
Abstract
Hepatic encephalopathy, characterized by mental status changes and neuropsychiatric impairment, is associated with chronic liver disease as well as acute liver failure. In children, its clinical manifestations can be challenging to pinpoint. However, careful assessment for the development of hepatic encephalopathy is imperative when caring for these patients as progression of symptoms can indicate impending cerebral edema and systemic deterioration. Hepatic encephalopathy can present with hyperammonemia, but it is important to note that the degree of hyperammonemia is not indicative of severity of clinical manifestations. Newer forms of assessment are undergoing further research, and include imaging, EEG and neurobiomarkers. Mainstay of treatment currently includes management of underlying cause of liver disease, as well as reduction of hyperammonemia with either enteral medications such as lactulose and rifaximin, or even with extracorporeal liver support modalities.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Hepatic encephalopathy (HE) is defined as neuropsychiatric impairment and mental status changes that present in patients with liver disease [1, 2]. Patients with HE are at risk of developing cerebral edema, and its diagnosis and grading can be particularly challenging in pediatrics depending on a child’s age, developmental achievements, and easily confused symptoms. These patients require close monitoring while inpatient and may develop progressive or waxing and waning symptoms. Patients with acute liver failure or chronic liver disease may both be afflicted, though with slightly different presentations. Episodes of HE may be prompted by sepsis, upper gastrointestinal tract bleeding, dehydration, constipation, ileus, or small bowel obstruction, among other things [1, 3]. Degree of HE can be exacerbated by a variety of mechanisms including oxidative stress, hyperinflammatory states, altered cerebral blood flow and metabolic derangements. Best clinical care for these patients takes place in an experienced liver transplant center. This discussion will focus on the clinical presentation, grading and management of HE in children, as well as introduce areas of ongoing research.
Pathogenesis of HE
The underlying mechanism of HE is not well-defined, but multiple theories have been proposed. One leading hypothesis surrounds gut-derived toxins and hyperammonemia, though other possibilities involve altered bile acids, cytokines, and chemokines [1, 4]. Ammonia is a byproduct of bacterial metabolism of both proteins and other nitrogenous compounds in the large intestine and is also generated during glutamine metabolism in small bowel enterocytes. A majority of ammonia is typically metabolized to an innocuous by-product (urea), during first-pass metabolism in the liver via the portal vein, which is then excreted [5]. As such, in the setting of liver disease which disrupts this natural blood flow, metabolism and excretion of ammonia is inhibited, leading to hyperammonemia and its increased passage across the blood-brain barrier [1]. In the brain, ammonia is postulated to cause cerebral edema by inducing swelling of type II astrocytes [1]. It is important to keep in mind that there is minimal, if any, clinical correlation between level of hyperammonemia and degree of HE. However, in the setting of extreme elevations, studies have shown increased risk of cerebral herniation when ammonia levels reach >200 μmol/L [4].
Additionally, accurate ammonia levels can be difficult to obtain. While arterial samples are the gold standard, these are not always feasible in the pediatric clinical setting. When collected as a venous sample, the level must be measured off of a specimen obtained from a free-flowing (without use of a tourniquet or clenching of the fist) blood draw, to minimize chances of a falsely elevated ammonia level due to excess release from skeletal muscle [1]. Finally, the specimen must be immediately placed on ice and transported to the lab to be processed within 20 min of collection. As such, there is high probability of invalid results which further highlights the caution clinicians should implement when assessing hyperammonemia to make clinical decisions.
Clinical Considerations and Classification of HE
HE associated with acute liver failure is known as Type A HE [1, 2]. Patients with HE due to portosystemic shunting but no underlying liver disease are categorized as Type B HE [1, 2]. Chronic liver disease with cirrhosis or portal hypertension, and HE, are known as Type C [1, 2]. Within Type C HE, there are several different forms: covert, persistent and episodic. Episodic encephalopathy changes in severity and duration; recurrent encephalopathy is defined as more than 2 episodes in one year; persistent encephalopathy is defined as cognitive impairment that limits activities of daily living for a period of more than 2 wk [1]. This classification system is summarized in Fig. 1.

Classification of Hepatic Encephalopathy (HE) phenotypes.
Portosystemic shunts direct intestinal blood flow bypassing the liver, meaning neurotoxic intestinal metabolites that would have typically been metabolized by the liver are instead directed into the systemic circulation. These compounds can cross the blood-brain barrier, leading to clinical encephalopathy. In particular, patients who have undergone transjugular intrahepatic portosystemic shunt (TIPS) have been shown to develop HE at fairly high rates (~50%) [2]. However, TIPS is only used in the older adolescent population in the pediatric age group.
