continuous wave one measures (all p’s > 0.05).
Subgroups for combined depression and alcohol problems
Table 1 presents the results for the models consisting of one latent class to six latent classes, estimated using parallel-process LCGA. Across all models, the SA-BIC index decreased, with a difference greater than 10 between each model (i.e., the model with “k” classes) and the previous model (i.e., the model with “k – 1” classes). Across all models, the entropy values were above 0.80, which suggests that the overall classification quality was good, and the parametric BLRT was significant (all p’s < 0.001). However, the sizes for models with four, five, and six classes were small (< 4 percent of the sample). These models also possessed low classification probabilities (specifically < 0.49), which suggests that the models were not accurately classifying participants into the smaller classes/subgroups. Furthermore, models with four, five, and six classes had classes with similar co-trajectories of depression severity and alcohol problems across the study’s four waves, which suggests that the classes were not meaningfully distinct or unique. Accordingly, upon considering all fit statistics, class sizes, and classification probabilities, as well as graphing the co-trajectories for each class in all of the six models, we determined that the three-class solution, which possessed high classification probabilities (> 0.87), was the most interpretable model.
The first class (6.32% of participants in the sample, n = 23) had moderate initial levels of both depression and alcohol problems that both significantly increased over the course of the COVID-19 pandemic (i.e., from wave one to wave four). The second class (7.69% of participants in the sample, n = 28) had mild-to-moderate initial levels of depression that remained stable over time and moderate initial levels of alcohol problems that significantly decreased over time. The third class (85.99% of participants in the sample, n = 313) had mild initial levels of both depression and alcohol problems, with the latter significantly decreasing over time. In subsequent sections, we refer to these three classes as followed: “moderate increasing depression and alcohol problems” subgroup (Class 1), “moderate stable depression, moderate decreasing alcohol problems” subgroup (Class 2), and “low-risk normative” subgroup (Class 3). Table 2 and Fig. 1 present the parameter estimates and graphs, respectively, of each latent class.

Longitudinal Co-Trajectories of Depression and Alcohol Problems of the Three Latent Classes
Risk factors
Next, multinomial logistic regressions were estimated to determine the preditive roles of personality, pandemic-relevant external stressors, and biological sex on participants’ membership in the depression-alcohol problems subgroups. These results are presented in Tables 3 and 4, which report each predictor’s odds ratio with 95% confidence intervals (CIs). A variable was considered to be a predictor of being in the “high-risk” (versus “low-risk”) depression-alcohol problems subgroup if the 95% CI for the odds ratio did not include 1.0.
In the first model (Table 3), we found that compared to the “low-risk normative” subgroup, the “moderate increasing depression and alcohol problems” subgroup endorsed significantly higher hopelessness and impulsivity, and the “moderate stable depression, moderate decreasing alcohol problems” subgroup endorsed significantly higher impulsivity. The reference subgroup was then changed in order to determine if these personality traits differentiated the “moderate increasing depression and alcohol problems” subgroup from the “moderate stable depression, moderate decreasing alcohol problems” subgroup; we found that these traits did not relate to subgroup membership.
In the second model (Table 4), we found that compared to the “low-risk normative” subgroup, the “moderate increasing depression and alcohol problems” subgroup endorsed significantly higher boredom proneness and significantly lower general self-efficacy, and the “moderate stable depression, moderate decreasing alcohol problems” subgroup endorsed significantly higher boredom proneness. Compared to the “moderate stable depression, moderate decreasing alcohol problems” subgroup, the “moderate increasing depression and alcohol problems” subgroup endorsed significantly lower general self-efficacy.
In both models (Tables 3 and 4), biological sex, experiencing a loss of income during the pandemic, being a parent who lives with a child under 18, and living alone were unrelated to depression-alcohol problems subgroup membership.
Coping strategies
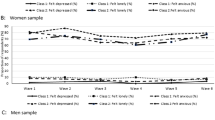
Finally, linear mixed models (LMMs) were conducted to explore differences between the depression-alcohol problems subgroups in avoidant, problem-focused, and emotion-focused coping over time during the pandemic. Time was coded as 0, 1, 2, and 3. Age, sex, and race were statistically controlled for. Table 5 and Fig. 2 present the parameter estimates and graphs, respectively, of the Class by Time effects. Using Rights and Sterba’s (2019) Integrative Framework of R-Squared Measures, we report the proportion of total dependent variable variance explained by the LMM (i.e., by predictors through fixed slopes and random slope variation-covariation and by group outcome means through variations in the random intercept).

