
Abstract
The extent to which and where immigrants’ health may deteriorate in the integration process is less understood. This study extends the current knowledge by focusing on sickness absence in Norway among female immigrants working within eight occupations where few formal skills are required. Administrative register data with a total sample of 261,291 native women and 9251 female refugees or families reunited are used to examine the native-immigrant gap in absence due to sickness during a 10-year period. The main findings are that female immigrants are less likely to have at least one sickness absence spell compared to natives, and that the native-immigrant gap in sickness absence was rather stabile when the number of years worked in these occupations was considered. This study shows that immigrants follow the same pattern as natives and suggests that the native-immigrant gap in absence due to health should be nuanced and focus more on why several years in these occupations increase the probability of sickness absence, independent of country of origin.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Norway ranks amongst the European countries with the highest public spending on incapacity, including paid sick leave, special allowances, and disability-related payments (OECD, 2022) and has one of the highest prevalence of long sickness absence from work (Antczak & Miszczynska, 2021) where women are approximately 50% more absent than men.Footnote 1 Research from Norway shows further that immigrants are more prone to be absent from work due to health compared to Norwegian born (Brekke & Schøne, 2014; Dahl et al., 2010). Sickness absence is closely related to health (Björkenstam et al. 2014) but can also be affected by the poor working environment (e.g., Akay & Ahmadi, 2021) and occupational belonging (Solovieva et al. 2018; Pekkala et al., 2017). Disadvantages in the labour market correlate with higher frequencies of sick leave (e.g., Akay & Ahmadi, 2021) and could lead to an early exit from the labour market and social exclusion (e.g., Dunlavy, Juárez and Rostila 2018). As such, socioeconomic status and immigration background may correlate with variation in sickness absence.
Though the evidence is limited, a systematic review by Sterud et al. (2018) focused on working conditions and occupational health among immigrants in Europe and Canada concluded that, more often than natives, immigrants experience precarious employment that is negatively correlated with health. Especially non-Western immigrants are more prone to work in low-skilled and lower-paid jobs (Behtoui et al., 2020; Ilsøe, 2016; Slavnic & Urban, 2018) with physical demanding work tasks (Dunlavy and Rostila 2013). Further, work-related factors may have a detrimental effect on health, such as the segregation of lower-educated immigrants into lower-paid jobs with poorer job security and working conditions compared to native workers (Taloyan et al., 2019; Charlesworth & Malone, 2022; Hussein, 2022).
The explanations in earlier research on the native-immigrant gap in sickness absence can, to a large extent, be related to factors that stem from differences in socioeconomic status and that immigrants and the majority population work in different occupations. This article extends the current knowledge by weeding out well-documented explanations and focusing explicitly on lower-educated females working in eight occupations where few formal skills are required. Immigrants’ absence due to sickness above 16 days, directed by a physician (hereafter referred to as sickness absence), are compared with the native population (Norwegian-born with at least one Norwegian-born adult). The aim is to determine if immigrants with more years of work have higher sickness absence than immigrants with fewer years of work and if the native-immigrant gap in sickness absence gets tighter after years of work.
The analyses are based on administrative register data with information on age, number of children, immigration status, occupation, and doctor-certificated sick leave. The sample is restricted to female workers aged 21–61 years in eight occupations. The sample of immigrants is further restricted to include refugees and families reunited with formal refugees who immigrated from European non-EU countries (3356), Africa (1556), Asia (4082), or South and Central America (257) to Norway from 2004 to 2008. By examining the native-immigrant gap in sickness absence within occupations where few formal skills are needed, this article will enhance our understanding of the immigrants’ absences due to sickness in occupations where newly arrived immigrants often start their working careers in their new host country.
This article is divided into four sections. The first section provides a brief overview of previous research, theoretical framework, and the institutional context. The second section describes the data source and methodological design. In the third section, the findings are presented, followed by a discussion and conclusions in the final section.
Background
Most of the native-immigrant gap in sickness absence is believed to stem from immigrants’ disadvantages in their work situations relative to natives. Poor host country human capital, such as language, formal skills, and work-relevant experience, has been put forward as a possible explanation for immigrants’ difficulties in entering the labour market (Shields and Price 2002; Chiswick & Miller, 2010) and thus, a selection into low-skilled and physically demanding jobs with less autonomy (Behtoui et al., 2020; Dunlavy and Rostila 2013; Ilsøe, 2016; Shields and Price 2002; Slavnic & Urban, 2018) that adversely affect their health (Sterud et al., 2018). Long-term exposure to demanding and stressful working conditions may affect poor health (Fletcher et al. 2011), as theorised in Karasek’s (1979) demand-control model, which has been used to explain such differences, where demand and lack of control in the work situation cause poor health.
