
Abstract
Objectives
To determine efficacy of non-invasive positive pressure face mask ventilation using a ventilator device (NIPPmV) for achieving early effective ventilation compared to that by self-inflating bag (SIB) or T- piece resuscitator (TPR).
Methods
The authors video recorded 33 trained resuscitators using NIPPmV (provided using ventilator device), SIB [a 500 ml silicone SIB without a positive end expiratory pressure (PEEP) valve] and a TPR. Using a continuous pressure recording system and a neonatal manikin, the authors evaluated the efficacy of the ventilation to achieve early effective ventilation during 30 s of ventilation. The primary outcome was time to achieve effective chest rise. Secondary outcomes were peak inspiratory pressure (PIP), ventilation rate and the need to perform ventilation corrective steps during positive pressure ventilation (PPV) among the devices.
Results
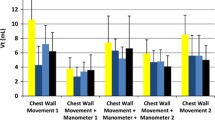
Total 99 videos were recorded. The time(s) taken to achieve the first chest rise was significantly lesser in NIPPmV group compared to SIB and TPR (3.0 ± 1.7 vs. 3.7 ± 1.9 vs. 7.5 ± 5.4, respectively, p <0.001). The mean PIP delivered by NIPPmV compared to SIB & TPR (19.8 ± 1.6 vs. 35.6 ± 7.4 vs. 17.8 ± 2.0 cm H20 respectively; p <0.001) was more accurate with preset PIP. Ventilation, in terms of breath rate, was observed to be controlled more accurately with NIPPmV compared to SIB & TPR (50 vs. 42 vs. 33 per min respectively; p <0.001).
Conclusions
The non-invasive positive pressure face mask ventilation using a ventilator (NIPPmV) resulted in achieving early, effective and consistent ventilation.

Similar content being viewed by others
References
Liu L, Oza S, Hogan D, et al. Global, regional, and national causes of child mortality in 2000–13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet. 2015;385:430–40.
Aziz K, Lee CHC, Escobedo MB, et al. Part 5: Neonatal Resuscitation 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Pediatrics. 2021;147:e2020038505E.
Hussey SG, Ryan CA, Murphy BP. Comparison of three manual ventilation devices using an intubated mannequin. Arch Dis Child Fetal Neonatal Ed. 2004;89:F490–3.
Augustine JA, Seidel DR, McCabe JB. Ventilation performance using a self-inflating anesthesia bag: effect of operator characteristics. Am J Emerg Med. 1987;5:267–70.
Leone TA, Finer NN, Rich W. Delivery room respiratory management of the term and preterm infant. Clin Perinatol. 2012;39:431–40.
Goudar SS, Somannavar MS, Clark R, et al. Stillbirth and newborn mortality in India after helping babies breathe training. Pediatrics. 2013;131:e344–52.
Lemyre B, Davis PG, de Paoli AG. Nasal intermittent positive pressure ventilation (NIPPV) versus nasal continuous positive airway pressure (NCPAP) for apnea of prematurity. Cochrane Database Syst Rev. 2002;1:CD002272.
Laurie-Rose C, Frey M, Ennis A, Zamary A. Measuring perceived mental workload in children. Am J Psychol. 2014;127:107–25.
Roehr CC, Davis PG, Weiner GM, Jonathan Wyllie J, Wyckoff MH, Trevisanuto D. T-piece resuscitator or self-inflating bag during neonatal resuscitation: a scoping review. Pediatr Res. 2021;89:760–6.
Trevisanuto D, Roehr CC, Davis PG, et al. Devices for administering ventilation at birth: a systematic review. Pediatrics. 2021;148:e2021050174.
Whyte SD, Sinha AK, Wyllie JP. Neonatal resuscitation: a practical assessment. Resuscitation. 1999;40:21–5.
Acknowledgements
The authors sincerely thank Dr. Niranjan Khambete from Department of Clinical Engineering, for his inputs during data collection and Dr. Rajan Joshi HOD Pediatrics, for his valuable inputs while preparing the manuscript. The authors also thank team PediSTARS, Dr Jennifer Arnold, Dr Jonathan Duff, INSPIRE scientific review committee and IPSSV for their valuable inputs during initial designing of the study. They also thank CAE Healthcare for providing CAE Luna baby simulator for the study purpose.
Author information
Authors and Affiliations
Contributions
SK conceptualized and designed the study. She collected the data, wrote initial draft and gave final approval. VU collected the data, did literature search, revised the manuscript critically and gave final approval. AVM analysed and interpreted the data, revised the manuscript critically for important intellectual content and approved the final manuscript. APP collected the data, did literature search, revised the manuscript and approved the final manuscript.
Corresponding author
Ethics declarations
Guarantor
Dr Rajan Joshi, Head, Department of Pediatrics, Deenanath Mangeshkar Hospital, Pune
Conflict of Interest
None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kalane, S., Upadhye, V., Mulay, A.V. et al. Comparison of Efficacy of Pressure Controlled vs. Traditional Manual Mask Ventilation for Newborn Resuscitation – A Simulation-Based Pilot Randomized Control Trial. Indian J Pediatr (2023). https://doi.org/10.1007/s12098-023-04938-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s12098-023-04938-6