Coping Strategies of the Three Latent Classes
With respect to avoidant coping, there was a supported Class (Class 1 versus Class 3) by Time interaction in predicting the use of denial (Table 5, Model 1). Simple slopes analysis indicated that the “moderate increasing depression and alcohol problems” subgroup’s use of denial significantly increased over time (BClass1 = 0.21, SEClass1 = 0.10, pClass1 = 0.032, 95% CIClass1 [0.0184, 0.4005]), whereas denial did not significantly change over time among the “moderate stable depression, moderate decreasing alcohol problems” subgroup (BClass2 = 0.06, SEClass2 = 0.08, pClass2 = 0.436, 95% CIClass2 [-0.0953, 0.2198]) and the “low-risk normative” subgroup (BClass3 = -0.04, SEClass3 = 0.03, pClass3 = 0.149, 95% CIClass3 [-0.0857, 0.0129]). Similarly, there was a supported Class (Class 1 versus Class 2; Class 1 versus Class 3) by Time interaction in predicting the use of substances to cope (Table 5, Model 2). Simple slopes analysis found that the use of drugs and alcohol to cope significantly increased over time among the “moderate increasing depression and alcohol problems” subgroup (BClass1 = 0.45, SEClass1 = 0.12, pClass1 < 0.001, 95% CIClass1 [0.2185, 0.6732]), but significantly decreased over time among the “moderate stable depression, moderate decreasing alcohol problems” subgroup (BClass2 = -0.25, SEClass2 = 0.09, pClass2 = 0.008, 95% CIClass2 [-0.4395, -0.0672]). Among the “low-risk normative” subgroup, the use of substances to cope did not significantly change (BClass3 = -0.03, SEClass3 = 0.03, pClass3 = 0.273, 95% CIClass3 [-0.0910, 0.0257]). Finally, there was a supported Class (Class 1 versus Class 3) by Time interaction in predicting behavioural disengagement (Table 5, Model 3). Simple slopes analysis indicated that behavioural disengagement (i.e., giving up on attempts to cope) significantly increased over time among the “moderate increasing depression and alcohol problems” subgroup (BClass1 = 0.43, SEClass1 = 0.12, pClass1 < 0.001, 95% CIClass1 [0.1971, 0.6616]), but did not significantly change over time among the “moderate stable depression, moderate decreasing alcohol problems” subgroup (BClass2 = 0.20, SEClass2 = 0.10, pClass2 = 0.059, 95% CIClass2 [-0.0103, 0.3934]) and the “low-risk normative” subgroup (BClass3 = 0.01, SEClass3 = 0.03, pClass3 = 0.729, 95% CIClass3 [-0.0495, 0.0705]). The LMMs explained 53.9%, 66.1%, and 51.7% of the total outcome variance in the use of denial, drugs and alcohol, and behavioural disengagement, respectively.
With regards to problem-focused coping, there was a supported Class (Class 1 versus Class 2; Class 2 versus Class 3) by Time interaction in predicting planning (Table 5, Model 4). Simple slopes analysis found that the “moderate stable depression, moderate decreasing alcohol problems” subgroup’s use of planning significantly increased over time (BClass2 = 0.28, SEClass2 = 0.12, pClass2 = 0.021, 95% CIClass2 [0.0569, 0.5332]), but that the use of planning did not significantly change over time among the “moderate increasing depression and alcohol problems” subgroup (BClass1 = -0.16, SEClass1 = 0.15, pClass1 = 0.298, 95% CIClass1 [-0.4846, 0.1307]) and the “low-risk normative” subgroup (BClass3 = -0.05, SEClass3 = 0.04, pClass3 = 0.210, 95% CIClass3 [-0.1259, 0.0261]). The LMM explained 52.0% of the total outcome variance in the use of planning.
Finally, with respect to emotion-focused coping, the LMM supported a Class (Class 2 versus Class 3) by Time interaction in predicting the use of emotional supports (Table 5, Model 5). Simple slopes analysis indicated that the “moderate stable depression, moderate decreasing alcohol problems” subgroup’s use of emotional supports significantly increased over time (BClass2 = 0.25, SEClass2 = 0.11, pClass2 = 0.026, 95% CIClass2 [0.0305, 0.4685]), whereas this coping strategy did not significantly change over time among the “moderate increasing depression and alcohol problems” subgroup (BClass1 = 0.14, SEClass1 = 0.13, pClass1 = 0.304, 95% CIClass1 [-0.1258, 0.4033]) and the “low-risk normative” subgroup (BClass3 = -0.04, SEClass3 = 0.03, pClass3 = 0.227, 95% CIClass3 [-0.1111, 0.0264]). The LMM explained 66.0% of the total outcome variance in the use of emotional supports. The Class by Time interactions for predicting the other problem-focused and emotion-focused strategies were non-significant (see Table S3 in the Supplemental Materials).
Discussion
The current study analyzed longitudinal data, using parallel-process LCGA to determine whether distinct and meaningful classes of individuals would emerge based on their co-trajectories of depression and alcohol problems during the COVID-19 pandemic. Equally importantly, the current study sought out to determine the risk factors for combined increases in depression and alcohol problems among some people. To our knowledge, no prior study has examined person-centered changes in both depression and alcohol problems over a long period of time during the COVID-19 pandemic. Consistent with the above-reviewed studies, we found multiple classes of individuals based on their co-trajectories of depression and alcohol problems during the first nine months of the COVID-19 outbreak: a “low-risk normative” subgroup, a “moderate stable depression, moderate decreasing alcohol problems” subgroup, and a “moderate increasing depression and alcohol problems” subgroup. These patterns underscore the heterogeneity in the co-trajectory of depression and alcohol problems during the pandemic, highlighting that depression and alcohol problems remained stable and improved over time for some people, but both significantly worsened over time for other people. The multinomial logistic regressions and LMMs elucidate the risk factors for increasing depression and alcohol problems, which has significant clinical implications.
The “moderate increasing depression and alcohol problems” subgroup endorsed higher hopelessness and impulsivity than the “low-risk normative” subgroup. These results suggests depression characteristics (i.e., hopelessness) do not solely contribute to increasing depression and alcohol problems over time, and that impulsivity also plays a unique role, which is consistent with prior work linking impulsivity to both mood- (e.g., Adams et al., 2019; Keough et al., 2016) and alcohol-related difficulties (e.g., Adams et al., 2019; Gonzalez et al., 2011). Further, the “moderate stable depression, moderate decreasing alcohol problems” subgroup also endorsed higher impulsivity than the “low-risk” subgroup, however this result may be accounted for the fact that people in this subgroup had moderate initial levels of alcohol problems (before these problems decreased over time). Overall, these results emphasize the need to further explore the way in which impulsivity exacerbates or maintains peoples’ mood- and alcohol-related difficulties.