Socioeconomic status, formal education, and poor working conditions are relevant when explaining the native-immigrant gap in sickness absence in general, nevertheless less relevant when solely studying low-skilled women working in a selection of occupations with somewhat similar working conditions (less flexibility and physically demanding working tasks). The assumed correlation between high control over the work situation and less sickness absence (Alexanderson & Norlund, 2004) is relevant if immigrants have less autonomy and opportunity to exercise work tasks and develop their skills in the same type of occupation as their native counterparts. Few studies have focused on such differences, many of which are limited to one occupation or immigrants with a specific country of origin. Studies of migrant nurses have found that language problems and cultural differences are related to less autonomy and the ability to exercise work tasks (Knutsen et al., 2020). Foreign nurses with poor host language skills experience more stress and disempowerment (Magnusdottir 2005; O’Neill, 2011) and are more prone to accept work below their qualifications (Knutsen et al., 2020).
Other explanations on higher sickness absence among immigrants put forward in previous research are related to the stressful migration process itself and exposure to disadvantages in the destination country (Lindstrom et al., 2001; Klinthall & Lindstrom, 2011; Johansson et al. 2012; Gotsens et al., 2015), and that immigrant populations have poorer health and face more health problems compared with the majority population (Taloyan et al., 2006, 2008; Carneiro et al., 2010; Johansson et al. 2012; Witvliet et al., 2014; Lanari et al., 2015). Others argue that, due to a positive migration selection, immigrants are healthier than the native-born population upon arrival in the new host country. This phenomenon is also known as the healthy immigrant effect. The healthy immigrant effect has been found in studies from the USA and Canada and, to a lesser extent, in Western Europe (Helgesson et al., 2019; Kennedy et al., 2015; Vang et al., 2017).
Sickness absence is not the same as an illness but can be seen as a function of both the ability to attend and the motivation to attend (Steers & Rhodes, 1978); therefore, it is regarded as an illness behaviour (Mechanic, 1986). Health-related factors, such as sickness and accidents, are cited as prime factors affecting ability. The ability to attend depends on the possibility of working with health limitations, often related to occupational characteristics. Individuals’ absence behaviour in the presence of health limitations will thus depend on contexts such as access and financial compensation when absent from work. Some studies found that self-reported poor health correlates with sickness absence among immigrants (Brekke & Schøne, 2014; Carneiro et al., 2010). While studies from Denmark found that the correlation between self-reported poor health and sickness absence depends on the occupation. A study among healthcare assistants and healthcare helpers working in the elderly care sector in Denmark by Carneiro et al. (2010) found that despite the immigrants’ poorer health status, they had significantly lower sickness absence than their Danish counterparts, even after controlling for factors such as age and gender. A similar study among cleaners found that immigrants reported poorer health than Danes did. Still, no significant differences in sickness absence between immigrants and Danish cleaners were found (Carneiro et al., 2013). These studies were not designed to identify the reasons behind absence behaviour in the presence of health problems. However, there are certain similarities with Rhodes and Steers’ (1990) theoretical framework of job attendance. In addition to immigrants’ diminished control in the workplace and, on average, poorer health, they may face more pressure to attend work and risk long-lasting unemployment if they lose their job. Although such conditions may be most prevalent at the beginning of a professional career or after recent immigration to a new country, working while ill was more frequent among immigrants than among natives (Agudelo-Suarez et al. 2010) and contributed to poor health (Schultz and Edington 2007).
As this brief overview shows, explanations of the native-immigrant gap in sickness absence are complex and partly contradictory. Focusing explicitly on lower-educated female workers in eight occupations, I asked the first research question: To what extent do immigrants have higher sickness absence than natives when working in similar occupations?
Due to the argument of a positive selection in migration, immigrants could be healthier than natives upon arrival, but their health advantages will deteriorate after years in the host country. Hence, the native-immigrant gap in sickness absence favours immigrants with a few years of work (less absent); the gap could thus be narrower or disfavoured for immigrants with many years of work. Focusing on the sickness absence after years of work, I ask the second research question: Is the native-immigrant gap in sickness absence narrower among those with many years of work compared to those with fewer years of work?
Absence Due to Sickness in a Norwegian Context
The Norwegian sickness benefit system is universal, financed through general taxation, and ranked among the most generous (OECD, 2009). An employee whose occupational activity has lasted for at least 4 weeks is entitled to daily cash benefits, sickness pay, if incapable of working due to illness. Nationality and years of residence are irrelevant if this criterion is met. Daily cash benefits for employees are equal to 100%Footnote 2 of their income and are paid from the first day of sickness for up to 260 working days (52 weeks). The employer is obligated to finance the employee for the first 16 days; afterwards, the Norwegian National Insurance Programme will pay for the leave. An illness lasting more than 3 days requires certification by a general practitioner. A common approach to absenteeism in economics (Brown & Sessions, 1996) is that individuals generally prefer nonwork before work and that motivation for attending work affects the sickness absence behaviour. Due to the Norwegian system, where long-term absence requires certification from a doctor, long-term absence due to sickness is strongly related to illness compared to short-term absence.