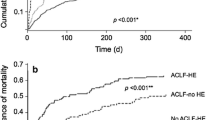
Patients with acute liver failure and encephalopathy are at higher risk of developing seizures and cerebral edema along with hyperammonemia than are patients with chronic liver disease. Of note, cerebral edema tends to be rarer in patients with chronic liver disease, possibly due to underlying cerebral atrophy [1]. Overall, patients with acute liver failure and HE have a higher risk of mortality and more often require emergent liver transplantation than do patients with chronic liver disease whose disease progression may be more subtle [4, 6]. For patients with acute on chronic liver disease, HE is often used as a diagnostic criterion for the acute episode of decompensation, and grade 3-4 HE may be associated with increased mortality in this population [7,8,9]. These patients, who present with sudden worsening of known underlying liver disease or cirrhosis as indicated by progression of ascites, gastrointestinal bleeding, cholangitis, infection or development of HE, often go on to develop multi organ system failure and progressive HE in the setting of acute on chronic liver failure [7, 8]. Children with acute on chronic liver failure have been known to experience increased mortality, but further research is needed to clarify the mechanisms and pathophysiology [7,8,9].
Grading of Hepatic Encephalopathy
Standard grading of pediatric HE tends to rely on West Haven criteria (Table 1). The scoring systems have been established using adult data but are also adapted to the pediatric population. HE can be vague in children, with subtle clinical changes in mental status such as those listed in Table 2, still notable of progressive encephalopathic changes. Signs of pediatric HE may include irritability, fatigue, confusion, and can progress to coma (Table 2). As such, some of the signs of ongoing HE may initially be overlooked by the medical team as they can be attributed to expected child behavior in a hospital setting. In chronic liver disease, presentation may be more indolent as many patients have underlying cerebral atrophy.
Minimal Hepatic Encephalopathy
Minimal encephalopathy may also be known as grade 1 as scored with the West Haven Criteria. This degree of encephalopathy is known as covert encephalopathy, and presents with subtle mental status changes such as sleep disturbance, mood changes, anxiety, fatigue [3]. Yet when these patients are subjected to psychometric testing, their performance is abnormal [1]. These patients may even have normal mental status, and the only evidence of impairment is performance on psychometric testing [10]. This tends to be more common in patients with cirrhosis rather than other forms of liver disease, characterizing up to 50% of patients with chronic liver disease [10, 11]. Typically, minimal encephalopathy seems to affect executive functions rather than speech and can therefore be difficult to assess. In pediatric patients, this may mean these patients have more academic difficulties, and poor school performance [3]. Furthermore, biomarkers do not correlate with psychometric testing results.
Management of Hepatic Encephalopathy
When evaluating a patient for HE, it is important to exclude other conditions that can present in a similar fashion. These conditions include but are not limited to respiratory failure, electrolyte derangements, status epilepticus, renal failure, stroke, hypoglycemia, central nervous system infections, metabolic acidosis and drug intoxication. Patients may also require evaluation of underlying liver disease, and workup should include a comprehensive metabolic panel with liver enzymes, complete blood count to assess for pancytopenia and thrombocytopenia, and coagulation panel with specific notation of international normalized ratio (INR) as described in Table 2. Further workup for the underlying etiology of liver disease is also important, and patients should be evaluated with autoimmune, infectious, and metabolic testing. Urine toxicology screening is needed to determine whether medication or drug effect is contributing to symptom presentation, and finally, a serum ammonia level to determine presence of hyperammonemia. Again, it is important to note that hyperammonemia does not correlate with the degree of clinical HE. Furthermore, collection of serum samples for ammonia level is very sensitive to technical variations and affects the results. This diagnostic approach is summarized in Table 2.
Overall, HE is a clinical diagnosis, and it can be difficult to clarify with concomitant concern for intensive care unit delirium. Imaging may be considered to exclude a cerebral mass or hemorrhage as confounding variables, and to evaluate for evidence of increased intracranial pressure (ICP) or cerebral herniation. Both magnetic resonance imaging (MRI) brain and computed tomography (CT) brain scans can be considered depending on the clinical context [1]. Furthermore, given the subtle but potentially progressive presentation of HE, close monitoring of the patient by bedside nursing, vigilant family/caregivers, and subsequent early intervention of the provider team if needed, is imperative. As such, these patients are best cared for in experienced liver transplant centers that are familiar with the signs and symptoms of HE, and understand this phase of disease can fluctuate, and have nuanced presentation as indicated in Table 1.