The “moderate increasing depression and alcohol problems” subgroup also endorsed higher levels of boredom proneness and lower levels of general self-efficacy than the “low-risk normative” subgroup. Tying together boredom proneness and general self-efficacy is the tendency to focus on oneself, which, according to theories of objective self-awareness (Brockmeyer et al., 2015; Duval & Wicklund, 1972; Higgins, 1987; Steenbarger & Aderman, 1979), is associated with negative mood states (e.g., disappointment, dejection) and attempts to escape/avoid self-awareness. A person high in boredom proneness is persistently self-focused—aware of their lack of cognitive engagement but unable to articulate actionable desires and meaningfully engage with their external environment (Eastwood & Bambrah, 2021). Indeed, correlational studies suggest a positive relationship between trait indices of self-directed attention and boredom proneness (Eastwood et al., 2007; Gana et al., 2000; Harris, 2000; Seib & Vodanovich, 1998; von Gemmingen et al., 2003; as cited in Eastwood & Bambrah, 2021). Similarly, a person with low general self-efficacy is often focused on the discrepancy between what they would like to achieve and what they believe they are capable of achieving across contexts; and hence, they often avoid external circumstances/tasks perceived as difficult and they lack the ability to regulate their emotional states in such circumstances/tasks (Bandura, 1999, 2010; Carr, 2004). The current study’s results suggest that, compared to the “normative” subgroup, people with combined increases in depression and alcohol problems might be more self-focused—stuck on themselves, unable to transition into engaging, meaningful, and self-regulatory behaviour(s). Future studies could explicitly test whether or not the relationships of boredom proneness and general self-efficacy with combined increases in depression and alcohol problems involve self-directed attention.
Speaking to the findings from the LMMs, the “moderate increasing depression and alcohol problems” subgroup increasingly used avoidant coping over time, specifically the tendency to deny the reality of their problems, to use alcohol or other drugs to make themselves feel better and get through challenges, and to give up on attempts to cope with or address stressors. In tandem with the multinomial logistic regressions, which found that low general self-efficacy uniquely distinguished the “moderate increasing depression and alcohol problems” subgroup from both of the other subgroups, these findings suggests that people with combined increases in depression and alcohol problems not only tend to possess little belief in their ability to manage difficult and stressful circumstances, but also coped with such circumstances during the pandemic in a manner where they avoided thinking about, feeling, and doing difficult things. Importantly, given the pandemic’s enduring nature, these findings are the first to suggest that worsening depression and alcohol problems among a subset of people was associated longitudinally with unhealthy cognitive (denial) and behavioural (substance use, behavioural disengagement) coping efforts to avoid stressors. In contrast, the “moderate stable depression, moderate decreasing alcohol problems” subgroup decreasingly used avoidant coping, specifically substances to cope. They also increasingly used adaptive problem-focused coping skills and emotion-focused coping skills over time, specifically the tendency to plan and strategize the steps to deal with stressors and to seek comfort and emotional support from others. Avoidant coping strategies are associated with a host of psychological difficulties, including depression and problematic alcohol use, whereas problem- and emotion-focused strategies that are characterized by approaching and addressing challenging circumstances and concomitant negative emotions are associated with indices of psychological well-being (e.g., Dias et al., 2012; Eisenberg et al., 2012; Poulus et al., 2020).
Notably, increases in depression and alcohol problems were more strongly related to internal factors (hopelessness, impulsivity, boredom proneness, general self-efficacy, and avoidant coping) than external stressors (experiencing a loss of income during the pandemic, being a parent who lives with a child under 18, living alone), which is consistent with the above-reviewed longitudinal findings by Baptist-Mohseni et al. (2022). Elucidating the personality and coping risk factors associated with combined increases in depression and alcohol problems not only underscores who may benefit most from prevention and intervention approaches during the pandemic (and other such stressful circumstances), but also areas of focus for these approaches. Indeed, psychoeducation and treatment approaches that target those prone to hopelessness, boredom, and low self-efficacy and that focus on reducing the use avoidant coping and enhancing the use of approach-oriented coping may help facilitate recovery and preparedness for those at risk for worsening depression alcohol problems. Specifically, approaches that emphasize the impeding nature of denial, substance use, and behavioural disengagement on one’s ability to cope with stressors in the long-term (e.g., that denying the reality of a stressor, using alcohol/drugs, and reducing one’s efforts to address a stressor might permit the stressor to become more serious, making it more difficult to address; Carver et al., 1989), as well as emphasize how these avoidant coping strategies maintain hopelessness, the aversive feeling of being cognitively unengaged with one’s surroundings, and the low belief in one’s ability to achieve goals despite difficult circumstances, may be helpful in this regard. Cognitive behavioural therapy, which seeks to mitigate peoples’ avoidance, escape, and other safety behaviours, as well as increase behavioural activation and engagement in meaningful and valued activities, may be an important avenue for intervention, as it has shown to be effective for people struggling with depression symptoms and problematic drinking (e.g., Pedrelli et al., 2013; Riper et al., 2014).
The use of a longitudinal design with four waves of assessment and with a large sample from across Canada, as well as the use of attention checks and validated measures to ensure accurate data on functioning, are key strengths of the current study. However, there are some shortcomings, including the lack of racial, provincial/territorial, and financial representation in our sample as the majority of participants identified as Caucasian, predominantly resided in Ontario, British Columbia, and Alberta, and had a high socioeconomic status. Additionally, we are precluded from extrapolating the current study’s findings and the implications for treating pandemic-related depression and alcohol problems to individuals with severe psychopathology as we did not examine (and control for) pre-existing mental health diagnoses in our community sample. Moreover, there was 32.42% overall attrition across waves and this could have reduced statistical power in the analyses that involved our smaller classes, such as the multinomial logistic regressions. Relatedly, our sample size could be viewed as modest for latent class growth analyses. Larger sample sizes would permit the use of other analytical approaches (see Kamata et al., 2018 for a review of the one- and three-step approaches) that are less likely to yield biased estimates of the relationships of the latent classes with auxiliary variables (i.e., covariates, outcomes) because they retain the classification measurement errors across models. Future studies on pandemic-related depression and alcohol problems that reproduce our results in more diverse and larger groups of participants, as well as that have lower attrition rates, will be important.