Data and empirical strategy
Data
This study employs anonymised data derived from a full-population dataset of Norwegian administrative registers available through microdata.no, enabled by Statistics Norway and Norwegian Social Science Data Services. Statistical analyses are facilitated by an integrated user interface, similar to Stata, but with limitations related to the availability of empirical strategies. The dataset included administrative data on demography, such as age, marital status, number of children, immigration status, and country of origin, and work-related information, such as occupation, employment income, and doctor-certified sick leave.
This study aims to explore sickness absence among lower-educated females with a particular focus on the development of female immigrants’ sickness absence until 10 years after immigration. 2019 is the most recent year with close-to-full data coverage on variables of interest, which make restrictions on the study population and further design of the empirical strategy. First, the immigrant population is restricted to refugees and reunited families who immigrated to Norway from 2004 to 2008. The primary reason for choosing this period was a significant reform introduced in 2003, an introduction programme for humanitarian immigrants, which may affect the measure of interest. The last year of immigration was set to 2008 to give the newly arrived immigrants some time before the analysis began. The immigration population were further limited to those who remained in Norway from their first settlement date until 2019. Second, to ensure that active occupational women are included, as this is a necessary criterion for obtaining doctor-certified sick leave, a set of minimum requirements for earned income in 2019 is needed. Earned income equal to or above the basic amount (BA)Footnote 3 of the national social insurance programme, which is the lowest threshold for earning pension points in the national pension scheme, is used. The earning threshold is low; however, this measure is widely used in register studies in Norway and matches quite well the employment measures used in the labour force sample survey (Bratsberg et al., 2014). Moreover, women on parental leave are excluded. Third, the sample is restricted to women with a high school education level or lower who worked in health services, pre-primary education, administration, trade, accommodation and food service activities, cleaning, and support activities in the measurement period 2010 to 2018. Fourth, to reduce selection bias in and out of the workforce, the age span was set at 21–61 in 2019. The lower age limit was set to 21 to capture those who used some years of the transition from education to work and those who end education at a higher age than 19. The cap was set at 61 years because, at 62, employees can receive early retirement at their own request, which will lead to selection bias out of the labour force among the oldest employees.
The analytical sample is balanced in such a way that all individuals are registered as residents in Norway in the period from 2010 to 2019, and in work in 2019 and at least one more year in the period from 2010 to 2018. However, how many years they have been working in this period will vary. The number of years in work is an important variable for elucidating the significance of immigrant women’s development of sickness absence after immigration. These restrictions leave us with a total sample of 261,291 female natives and 9251 female immigrants who immigrated from non-EU countries (3356), Africa (1556), Asia (4082), and South and Central America (257).
Dependent Variable
Physician-certified absences (sickness absence) measure the number of days paid by the National Insurance Administration, which includes 17 days and above. There is no information on self-certified absences (1–3 days) and absence paid by the employer (less than 17 days) in the dataset. Self-certified absences and sickness absences paid by the employer have the value zero, together with respondents with no absence spells, whereas sickness absences of 17 days and above are measured continuously. Thus, the measurement of days absent due to sickness is left censored and a latent continuous response of physician-certified absences. All of the observations are included in the dataset, but we do not know the “true” value of observations with sickness absence of less than 17 days. Given the form of the data and the nature of the outcomes, it is reasonable to organise the outcome as a dichotomous variable. One refers to at least 17 days absent due to sickness in 2019, while zero refers to 16 days or less.
Control Variables
The focus of this article is to study the native-immigrant gap in sickness absence among lower-educated female workers within eight occupations in a 10-year period. Though the selection of occupations gives more homogeneous groups, the two samples (native and immigrant) will differ with regard to a number of individual characteristics. Thus, a set of control variables were included to show sensitivity with respect to conditions such as age, marital status, number of children in the household, and part-time work. The control variables used were divided into work-related and individual characteristics.
Primarily, the group with the most individuals for the immigrant sample is chosen as a reference, except for age. This is because 10 years of work is used as the reference category in the model 4, thus 40–49 is then a more relevant group to use due to the combination of years in work and age, especially among the immigrant sample. The sample comprises a selection of occupations that do not require higher education in eight industries. The two-digit Standard Industrial Classification (SIC2007) was used to select occupations based on coding units according to the most important activities in Statistics Norway’s Business Register and the Central Coordinating Register for Legal Entities. SIC2007 allows for comparisons over time and across countries. Occupation is organised as eight dummy variables: residential care activities (reference group), retail trade, except of motor vehicles and motorcycles, accommodation and food service activities, cleaning and support activities, public administration and defence, education (pre-primary education), human health activities, and social work activities without accommodation.