Treatment of HE largely depends on the underlying cause of liver disease. Mainstay of therapy tends to be supportive care, but there are medications to mitigate hyperammonemia as well (Table 3). Lactulose, a disaccharide which acidifies the intestinal lumen, is the most commonly used medication, and limits generation and absorption of gut ammonia. Lactulose stimulates passage of stool to eliminate ammonium converted by gut bacteria from ammonia [2, 10]. One study showed improvement in psychometric testing results in patients with minimal hepatic encephalopathy after treatment with lactulose [12]. Rifaximin may also be used, as this is a minimally absorbed broad-spectrum antibiotic that is solubilized by bile salts present in the small bowel to decrease ammonia production. Typically, lactulose is considered first-line therapy given its shorter time to onset than rifaximin [2, 4]. Other options for short-term treatment include empiric antibiotic therapy such as neomycin, metronidazole or oral vancomycin which all aim to alter the gut microbiome to reduce ammonia levels [2, 3, 10].
In the event of acute-onset progressive encephalopathy, patients should be closely monitored given the risk of increased ICP and cerebral edema. Management includes minimizing stimulation, elevating the head of the bed to 30 degrees, and prevention of further injury with the consideration of padded bed rails or a patient sitter. If the HE leads to cerebral edema, management of the associated increased ICP is indicated, and may include hyperventilation and hyperosmolar therapy with mannitol or hypertonic saline [4].
Dietary protein restriction is highly controversial in children of growing age, though intake of 1-2 g/kg/d has been suggested for patients with HE associated with acute liver failure and hyperammonemia, urea cycle defects, or chronic liver disease and acute onset HE in an effort to mitigate further ammonia production as a component of nitrogenous waste during protein catabolism [4, 10, 13, 14]. All sedative medications should be avoided, unless necessary for airway protective measures, especially benzodiazepines and opiate medications, which may alter the neurological exam further [3, 4]. Finally, extracorporeal liver support modalities may be required. Continuous renal replacement therapy (CRRT) treats HE by reducing hyperammonemia without inducing rapid fluid shifts, and removes water-soluble toxins [15]. Initiation of CRRT at Children’s Hospital Los Angeles (CHLA) is reserved for patients in liver failure with progressive encephalopathy grade 2 or higher, concerns for pulmonary edema, and hepatorenal syndrome that is unresponsive to medical management (Table 4). CRRT may also be considered for patients with hyperammonemia >100 μmol/L, or patients with renal failure and oliguria. It is important to note that recurrent HE in the setting of liver failure is an indication for liver transplantation.
Prevention of HE in patients with chronic liver disease relies on limiting underlying disease progression. Further attempts may include avoiding hepatotoxic medications and reducing gastrointestinal bleeding risks in patients with known esophageal varices through endoscopic approach when possible [5].
Newer Modalities of Investigation
Psychometric testing is limited in pediatrics and has mostly been validated in adult studies. Adapting adult assessments to children is difficult due to the variety of developmental achievements of children depending on their ages [3]. However, when appropriate, neuropsychiatric testing may be used to objectively measure severity of HE, especially in patients with chronic liver disease who are monitored in an outpatient setting [10].
In children with acute liver failure, EEG has been considered as a metric for monitoring degree of encephalopathy [16]. Patients who demonstrated moderate EEG changes (slowing and epileptiform discharges) were found to be more likely to require liver transplantation or die. In the same study, patients with low grade encephalopathy, <2, with normal or mild changes on EEG were more likely to recover without requirement of liver transplant [16].
New studies have attempted to identify neurobiomarkers that correlate more accurately with progression of encephalopathy than ammonia. One group which focused on patients with acute liver failure, noted that SB100β (an astrocyte marker) and IL-6, are present in higher amounts in patients with hepatic encephalopathy, which may highlight an inflammatory and immunologic component to hepatic encephalopathy [17]. Similarly, in patients with minimal HE and chronic liver disease, levels of IL-6 and TNF-α have been showed to be elevated [11].