In spite of these shortcomings, we obtained high classification probabilities in the current study, which, in tandem with prior findings (Frohlich et al., 2018; Orui et al., 2020), reinforces the distinct and meaningful classes of depression and alcohol problems that emerged in the data, as well as the risk factors for people with combined increases in depression and alcohol problems. As noted above, future studies should endeavour to understand exactly how features of personality (e.g., self-directed attention in boredom proneness and general self-efficacy) contribute to increased depression and alcohol problems, so that interventions can be tailored more incisively. Furthermore, longitudinal studies that assess peoples’ depression and alcohol problems beyond the waves that were examined in the current study will be critical in order to continue to understand the persisting and lingering effects of the pandemic on individuals’ psychological functioning.
Data availability
Subject to the ethical requirements of the York University Human Participants Research Committee and the Canadian Tri-Council policy statement on ethical conduct for research involving humans, all data, analysis code, and research materials underlying this study will be made available to researchers upon submission of an approved ethics protocol from their academic or research institution (or equivalent) to the corresponding author.
References
Acuff, S. F., Strickland, J. C., Tucker, J. A., & Murphy, J. G. (2022). Changes in alcohol use during COVID-19 and associations with contextual and individual difference variables: A systematic review and meta-analysis. Psychology of Addictive Behaviors, 36(1), 1–19. https://doi.org/10.1037/adb0000796
Adams, T., Rapinda, K. K., Frohlich, J. R., O’Connor, R. M., & Keough, M. T. (2019). Impulsivity moderates the effect of social anxiety on in-lab alcohol craving. Addictive Behaviors, 97, 70–76. https://doi.org/10.1016/j.addbeh.2019.05.025
Bambrah, V., Gurovich, S., Friedman, E., & Eastwood, J. D. (2020). What does trait boredom mean? Is it about how you feel or how you respond to boring situations? Paper presented at the 81st annual convention of the Canadian Psychological Association, Montreal.
Bandura, A. (1999). Self-efficacy: The exercise of Control. Freeman.
Bandura, A. (2010). Self-Efficacy. In The Corsini Encyclopedia of Psychology (4th ed., pp. 1–3). John Wiley & Sons, Inc.
Baptist-Mohseni, N., Morris, V., Vedelago, L., Kempe, T., Rapinda, K., Mesmer, E., Bilevicius, E., Wardell, J. D., MacKillop, J., & Keough, M. T. (2022). A longitudinal approach to understanding risk factors for problem alcohol use during the Covid-19 pandemic. Alcoholism: Clinical and Experimental Research, 46(3), 434–446. https://doi.org/10.1111/acer.14774
Barari, S., Caria, S., Davola, A., Falco, P., Fetzer, T., Fiorin, S., Hensel, L., Ivchenko, A., Jachimowicz, J., King, G., Kraft-Todd, G., Ledda, A., MacLennan, M., Mutoi, L., Pagani, C., Reutskaja, E., Roth, C., & Slepoi, F. R. (2020). Evaluating covid-19 public health messaging in Italy: Self-reported compliance and growing mental health concerns. https://doi.org/10.1101/2020.03.27.20042820
Bench, S. W., & Lench, H. C. (2019). Boredom as a seeking state: Boredom prompts the pursuit of novel (even negative) experiences. Emotion, 19(2), 242–254. https://doi.org/10.1037/emo0000433
Brockmeyer, T., Zimmermann, J., Kulessa, D., Hautzinger, M., Bents, H., Friederich, H.-C., Herzog, W., & Backenstrass, M. (2015). Me, myself, and I: Self-referent word use as an indicator of self-focused attention in relation to depression and anxiety. Frontiers in Psychology, 6. https://doi.org/10.3389/fpsyg.2015.01564
Canadian Centre on Substance Use and Addiction (2020). Canadians under 54 drinking more while at home due to COVID-19 pandemic [Web site]. April 15, 2020. Available at: https://ccsa.ca/canadians-under-54-drinking-more-while-home-due-covid-19-pandemic. Accessed 5 June 2020.
Capasso, A., Jones, A. M., Ali, S. H., Foreman, J., Tozan, Y., & DiClemente, R. J. (2021). Increased alcohol use during the COVID-19 pandemic: The effect of mental health and age in a cross-sectional sample of social media users in the U.S. Preventive Medicine, 145, 106422. https://doi.org/10.1016/j.ypmed.2021.106422
Carr, A. (2004). Positive psychology: The science of happiness and human strengths. Routledge.
Carver, C. S. (1997). You want to measure coping but your protocol is too long: Consider the Brief-COPE. International Journal of Behavioral Medicine, 4(1), 92–100. https://doi.org/10.1207/s15327558ijbm0401_6
Carver, C. S., Scheier, M. F., & Weintraub, J. K. (1989). Assessing coping strategies: A theoretically based approach. Journal of Personality and Social Psychology, 56(2), 267–283. https://doi.org/10.1037/0022-3514.56.2.267
Castillo-Carniglia, A., Keyes, K. M., Hasin, D. S., & Cerdá, M. (2019). Psychiatric comorbidities in alcohol use disorder. The Lancet Psychiatry, 6(12), 1068–1080. https://doi.org/10.1016/s2215-0366(19)30222-6
Cataudella, S., Carta, S. M., Mascia, M. L., Masala, C., Petretto, D. R., Agus, M., & Penna, M. P. (2021). Teaching in times of the COVID-19 pandemic: A pilot study on teachers’ self-esteem and self-efficacy in an Italian sample. International Journal of Environmental Research and Public Health, 18(15), 8211. https://doi.org/10.3390/ijerph18158211
Centre for Addiction and Mental Health (2020). COVID-19 national survey dashboard [Web site]. 2020. Available at: https://www.camh.ca/en/health-info/mental-health-and-covid-19/covid-19-national-survey. Accessed 8 June 2020.