Hours at work are included as a dummy variable where full-time employment is coded as one if the agreed working hours are above 19 h a week; otherwise, it is coded as zero and referred to as part-time (reference). Years in work (2010–2019) are derived from individual annual earnings,Footnote 4 where earnings above the BA for each respective yearFootnote 5 are defined as work. Each year of employment is summarised and organised into 10 dummy variables. This measure is not directly comparable because native workers, in particular, may have worked several years before 2010, which are not calculated in this data. Age was measured in 2019 and organised into four dummy variables: 21–30, 31–40, 41–50 (reference group), and 51–61. The number of children in the household under 18 years of age was measured in 2019. It includes four dummy variables in which no children are the reference group, and the other three dummy variables are 1, 2, or more than 3 children. The reference group is chosen due to research that shows that having children is positively correlated with higher sickness absence behaviour (Floderus et al., 2012; Mastekaasa, 2020; Melsom & Mastekaasa, 2018; Nilsen et al., 2017). Marital status was organised into three dummy variables: married or cohabiting (reference group), unmarried, and divorced or widowed.
Empirical Strategy
The objectives of this study were twofold. First, to test if there are differences in the correlation between occupational categories and sickness absence between natives and immigrants. Second, examine the correlation between years in work and female immigrants’ sickness absence during a 10-year period, at the beginning of their careers in their new host country (Norway), compared to their native counterparts.
Although the dependent variable is dichotomous, I prefer to follow the trend of using linear probability models (LPM) instead of logistic regression. The primary advantage of LPM is its interpretability. A one-unit increase in X1 is associated with a percentage point increase in the probability that Y (e.g., sickness absence) is one. Moreover, as native and immigrants differ in their individual characteristics and available information in the data used, split sample analyses can be beneficial as the covariates within each group are allowed to vary. Further, as all analyses were performed separately among the native and the immigrant sample and several models were used, LPM is beneficial to use as coefficients across models and across samples can be compared. As coefficients in logistic regressions depend both on effect sizes and the magnitude of unobserved heterogeneity, coefficients across samples, across groups within samples, or across models with different independent variables within the same sample, cannot be compared straightforwardly (Mood, 2010). The LPM and logistic regression fit about equally if the probabilities of the dependent variable are moderate (between 0.20 and 0.80). In this case, 38.5% of the native sample and 25.9% of the immigrant sample had at least one sickness absence spell during the measurement period, thus, within the preferred range. A potential problem of using a LPM when the dependent variable is dichotomous is that the error terms could be heteroskedastic. This will not cause bias in the coefficient estimates, but can make them less precise, thus give statistically significant estimates on an incorrect basis. Due to heteroscedasticity, robust standard errors were used in all analyses and logistic regression was used on all analyses without violating the results (Table 4 in the Appendix).
Findings
Descriptive statistics of explanatory variables are given in Table 1. Among natives, 35.5% had at least one sickness absence spell in 2019, compared with 25.9% among immigrants. The native–immigrant gap reflects that, on average, native workers are more prone to be absent due to sickness within these occupations. However, individual differences between these two groups were not considered. The age distribution of the natives follows a U-curve, while the opposite is found among immigrants. The most significant difference is found among the oldest age group (50–61), where the proportion of the natives (33.6%) is more than three times as large as the immigrants (7.3%). The differences in age distribution are also reflected in the number of children in the household. The most significant proportion of natives had no children under 19 in the home, while it was the most common among immigrants. In terms of marital status, about half of the natives were unmarried, in contrast to 32% of the immigrants. Furthermore, 35.8% of the natives and 52% of the immigrants were married or cohabiting; the lowest proportion of natives (13.1%) and immigrants (16.1%) was in the category of divorced, widowed, or surviving partners.
The most significant proportion of the sample was employed in the healthcare sector. Residential care activities were the largest category among immigrants (31.9%), in contrast, 18.3% of the natives worked in the same occupation. The differences between natives and immigrants were significantly smaller in social work activities without accommodation (19.5% and 15.1%) and in human health activities (14% and 9.3%). The proportion of workers in pre-primary education, public administration and services and sales was higher among natives than immigrants, whereas the opposite was found in support activities. Regarding years of work, the proportion of those who had worked 10 years was the largest category for both groups. However, the number of natives who had worked for 10 years was markedly higher (62.2%) than immigrants (18.1%).
To sum up, the descriptive statistics show that immigrants were generally younger and had fewer years of work between 2010 and 2019, which are assumed to predict lower sickness absence. In contrast, they had in general more children below 19 years of age in the household, that are more likely to be positively correlated with higher sickness absence behaviour (Mastekaasa, 2020; Melsom & Mastekaasa, 2018).
Table 2 shows the results of the linear probability model. All analyses were conducted separately for natives and immigrants and included four models. The first three models estimate the correlation between sickness absence and occupation (Model 1), individual characteristics, including full-time work (Model 2), and number of years employed from 2010 to 2019 (Model 3). To test the sensitivity and how occupations, individual characteristics, and years employed correlated with sickness absence, all variables of interest were included in Model 4 (Table 3 in the Appendix).