Conclusions
In summary, HE, which is a clinically-diagnosed phenomena associated with worsening liver failure (acute, chronic, or acute-on-chronic), can be an indicator of poor prognosis. HE is often initially managed conservatively with supportive care. When it progresses, a variety of interventions may be useful and range from medication to dietary changes to extracorporeal liver support systems. Yet HE may also present with subtle mental status changes and is often initially missed in the pediatric population. In some cases, patients with HE in the setting of chronic liver disease may only be identified with psychometric testing. Knowing this, it is imperative to manage children with liver failure in an experienced liver transplant center equipped with the appropriate treatment modalities to intervene when necessary, given the unpredictable and potentially progressive nature of HE.
References
Prakash R, Mullen K. Hepatic encephalopathy. In: Schiff E, Maddrey W, Sorrell M, editors. Schiff’s Diseases of the Liver. 11th ed. Chichester: Wiley-Blackwell; 2012. p. 421–38.
Vilstrup H, Amodio P, Bajaj J, et al. Hepatic encephalopathy in chronic liver disease: Practice guideline by the american association for the study of liver diseases and the European Association for the study of the liver. Hepatology. 2014;60:715–35.
Pinto RB, Schneider ACR, da Silveira TR. Cirrhosis in children and adolescents: An overview. World J Hepatol. 2015;7:392–405.
Squires JE, Alonso EM, Ibrahim SH, et al. North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition position paper on the diagnosis and management of pediatric acute liver failure. J Pediatr Gastroenterol Nutr. 2022;74:138–58.
Dara N, Sayyari A-A, Imanzadeh F. Hepatic encephalopathy: Early diagnosis in pediatric patients with cirrhosis. Iran J child Neurol. 2014;8:1–11.
Ng VL, Li R, Loomes KM, Leonis MA, et al. Outcomes of children with and without hepatic encephalopathy from the pediatric acute liver failure study group. J Pediatr Gastroenterol Nutr. 2016;63:357–64.
Banc-Husu AM, Neighbors K, Rychlik K, Mohammad S, Harris ZL, Alonso EM. Admission characteristics identify risk of pediatric acute-on-chronic liver failure. J Pediatr Gastroenterol Nutr. 2020;70:783–8.
D’Souza R, Grammatikopoulos T, Pradhan A, et al. Acute-on-chronic liver failure in children with biliary atresia awaiting liver transplantation. Pediatr Transplant. 2019;23:e13339.
Singh H, Kelgeri C, Passingham C, et al. Acute-on-chronic liver failure: A 20-year retrospective review of a tertiary paediatric liver centre. Acta Paediatr. 2022;111:1435–40.
Blei AT, Córdoba J. Practice parameters committee of the American College of Gastroenterology. Hepatic encephalopathy. Am J Gastroenterol. 2001;96:1968–76.
Srivastava A, Chaturvedi S, Gupta RK, et al. Minimal hepatic encephalopathy in children with chronic liver disease: Prevalence, pathogenesis and magnetic resonance-based diagnosis. J Hepatol. 2017;66:528–36.
El-Karaksy HM, Afifi O, Bakry A, Kader AA, Saber N. A pilot study using lactulose in management of minimal hepatic encephalopathy in children with extrahepatic portal vein obstruction. World J Pediatr. 2017;13:70–5.
Nguyen DL, Morgan T. Protein restriction in hepatic encephalopathy is appropriate for selected patients: A point of view. Hepatol Int. 2014;8:447–51.
Yang CH, Perumpail BJ, Yoo ER, Ahmed A, Kerner JA. Nutritional needs and support for children with chronic liver disease. Nutrients. 2017;9:1127.
Zoica BS, Deep A. Extracorporeal renal and liver support in pediatric acute liver failure. Pediatr Nephrol. 2021;36:1119–28.
Hussain E, Grimason M, Goldstein J, et al. EEG abnormalities are associated with increased risk of transplant or poor outcome in children with acute liver failure. J Pediatr Gastroenterol Nutr. 2014;58:449–56.
Toney NA, Bell MJ, Belle SH, et al. Hepatic encephalopathy in children with acute liver failure: Utility of serum neuromarkers. J Pediatr Gastroenterol Nutr. 2019;69:108–15.
Funding
Open access funding provided by SCELC, Statewide California Electronic Library Consortium.
Author information
Authors and Affiliations
Contributions
JAB performed literature review, writing of manuscript and figure creation; RK performed manuscript writing and editing. RK will act as the guarantor for this manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bartlett, J.A., Kohli, R. Hepatic Encephalopathy in Children. Indian J Pediatr 91, 280–285 (2024). https://doi.org/10.1007/s12098-023-04679-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12098-023-04679-6