Chao, M., Chen, X., Liu, T., Yang, H., & Hall, B. J. (2020). Psychological distress and state boredom during the COVID-19 outbreak in China: The role of meaning in life and media use. European Journal of Psychotraumatology, 11(1), 1769379. https://doi.org/10.1080/20008198.2020.1769379
Chen, G., Gully, S. M., & Eden, D. (2001). Validation of a new general self-efficacy scale. Organizational Research Methods, 4(1), 62–83. https://doi.org/10.1177/109442810141004
Chodkiewicz, J., Talarowska, M., Miniszewska, J., Nawrocka, N., & Bilinski, P. (2020). Alcohol consumption reported during the covid-19 pandemic: The initial stage. International Journal of Environmental Research and Public Health, 17(13), 4677. https://doi.org/10.3390/ijerph17134677
Danckert, J., Mugon, J., Struk, A., & Eastwood, J. D. (2018). Boredom: What is it good for? In H. A. Lench (Ed.), The function of emotions: When and why emotions help us (pp. 93–121). Springer International Publishing.
Dias, C., Cruz, J. F., & Fonseca, A. M. (2012). The relationship between multidimensional competitive anxiety, cognitive threat appraisal, and coping strategies: A multi-sport study. International Journal of Sport and Exercise Psychology, 10(1), 52–65. https://doi.org/10.1080/1612197x.2012.645131
Dogan-Sander, E., Kohls, E., Baldofski, S., & Rummel-Kluge, C. (2021). More depressive symptoms, alcohol and drug consumption: Increase in mental health symptoms among university students after one year of the COVID-19 pandemic. Frontiers in Psychiatry, 12. https://doi.org/10.3389/fpsyt.2021.790974
Dozois, D. J. (2021). Anxiety and depression in Canada during the COVID-19 pandemic: A national survey. Canadian Psychology/psychologie Canadienne, 62(1), 136–142. https://doi.org/10.1037/cap0000251
Droit-Volet, S., Gil, S., Martinelli, N., Andant, N., Clinchamps, M., Parreira, L., Rouffiac, K., Dambrun, M., Huguet, P., Dubuis, B., Pereira, B., Bouillon, J.-B., & Dutheil, F. (2020). Time and covid-19 stress in the lockdown situation: Time free, dying of boredom and sadness. PLOS ONE, 15(8). https://doi.org/10.1371/journal.pone.0236465
Duval, S., & Wicklund, R. A. (1972). A theory of objective self-awareness. Academic Press.
Eastwood, J. D., & Bambrah, V. (2021). Self-focused but lacking self-insight: The relationship between boredom and self-consciousness. Paper presented at the 4th International Interdisciplinary Boredom Conference, Madrid.
Eastwood, J. D., Cavaliere, C., Fahlman, S. A., & Eastwood, A. E. (2007). A desire for desires: Boredom and its relation to alexithymia. Personality and Individual Differences, 42(6), 1035–1045. https://doi.org/10.1016/j.paid.2006.08.027
Eisenberg, S. A., Shen, B.-J., Schwarz, E. R., & Mallon, S. (2012). Avoidant coping moderates the association between anxiety and patient-rated physical functioning in heart failure patients. Journal of Behavioral Medicine, 35(3), 253–261. https://doi.org/10.1007/s10865-011-9358-0
Fahlman, S. A., Mercer-Lynn, K. B., Flora, D. B., & Eastwood, J. D. (2013). Development and validation of the Multidimensional State Boredom scale. Assessment, 20(1), 68–85. https://doi.org/10.1177/1073191111421303
Fancourt, D., Steptoe, A., & Bu, F. (2021). Trajectories of anxiety and depressive symptoms during enforced isolation due to covid-19 in England: A longitudinal observational study. The Lancet Psychiatry, 8(2), 141–149. https://doi.org/10.1016/s2215-0366(20)30482-x
Frohlich, J. R., Rapinda, K. K., O’Connor, R. M., & Keough, M. T. (2018). Examining co-patterns of depression and alcohol misuse in emerging adults following university graduation. Addictive Behaviors Reports, 8, 40–45. https://doi.org/10.1016/j.abrep.2018.06.002
Gana, K., Deletang, B., & Metais, L. (2000). Is boredom proneness associated with introspectiveness? Social Behavior and Personality: An International Journal, 28(5), 499–504. https://doi.org/10.2224/sbp.2000.28.5.499
Gonzalez, V. M., Reynolds, B., & Skewes, M. C. (2011). Role of impulsivity in the relationship between depression and alcohol problems among emerging adult college drinkers. Experimental and Clinical Psychopharmacology, 19(4), 303–313. https://doi.org/10.1037/a0022720
Grant, B. F., Goldstein, R. B., Saha, T. D., Chou, S. P., Jung, J., Zhang, H., Pickering, R. P., Ruan, W. J., Smith, S. M., Huang, B., & Hasin, D. S. (2015). Epidemiology of DSM-5 alcohol use disorder: Results from the national epidemiologic survey on alcohol and related conditions. JAMA Psychiatry, 72(8), 757. https://doi.org/10.1001/jamapsychiatry.2015.0584
Gurvich, C., Thomas, N., Thomas, E. H. X., Hudaib, A.-R., Sood, L., Fabiatos, K., Sutton, K., Isaacs, A., Arunogiri, S., Sharp, G., & Kulkarni, J. (2021). Coping styles and mental health in response to societal changes during the COVID-19 pandemic. International Journal of Social Psychiatry, 67(5), 540–549. https://doi.org/10.1177/0020764020961790
Harris, M. B. (2000). Correlates and characteristics of boredom proneness and boredom. Journal of Applied Social Psychology, 30(3), 576–598. https://doi.org/10.1111/j.1559-1816.2000.tb02497.x