When using LPM, the estimates between the separate analyses of natives and immigrants can be compared. In Model 1, the coefficient of the reference group (residential care activities) indicated that 43% of the native workers had at least one sickness absence of more than 16 days in 2019. In contrast, immigrants in the same occupation had a 19% points lower probability of sickness absence. With workers in residential care as a reference, a different pattern between natives and immigrants was observed. Among natives, workers in the other occupations, except cleaning and support activities and social work activities without accommodation, had a significantly lower probability of sickness absence. In particular, two occupations deviated from the other occupations. Native workers in services and sales and accommodations and food service had respectively 11.7 and 13.1 percentage point lower probability of sickness absence compared to the reference group. In contrast, the opposite pattern was found among immigrants. Except for immigrants who worked in accommodations and food services, with a 2.6 percentage points lower probability of sickness absence (borderline significant), all the other groupsFootnote 6 had a higher probability of sickness absence compared to the reference group.
Model 2 showed that the probability of sickness absence among natives who are married, in the age group 40–49 and with no children in the household, was 32%. Their immigrant counterparts were 19 percentage point less likely to have sickness absence in the same period. Natives were generally older than the immigrants, which may explain some of the differences in the sickness absence. The probability of sickness absence among natives in the youngest age group (20–29 years) was markedly lower, 12 percentage points, compared to the reference group (40–49 years). The other age groups had a marginally higher sickness absence than the reference group. Such a pattern was not found among immigrants. The only significant estimate was found in the age group 30–39, which had three percentage points higher probability of sickness absence compared to the reference group (40–49 years).
The pattern among natives and immigrants regarding the correlation between marital status and sickness absence was rather equal. Though the level of sickness absence differed, unmarried persons had the lowest probability of sickness absence, followed by married and cohabiting (reference category), and divorced or widowed persons. Having children generally results in a higher probability of sickness absence among natives. This relationship was not found among immigrants. The lack of significant results among immigrants could result from the sample size and selection bias such as female immigrants, more than natives, might exit the labour market for a more extended period when having children. Moreover, working full-time is positively correlated with higher sickness absence. Natives working full-time had 7 percentage points higher probability of sickness absence compared to natives who worked part-time. The same relationship was found among immigrants (11 percentage points).
The coefficients in Model 3 showed that the correlation between sickness absence and years of work from 2010 to 2019 was approximately linear for both groups. Although this study does not follow the same individuals over time, the results illustrate that the probability of sickness absence was positively correlated with more years of work among lower-educated workers in the eight selected occupations.
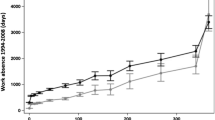
The results from Model 4 are visualised in Fig. 1. and present estimated sickness absence probabilities after years of work for natives and immigrants, including controls for occupations, individual characteristics (see Table 3 in the Appendix).

The probability of sickness absence above 16 days among natives and immigrants after number of years in work in the period 2010–2019. Control variables: occupation, fulltime, age, marital status, number of children in household
The bars in Fig. 1 are based on the results from Model 4 and show the probability of sickness absence in 2019 after how many years natives and immigrants has worked in the period from 2010 to 2019. The main picture is that natives who have worked more years in the 10-year period had a higher probability of sickness absence in 2019 compared to natives with fevers years of work in the same period. One exception is those who have worked for 10 years, they have a lower probability of sickness absence compared to those who have worked 9 years. A possible explanation could be due to a positive health selection of natives who worked at least 10 years in these occupations. However, this difference is significant but small, in order to clarify whether this is due to health selection or randomness, there is a need for information on more years and an extension of the evaluation period. The same picture mainly applies to immigrants as well, those who have worked within these occupations for 10 years, during 2010 to 2019, have a significant higher probability of sickness absence (except those working nine years) compared to immigrants with fevers years in work in the same 10-year period.
The native-immigrant gap in sickness absence seems to be rather stable in the 10-year period, and there is a clear tendency that the probability of sickness absence in 2019 correlates with the number of years within these occupations. There are few indications that points in the direction that the native-immigrant gap between those who have worked for several years is in general smaller than those with few years of work within these occupations.
Concluding Discussion
This study aimed to explore the native-immigrant gap in sickness absence by focusing on explanations other than gender, educational attainment, and occupational skills, which explain a large part of the differences in sickness absence. By weeding out well-documented explanations, the focus in this article is on the importance of individual characteristics and the number of years worked from 2010 to 2019 on sickness absence among lower-educated female workers in eight occupations where few formal skills are required. As such, this article adds to the existing literature by examining the native-immigrant gap in sickness absence and the development of immigrants’ sickness absence at the beginning of their working careers in the new host country (Norway).