Havermans, R. C., Vancleef, L., Kalamatianos, A., & Nederkoorn, C. (2015). Eating and inflicting pain out of boredom. Appetite, 85, 52–57. https://doi.org/10.1016/j.appet.2014.11.007
Higgins, E. T. (1987). Self-discrepancy: A theory relating self and affect. Psychological Review, 94(3), 319–340. https://doi.org/10.1037/0033-295x.94.3.319
Jung, T., & Wickrama, K. A. (2007). An introduction to latent class growth analysis and growth mixture modeling. Social and Personality Psychology Compass, 2(1), 302–317. https://doi.org/10.1111/j.1751-9004.2007.00054.x
Kamata, A., Kara, Y., Patarapichayatham, C., & Lan, P. (2018). Evaluation of analysis approaches for latent class analysis with auxiliary linear growth model. Frontiers in Psychology, 9. https://doi.org/10.3389/fpsyg.2018.00130
Kar, N., Kar, B., & Kar, S. (2021). Stress and coping during COVID-19 pandemic: Result of an online survey. Psychiatry Research, 295, 113598. https://doi.org/10.1016/j.psychres.2020.113598
Karpyak, V. M., Biernacka, J. M., Geske, J. R., Abulseoud, O. A., Brunner, M. D., Chauhan, M., Hall-Flavin, D. K., Lewis, K. A., Loukianova, L. L., Melnyk, G. J., Onsrud, D. A., Proctor, B. D., Schneekloth, T. D., Skime, M. K., Wittkopp, J. E., Frye, M. A., & Mrazek, D. A. (2016). Gender-specific effects of comorbid depression and anxiety on the propensity to drink in negative emotional states. Addiction, 111(8), 1366–1375. https://doi.org/10.1111/add.13386
Keough, M. T., Badawi, G., Nitka, D., O’Connor, R. M., & Stewart, S. H. (2016). Impulsivity increases risk for coping-motivated drinking in undergraduates with elevated social anxiety. Personality and Individual Differences, 88, 45–50. https://doi.org/10.1016/j.paid.2015.08.036
Khantzian, E. J. (1997). The self-medication hypothesis of substance use disorders: A reconsideration and recent applications. Harvard Review of Psychiatry, 4(5), 231–244. https://doi.org/10.3109/10673229709030550
Khantzian, E. J. (2012). Reflections on treating addictive disorders: A psychodynamic perspective. The American Journal on Addictions, 21(3), 274–279. https://doi.org/10.1111/j.1521-0391.2012.00234.x
Kiluk, B. D., Dreifuss, J. A., Weiss, R. D., Morgenstern, J., & Carroll, K. M. (2013). The short inventory of problems – revised (SIP-R): Psychometric Properties within a large, diverse sample of substance use disorder treatment seekers. Psychology of Addictive Behaviors, 27(1), 307–314. https://doi.org/10.1037/a0028445
Kohls, E., Baldofski, S., Moeller, R., Klemm, S.-L., & Rummel-Kluge, C. (2021). Mental health, social and emotional well-being, and perceived burdens of university students during COVID-19 pandemic lockdown in Germany. Frontiers in Psychiatry, 12. https://doi.org/10.3389/fpsyt.2021.643957
Kroenke, K., Spitzer, R. L., & Williams, J. B. (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613. https://doi.org/10.1046/j.1525-1497.2001.016009606.x
Leventhal, A. M., Cho, J., Ray, L. A., Liccardo Pacula, R., Lee, B. P., Terrault, N., Pedersen, E., Lee, J. O., Davis, J. P., Jin, H., Huh, J., Wilson, J. P., & Whaley, R. C. (2022). Alcohol use trajectories among U.S. adults during the first 42 weeks of the Covid‐19 pandemic. Alcoholism: Clinical and Experimental Research. https://doi.org/10.1111/acer.14824
Luszczynska, A., Gutiérrez-Doña, B., & Schwarzer, R. (2005). General self-efficacy in various domains of human functioning: Evidence from five countries. International Journal of Psychology, 40(2), 80–89. https://doi.org/10.1080/00207590444000041
Marani, M., Katul, G. G., Pan, W. K., & Parolari, A. J. (2021). Intensity and frequency of extreme novel epidemics. Proceedings of the National Academy of Sciences, 118(35). https://doi.org/10.1073/pnas.2105482118
McCurdy, A., Stearns, J. A., Rhodes, R. E., Hopkins, D., Mummery, K., & Spence, J. C. (2022). Relationships between physical activity, boredom proneness, and subjective well-being among U.K. adults during the covid-19 pandemic. Journal of Sport & Exercise Psychology, 1–9. https://doi.org/10.1123/jsep.2021-0253
McPhee, M. D., Keough, M. T., Rundle, S., Heath, L. M., Wardell, J. D., & Hendershot, C. S. (2020). Depression, environmental reward, coping motives and alcohol consumption during the covid-19 pandemic. Frontiers in Psychiatry, 11. https://doi.org/10.3389/fpsyt.2020.574676
Muthen, B., & Muthen, L. K. (2000). Integrating person-centered and variable-centered analyses: Growth mixture modeling with latent trajectory classes. Alcoholism: Clinical and Experimental Research, 24(6), 882–891. https://doi.org/10.1111/j.1530-0277.2000.tb02070.x
Nylund, K. L., Asparouhov, T., & Muthén, B. O. (2007). Deciding on the number of classes in latent class analysis and growth mixture modeling: A Monte Carlo simulation study. Structural Equation Modeling: A Multidisciplinary Journal, 14(4), 535–569. https://doi.org/10.1080/10705510701575396
Orui, K., Frohlich, J. R., Stewart, S. H., Sherry, S. B., & Keough, M. T. (2020). Examining subgroups of depression and alcohol misuse in emerging adults during university: A replication and extension study. International Journal of Mental Health and Addiction, 19(6), 2323–2341. https://doi.org/10.1007/s11469-020-00325-w
Palan, S., & Schitter, C. (2018). Prolific.ac—a subject pool for online experiments. Journal of Behavioral and Experimental Finance, 17, 22–27. https://doi.org/10.1016/j.jbef.2017.12.004
Pedrelli, P., Borsari, B., Palm, K. M., Dalton, E., & Fava, M. (2013). Combined MI + CBT for depressive symptoms and binge drinking among young adults: Two case studies. Journal of Cognitive Psychotherapy, 27(3), 235–257. https://doi.org/10.1891/0889-8391.27.3.235
Pedrelli, P., Shapero, B., Archibald, A., & Dale, C. (2016). Alcohol use and depression during adolescence and young adulthood: A summary and interpretation of mixed findings. Current Addiction Reports, 3(1), 91–97. https://doi.org/10.1007/s40429-016-0084-0
Polak, K., Haug, N. A., Drachenberg, H. E., & Svikis, D. S. (2015). Gender considerations in addiction: Implications for treatment. Current Treatment Options in Psychiatry, 2(3), 326–338. https://doi.org/10.1007/s40501-015-0054-5
Pollard, M. S., Tucker, J. S., & Green, H. D. (2020). Changes in adult alcohol use and consequences during the COVID-19 pandemic in the US. JAMA Network Open, 3(9). https://doi.org/10.1001/jamanetworkopen.2020.22942
Poulus, D., Coulter, T. J., Trotter, M. G., & Polman, R. (2020). Stress and coping in esports and the influence of mental toughness. Frontiers in Psychology, 11. https://doi.org/10.3389/fpsyg.2020.00628
Pressley, T., & Ha, C. (2021). Teaching during a pandemic: United States Teachers’ self-efficacy during COVID-19. Teaching and Teacher Education, 106, 103465. https://doi.org/10.1016/j.tate.2021.103465
Raftery, A. E. (1995). Bayesian model selection in Social Research. Sociological Methodology, 25, 111. https://doi.org/10.2307/271063
Ram, N., & Grimm, K. J. (2009). Methods and measures: Growth mixture modeling: A method for identifying differences in longitudinal change among unobserved groups. International Journal of Behavioral Development, 33(6), 565–576. https://doi.org/10.1177/0165025409343765
Reynolds, D. L., Garay, J. R., Deamond, S. L., Moran, M. K., Gold, W., & Styra, R. (2008). Understanding, compliance and psychological impact of the SARS quarantine experience. Epidemiology and Infection, 136(7), 997–1007. https://doi.org/10.1017/s0950268807009156
Rights, J. D., & Sterba, S. K. (2019). Quantifying explained variance in multilevel models: An integrative framework for defining R-squared measures. Psychological Methods, 24, 309–338. https://doi.org/10.1037/met0000184
Riper, H., Andersson, G., Hunter, S. B., Wit, J., Berking, M., & Cuijpers, P. (2014). Treatment of comorbid alcohol use disorders and depression with cognitive-behavioural therapy and Motivational interviewing: A meta-analysis. Addiction, 109(3), 394–406. https://doi.org/10.1111/add.12441
Schmits, E., & Glowacz, F. (2022). Changes in alcohol use during the covid-19 pandemic: Impact of the lockdown conditions and mental health factors. International Journal of Mental Health and Addiction, 20(2), 1147–1158. https://doi.org/10.1007/s11469-020-00432-8
Seib, H. M., & Vodanovich, S. J. (1998). Cognitive correlates of boredom proneness: The role of private selfconsciousness and absorption. The Journal of Psychology, 132(6), 642–652. https://doi.org/10.1080/00223989809599295
Shamblaw, A. L., Rumas, R. L., & Best, M. W. (2021). Coping during the COVID-19 pandemic: Relations with Mental Health and quality of life. Canadian Psychology/psychologie Canadienne, 62(1), 92–100. https://doi.org/10.1037/cap0000263
Shield, K. D., Chrystoja, B. R., Ali, S., Sohi, I., Rehm, J., Nigatu, Y. T., Elton-Marshall, T., Hamilton, H., Jankowicz, D., & Wells, S. (2022). Changes in alcohol consumption in Canada during the COVID-19 pandemic: Associations with anxiety and self-perception of depression and loneliness. Alcohol and Alcoholism, 57(2), 190–197. https://doi.org/10.1093/alcalc/agab055
Simonetti, V., Durante, A., Ambrosca, R., Arcadi, P., Graziano, G., Pucciarelli, G., Simeone, S., Vellone, E., Alvaro, R., & Cicolini, G. (2021). Anxiety, sleep disorders and self-efficacy among nurses during COVID-19 pandemic: A Large Cross-Sectional Study. Journal of Clinical Nursing, 30(9–10), 1360–1371. https://doi.org/10.1111/jocn.15685
Spoorthy, M. S., Pratapa, S. K., & Mahant, S. (2020). Mental health problems faced by healthcare workers due to the COVID-19 pandemic–A Review. Asian Journal of Psychiatry, 51, 102119. https://doi.org/10.1016/j.ajp.2020.102119
Steenbarger, B. N., & Aderman, D. (1979). Objective self-awareness as a nonaversive state: Effect of anticipating discrepancy reduction. Journal of Personality, 47(2), 330–339. https://doi.org/10.1111/j.1467-6494.1979.tb00206.x
Struk, A. A., Carriere, J. S., Cheyne, J. A., & Danckert, J. (2017). A short boredom proneness scale: Development and psychometric properties. Assessment, 24(3), 346–359. https://doi.org/10.1177/1073191115609996