There are two important findings from this study. One is that female immigrants are less likely to have sickness absence spell compared to natives who work in the same occupations. These results correspond with studies on the native-immigrant gap in sickness absence in which the study population is restricted to one or a few occupations (Carneiro et al., 2010, 2013). At least two factors could explain the lower sickness absence among immigrants in this study. First, although restrictions, such as occupation and educational level, are used to make the study population more homogeneous, and important individual characteristics are included as control variables, the analyses are not designed to control for selection biases related to health and the number of years worked. The natives in this study were older and had more years of work during the measurement period, and probably before the measurement period as well, compared to the immigrants. If poor health is correlated with age and years of work, this will have an independent effect on sickness absence that is not captured in this study. Second, there might be a selection out of the labour market that is stronger for immigrants than natives. In this study, having children results in a higher probability of sickness absence among natives, but not among immigrants. The lack of significant results could stem from the sample size, or that female immigrants may exit the labour market for a more extended period when having children. Accordingly, there could be a positive health selection of employed immigrants with children in this study.
The other is that none of the results indicated that the native-immigrant gap in sickness absence was narrower among those with more years of work. This study did not follow the same individuals over time but conducted analogue analyses between natives and immigrants with an equal number of years worked. However, as natives and immigrants follow the same pattern, a plausible suggestion is that the higher probability of sickness absence among those with more years worked could be affected by poor working conditions or a positive health selection of workers with more years in these occupations.
There are many advantages of using register data, but it also has limitations. Based on the available data sources in this study, doctor-certified sick leave absence as a measure of health is used, which is potentially fallacious. The alleged native–immigrant gap in sickness absence, that immigrants are more prone to be absent from work due to sickness, may be underestimated if work attendance when sick is more common among immigrants than natives. If so, this could be due to motivation to attend, but also lack of knowledge of legislations and their rights, or refusal to consult a doctor. The latter is particularly relevant in this study, as long-term absence that requires certification from a physician is used. In addition, register data lack information on the working environment, a potential contributor to individuals’ poor health related to work. Such information would benefit this study’s findings. Future research could take advantage of a more detailed measures of working environments and health at different periods over employee careers. This would elucidate whether the native-immigrant gap in sickness absence results from health differences or a deterioration of health over time in occupations characterised by few opportunities for development and often poor working conditions.
Notwithstanding these limitations, this study adds to the current knowledge on the native-immigrant gap by focusing on sickness absence among lower-educated females working within eight occupations where few formal skills are required. This study shows that the previous assumption that immigrants are more absent due to health issues should be nuanced. The focus should be on explanations of why several years in these occupations increase the probability of sickness absence, independent of country of origin.
Data Availability
As I am using registerdata, this is not available for everyone, but access to data can be applied for at microdata.no, but mainly for Norwegian researchers. Data source: microdata.no.
Notes
This figure is up to a ceiling of six times the basic amount (B.A) (58,878 EUR in 2019), but most employers replace foregone earnings above the limit.
The base amount is adjusted each year. B.A. 2019: 99 858 NOK, 9 813 EUR.
Includes wages and salaries from paid employment as well as net entrepreneurial income and gross taxes measured at the end of the year.
BA for the respective years in EUR: 2010 = 75,641, 2011 = 79,216, 2012 = 81,153, 2013 = 84,204, 2014 = 87,328, 2015 = 90,068, 2016 = 92,576, 2017 = 93,634, 2018 = 96,883, 2019 = 99,858.
The occupation categories: services and sale, and public administrations are not significant.
References
Akay, P. A., & Ahmadi, N. (2021). The work environment of immigrant employees in sweden—a systematic review. Int Migration & Integration, 23, 2235–2268. https://doi.org/10.1007/s12134-021-00931-0
Alexanderson, K., & Norlund, A. (2004). Aim, background, key concepts, regulations, and current statistics. Scandinavian Journal of Public Health, 32(63), 12–30.
Agudelo-Suárez, A. A., Benavides, F. G., Felt, E., et al. (2010). Sickness presenteeism in Spanish-born and immigrant workers in Spain. BMC Public Health, 10, 791. https://doi.org/10.1186/1471-2458-10-791
Antczak, E., & Miszczynska, K. M. (2021). Causes of sickness absenteeism in Europe—Analysis from an intercountry and gender perspective. International Journal of Environmental Research and Public Health, 18, 11823. https://doi.org/10.3390/ijerph182211823
Bratsberg, B., Raaum, O., & Røed, K. (2014). Immigrants, labour market performance and social insurance. The Economic Journal, 124(580), F644–F683.
Behtoui, A., Boréus, K., Neergaard, A., & Yazdanpanah, S. (2020). Why are care workers from the global south disadvantaged? Inequality and discrimination in Swedish elderly care work, Ethnic and Racial Studies, 43(16), 155–174. https://doi.org/10.1080/01419870.2020.1734220
Björkenstam, E., Weitoft, G. R., Lindholm, C., et al. (2014). Associations between number of sick-leave days and future all-cause and cause-specific mortality: a population basedcohort study. BMC Public Health, 14, 733. https://doi.org/10.1186/1471-2458-14-733
Brekke, I., & Schøne, P. (2014). Long sickness absence differences between natives and immigrant workers: The role of differences in self-reported health. Journal of International Migration and Integration, 15(2), 217–235.
Brown, S., & Sessions, J. G. (1996). The economics of absence: Theory and evidence. Journal of Economic Surveys, 10(1), 23–53.
Carneiro, I. G., Ortega, A., Borg, V., & Hogh, A. (2010). Health and sickness absence in Denmark: A study of elderly-care immigrant workers. Journal of Immigrant and Minority Health, 12(1), 43–52.
Carneiro, I. G., Rasmussen, C. D., Jørgensen, M. B., Flyvholm, M. A., Olesen, K., Madeleine, P.,... and Holtermann, A. (2013). The association between health and sickness absence among Danish and non-Western immigrant cleaners in Denmark, International archives of occupational and environmental health, 86(4), 397-405
Charlesworth, S., and Malone, J. (2022). The production of employment conditions for migrant care workers: Cross national perspectives. Social Policy and Society, 1–14. https://doi.org/10.1017/S1474746422000100
Chiswick, B. R., & Miller, P. W. (2010). Occupational language requirements and the value of English in the US labor market. Journal of Population Economics, 23(1), 353–372.
Chiswick, B. R., Lee, L. Y., & Miller, P. W. (2008). Immigrant selection systems and immigrant health. Contemporary Economic Policy, 26(4), 555–578.
Dahl, S. A., Hansen, H. T., & Olsen, K. M. (2010). Sickness absence among immigrants in Norway, 1992–2003. Acta Sociologica, 53(1), 35–52.
Dunlavy, A. C., Juárez, S., & Rostila, M. (2018). Employment status and risk of all-cause mortality among native- and foreign-origin persons in Sweden. European Journal of Public Health, 28(5), 891–897. https://doi.org/10.1093/eurpub/cky090
Dunlavy, A. C., & Rostila, M. (2013). Health inequalities among workers with a foreign background in sweden: do working conditions matter? International Journal of Environmental Research and Public Health., 10(7), 2871–2887. https://doi.org/10.3390/ijerph10072871
Fletcher, J. M., Sindelar, J. L., & Yamaguchi, S. (2011). Cumulative effects of job characteristics on health. Health Economics, 20, 553–570. https://doi.org/10.1002/hec.1616
Floderus, B., Hagman, M., Aronsson, G., Marklund, S., & Wikman, A. (2012). Medically certified sickness absence with insurance benefits in women with and without children. The European Journal of Public Health, 22(1), 85–92.
Gotsens, M., Malmusi, D., Villarroel, N., Vives-Cases, C., Garcia-Subirats, I., Hernando, C., & Borrell, C. (2015). Health inequality between immigrants and natives in Spain: The loss of the healthy immigrant effect in times of economic crisis. The European Journal of Public Health, 25(6), 923–929.
Helgesson, M., Johansson, B., Nordquist, T., Vingård, E., & Svartengren, M. (2019). Healthy migrant effect in the Swedish context: a register-based, longitudinal cohort study. BMJ Open, 9, e026972. https://doi.org/10.1136/bmjopen-2018-026972
Hussein, S. (2022). Employment inequalities among British minority ethnic workers in health and social care at the time of Covid-19: A rapid review of the literature. Social Policy and Society, 21(2), 316–330.
Ilsøe, A. (2016). From living wage to living hours – The Nordic version of the working poor. Labour & Industry: A Journal of the Social and Economic Relations of Work, 26(1), 40–57. https://doi.org/10.1080/10301763.2016.1152534
Johansson, B., Helgesson, M., Lundberg, I., et al. (2012). Work and health among immigrants and native Swedes 1990–2008: a register-based study on hospitalization for common potentially work-related disorders, disability pension and mortality. BMC Public Health, 12, 845. https://doi.org/10.1186/1471-2458-12-845
Karasek, R. A., Jr. (1979). Job demands, job decision latitude, and mental strain: Implications for job redesign. Administrative Science Quarterly, 24(2), 285–308.
Kennedy, S., Kidd, M. P., McDonald, J. T., & Biddle, N. (2015). The healthy immigrant effect: Patterns and evidence from four countries. Journal of International Migration and Integration, 16(2), 317–332.
Klinthall, M., & Lindstrom, M. (2011). Migration and health: A study of effects of early life experiences and current socioeconomic situation on mortality of immigrants in Sweden. Ethnicity and Health, 16(6), 601–623.
Knutsen, H. M., Fangen, K., & Žabko, O. (2020). Integration and exclusion at work: Latvian and Swedish agency nurses in Norway. Journal of International Migration and Integration, 21(2), 413–429.
Lanari, D., Bussini, O., & Minelli, L. (2015). Self-perceived health among Eastern European immigrants over 50 living in Western Europe. International Journal of Public Health, 60(1), 21–31.
Lindstrom, M., Sundquist, J., & Ostergren, P. O. (2001). Ethnic differences in self-reported health in Malmo in southern Sweden. Journal of Epidemiology and Community Health, 55(2), 97–103.