Sun, Y., Song, H., Liu, H., Mao, F., Sun, X., & Cao, F. (2020). Occupational stress, mental health, and self-efficacy among community mental health workers: A cross-sectional study during COVID-19 pandemic. International Journal of Social Psychiatry, 67(6), 737–746. https://doi.org/10.1177/0020764020972131
Tucker, J. S., Rodriguez, A., Green, H. D., & Pollard, M. S. (2022). Trajectories of alcohol use and problems during the COVID-19 pandemic: The role of social stressors and drinking motives for men and women. Drug and Alcohol Dependence, 232, 109285. https://doi.org/10.1016/j.drugalcdep.2022.109285
Volken, T., Zysset, A., Amendola, S., Klein Swormink, A., Huber, M., von Wyl, A., & Dratva, J. (2021). Depressive symptoms in Swiss university students during the COVID-19 pandemic and their correlates. International Journal of Environmental Research and Public Health, 18(4), 1458. https://doi.org/10.3390/ijerph18041458
von Gemmingen, M. J., Sullivan, B. F., & Pomerantz, A. M. (2003). Investigating the relationships between boredom proneness, paranoia, and self-consciousness. Personality and Individual Differences, 34(6), 907–919. https://doi.org/10.1016/s0191-8869(01)00219-7
Wardell, J., Kempe, T., Rapinda, K. K., Single, A. N., Bilevicius, E., Frohlich, J. R., Hendershot, C. S., & Keough, M. T. (2020). Drinking to cope during the COVID-19 pandemic: The role of external and internal stress-related factors in coping motive pathways to alcohol use, solitary drinking, and alcohol problems. Alcoholism: Clinical and Experimental Research. https://doi.org/10.31234/osf.io/8vfp9
Weiss, E. R., Todman, M. W., Maple, E., & Bunn, R. R. (2022). Boredom in a time of uncertainty: State and trait boredom’s associations with psychological health during COVID-19. Behavioral Sciences, 12(8), 298. https://doi.org/10.3390/bs12080298
Westgate, E. C., Buttrick, N., Lin, Y., El Helou, G., Agostini, M., Belanger, J., … Damnjanović, K. (2022). Pandemic boredom: Little evidence that lockdown-related boredom affects risky public health behaviors across 116 countries. https://doi.org/10.31234/osf.io/78kma
Wickrama, K. A. S., Lee, T. K., O’Neal, C. W., & Lorenz, F. O. (2016). Higher-order growth curves and mixture modeling with mplus: A practical guide. Routledge.
Williams, G., & Kibowski, F. (2016). Latent class analysis and latent profile analysis. In D. Glenwick & L. Jason (Eds.), Handbook of methodological approaches to community-based research (pp. 143–151). Oxford University Press.
Woicik, P. A., Stewart, S. H., Pihl, R. O., & Conrod, P. J. (2009). The substance use risk profile scale: A scale measuring traits linked to reinforcement-specific substance use profiles. Addictive Behaviors, 34(12), 1042–1055. https://doi.org/10.1016/j.addbeh.2009.07.001
Wood, R., & Bandura, A. (1989). Impact of conceptions of ability on self-regulatory mechanisms and complex decision making. Journal of Personality and Social Psychology, 56(3), 407–415. https://doi.org/10.1037/0022-3514.56.3.407
World Health Organization (2022). Coronavirus disease (COVID-19) pandemic. [Web site]. 2020. Available at: https://www.who.int/europe/emergencies/situations/covid-19. Accessed 1 July 2022.
Xue, A., Oros, V., La Marca-Ghaemmaghami, P., Scholkmann, F., Righini-Grunder, F., Natalucci, G., Karen, T., Bassler, D., & Restin, T. (2021). New parents experienced lower parenting self-efficacy during the COVID-19 pandemic lockdown. Children, 8(2), 79. https://doi.org/10.3390/children8020079
Yan, L., Gan, Y., Ding, X., Wu, J., & Duan, H. (2021). The relationship between perceived stress and emotional distress during the covid-19 outbreak: Effects of boredom proneness and coping style. Journal of Anxiety Disorders, 77, 102328. https://doi.org/10.1016/j.janxdis.2020.102328
Yıldırım, M., & Güler, A. (2020). Covid-19 severity, self-efficacy, knowledge, preventive behaviors, and mental health in Turkey. Death Studies, 46(4), 979–986. https://doi.org/10.1080/07481187.2020.1793434
Funding
This research was funded by the York University Generic Startup Funds.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study’s conception and design. Material preparation and data collection were performed by Jeffrey D. Wardell and Matthew T. Keough. Data analyses were performed by Veerpal Bambrah and Matthew T. Keough. The first draft of the manuscript was written and revised by Veerpal Bambrah and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
Ethics approval for this study was obtained from the York University Human Participants Review Committee (Ethics certificate number: e2020-118).
Consent to participate
Informed consent was obtained from all individual participants.
Conflicts of interest
The authors have no conflicts of interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Bambrah, V., Wardell, J.D. & Keough, M.T. Longitudinal co-trajectories of depression and alcohol problems in adults during the COVID-19 pandemic. Curr Psychol 43, 14955–14971 (2024). https://doi.org/10.1007/s12144-022-04109-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-022-04109-4