Magnusdottir, H. (2005). Overcoming strangeness and communication barriers: a phenomenological study of becoming a foreign nurse. International Nursing Review, 52(4), 263–269.
Mastekaasa, A. (2020). Absenteeism in the public and the private sector: Does the public sector attract high absence employees? Journal of Public Administration Research and Theory, 30(1), 60–76.
Mechanic, D. (1986). The concept of illness behaviour: Culture, situation and personal predisposition1. Psychological Medicine, 16(1), 1–7.
Melsom, A. M., & Mastekaasa, A. (2018). Gender, occupational gender segregation and sickness absence: Longitudinal evidence. Acta Sociologica, 61(3), 227–245.
Mood, C. (2010). Logistic regression: Why we cannot do what we think we can do and what we can do about it. European Sociological Review., 26(1), 67–82.
Nilsen, W., Skipstein, A., Østby, K. A., & Mykletun, A. (2017). Examination of the double burden hypothesis – A systematic review of work-family conflict and sickness absence. European Journal of Public Health, 27(3), 465–471.
O’Neill, F. (2011). From language classroom to clinical context: The role of language and culture in communication of nurses using English as a second language. A Thematic Analysis, International Journal of Nursing Studies, 48(9), 1120–1128.
OECD. (2009). Employment outlook. OECD.
OECD (2022). Public spending on incapacity (indicator). https://doi.org/10.1787/f35b71ed-en
Pekkala, J., Blomgren, J., Pietiläinen, O., Lahelma, E., & Rahkonen, O. (2017). Occupational class differences in diagnostic-specific sickness absence: A register-based study in the Finnish population, 2005–2014. BMC Public Health, 17, 670. https://doi.org/10.1186/s12889-017-4674-0
Rhodes, S. R., & Steers, R. M. (1990). Managing employee absenteeism. Addison Wesley Publishing Company.
Shields, M. A., & Price, S. W. (2002). Racial harassment, job satisfaction and intentions to quit: evidence from the British nursing profession. Economica, 69(274), 295–326.
Schultz, A. B., & Edington, D. W. (2007). Employee health and presenteeism: a systematic review. J Occupational Rehabilitation, 17, 547–579. https://doi.org/10.1007/s10926-007-9096
Solovieva, S., Leinonen, T., Husgafvel-Pursiainen, K., Heliövaara, M., & Viikari-Juntura E. (2018) Occupational differences in sickness presenteeism trend. European Journal of Public Health, 28(suppl_4)
Slavnic, Z., & Urban, S. (2018). Meandering rides of the Swedish taxi industry: Flourishing entrepreneurship or ethnic segmentation? International Journal of Sociology and Social Policy, 38(5), 444–458.
Steers, R. M., & Rhodes, S. R. (1978). Major influences on employee attendance: A process model. Journal of Applied Psychology, 63(4), 391.
Sterud, T., Tynes, T., Mehlum, I. S., Veiersted, K. B., Bergbom, B., Airila, A., Johansson, B., Brendler-Lindqvist, M., Hviid, K., and Flyvholm, M. A. (2018). A systematic review of working conditions and occupational health among immigrants in Europe and Canada, BMC public health, 18(1), 1-15
Taloyan, M., Johansson, L. M., Johansson, S. E., Sundquist, J., & Kocturk, T. O. (2006). Poor self-reported health and sleeping difficulties among Kurdish immigrant men in Sweden. Transcultural Psychiatry, 43(3), 445–461.
Taloyan, M., Johansson, S. E., Sundquist, J., Kocturk, T. O., & Johansson, L. M. (2008). Psychological distress among Kurdish immigrants in Sweden. Scandinavian Journal of Public Health, 36(2), 190–196.
Taloyan, M., Westerlund, H., Aronsson, G., & Östergren, P. O. (2019). Does labor market position explain the differences in self-rated health between employed immigrants and native Swedes?: A population-based study from Southern Sweden. Journal of International Migration and Integration, 20(3), 703–715.
Vang, Z. M., Sigouin, J., Flenon, A., & Gagnon, A. (2017). Are immigrants healthier than native-born Canadians? A Systematic Review of the Healthy Immigrant Effect in Canada, Ethnicity and Health, 22(3), 209–241.
Witvliet, M. I., Arah, O. A., Stronks, K., & Kunst, A. E. (2014). Examining self-rated health of young central and eastern Europeans in the context of other world regions. European Journal of Public Health, 24(2), 314–321.
Acknowledgements
This article has benefited from valuable comments from two anonymous reviewers, and Justyna Bell and Therese Dokken. All errors are the author’s own.
Funding
Open access funding provided by OsloMet - Oslo Metropolitan University This work was supported by the Research Council of Norway (grant number 270838).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing Interests
The author declares no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ugreninov, E. Absence Due to Sickness Among Female Immigrants: Disadvantages Over the Career?. Int. Migration & Integration 24, 1455–1475 (2023). https://doi.org/10.1007/s12134-023-01016-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12134-023-01016-w