
Abstract
Childhood pneumonia is still a significant clinical and public health problem. India contributes the highest number of deaths due to pneumonia, accounts for about 20% of global mortality among under five children. Various etiologic agents including bacteria, viruses and atypical organism are responsible for childhood pneumonia. Recent studies suggest that viruses are one of the major causes of childhood pneumonia. Among viruses, respiratory syncytial virus has got great attention and several recent studies are reporting it as an important organism for pneumonia. Lack of exclusive breast feeding during first six months, improper timing of start and content of complimentary feeding, anemia, undernutrition, indoor pollution due to tobacco smoking and use of coal and wood for cooking food and lack of vaccinations are important risk factors. X-ray chest is not routinely performed to diagnose pneumonia while use of lung ultrasound is increasing to detect consolidation, pleural effusion, pneumothorax and pulmonary edema (interstitial syndrome). Role of C-reactive protein (CRP) and procalcitonin is similar, to differentiate between viral and bacterial pneumonia, however duration of antibiotics is better guided by procalcitonin. Newer biomarkers like IL-6, presepsin and triggering receptor expressed on myeloid cells 1 are needed to be evaluated for their use in children. Hypoxia is significantly associated with childhood pneumonia. Therefore, use of pulse oximetry should be encouraged for early detection and prompt treatment of hypoxia to prevent adverse outcomes. Among the available tools for risk of mortality assessment in children due to pneumonia, PREPARE score is the best but external validation will be needed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Childhood pneumonia is still a significant clinical and public health problem. No other childhood ailment comes close to its impact on the lives of children, community, and the healthcare system. India contributes the highest number of deaths due to pneumonia, which accounts for about 20% of global mortality among under five children [1]. Pneumonia is infective inflammation of lung parenchyma due to various pathogenic organisms including bacteria, viruses, fungi and parasites. The key symptom to suspect childhood pneumonia is tachypnea. The World Health Organization (WHO) has defined tachypnea as respiratory rate >60 per min for infants less than 2 mo, >50 per min for infants between 2 -12 mo and >40 per min for children 13 to 59 mo of age [2]. WHO has categorised pneumonia in children under-five years of age into two categories, pneumonia and severe pneumonia. Tachypnea with or without chest retraction is categorised as pneumonia while tachypnea with any danger signs (unable to feed or drink, hypothermia, unconsciousness, convulsion, signs of hypoxia including cyanosis, grunting, groaning, head nodding) as severe pneumonia [2].
In India, childhood pneumonia contributes 14% of under-five mortality and current mortality rate is 33 per 1,000 live births [3]. Resource-poor nations, where the prevalence of childhood pneumonia is approximately 15 times higher than in resource-rich countries, bear a disproportionate share of the worldwide burden [4]. The United Nations’ Organisation’s sustainable development goal (SDG) aims at reduction in under-five mortality to ≤25 per 1,000 live births by 2030 [5].
Epidemiology
Burden
The incidence of pneumonia, in under-five children of India, is not precisely known. There is a lot of variation in its reported incidence among various studies because of different definitions, diagnostic modalities and regional variations. In small-scale studies, the disease burden, measured in terms of episodes per child per year, ranged from 0.03 to 0.52 [6, 7]. In India, annually, 3.6 to 4.0 million episodes of childhood pneumonia are being reported along with 0.35 to 0.37 million deaths attributed to it [4, 8]. Pneumonia was responsible for 22.5% of total deaths among 1 to 4 y old children as shown by the RHIME study conducted in the year 2001-03 [9], while the Million Death Study showed 27.6% contribution of pneumonia in total under-five mortality in India for the year 2005 [8]. Among under-five children, case fatality rate for pneumonia ranged from 2.5% to 11.8% [10, 11]. As age increased, the incidence of severe pneumonia requiring hospitalisation considerably decreased [7, 10]. At global level mortality is equal among boys and girls while in India, mortality is 1.2 times higher in girls [1, 8].
Etiology
Various etiologic agents including bacteria, viruses and atypical organisms are responsible for childhood pneumonia. Identification of possible etiological organism of childhood pneumonia can be done by culture of the organism. Limited availability, poor yield of blood culture and time involved to get it reported are the main limiting factors for its utilisation. The reported yield of blood culture ranged between 2% to 27% in Indian studies [11, 12]. In recent years, polymerase chain reaction (PCR) has gained a lot of attention for etiologic evaluation of pneumonia on various specimens as it has high sensitivity as well specificity. The PCR is a quick and accurate approach for detecting bacteria, even atypical ones, and viruses, but it has a high initial equipment and training cost. Since lung aspirates are found to be sterile in healthy children, culture and PCR evaluation of lung aspirate could give a greater yield of the etiological agent and can be specific. However, lung aspiration is an invasive procedure and associated with serious side-effects including pneumothorax, or pulmonary hemorrhage. Therefore, it is rarely performed in pneumonia. Culture and PCR of the nasopharyngeal aspirate (NPA) has higher yield and therefore it can be utilised for possible etiologic evaluation of childhood pneumonia but the NPA reflects the organism present in nasopharynx and does not necessarily reflect the causative organism of pneumonia [13]. Using blood or NPA samples, multiplex PCR platforms have been evaluated to distinguish between viral and bacterial etiology and can identify more than one organism at the same time. Additionally, the PCR approach has been used to attempt serotyping of some microorganisms, such as Streptococcus pneumoniae [14, 15].
In order to diagnose Mycoplasma and Chlamydia infections, immune tests of serum for the presence of certain antibodies have also been utilised. This is because culture of these pathogens requires live tissue as a growth medium. However, the interpretation of seropositivity is complicated as antibodies develop 2 to 3 wk after primary infection and remain elevated for 2 to 6 mo [16].
Attempts have been made to identify etiological agent of pneumonia by detecting bacterial antigen in the urine [17]. However, due to kit to kit heterogeneity in detection rates, urine tests for antigens of specific bacteria like Streptococcus pneumoniae and Haemophilus influenzae have not been widely accepted.
There were many Indian studies in the 1990s and early 2000s suggesting Streptococcus pneumoniae being as the most common bacterial etiology (30 to 50%) followed by Haemophilus influenzae type B (HiB) [4, 11-13]. Various serotypes of Streptococcus pneumoniae are isolated form Indian children. Serotypes 1 and 5 were most prevalent followed by 4, 6A and 6B, 7, 12, 14, 15, 19F, 23 and 45 [18, 19]. However, recent studies are suggesting the increasing prevalence of Staphylococcus aureus [18]. Other organisms had also been reported like Acinetobacter in 20% and Klebsiella pneumoniae 3.3%- 20.5% [11, 12].
Global Burden of Disease 2015 Lower Respiratory Infection Collaborative Study revealed that deaths due bacterial pneumonia, Streptococcus pneumoniae and HiB together contribute 64.1% in under-five children [1]. Globally, attribution of HiB pneumonia in under-five mortality decreased by 38.6% but in India Hib is still responsible for 14.9% under-five deaths due to pneumonia [1]. The conjugate pneumococcal vaccine was introduced in India in a phased manner in 2017. There was a dip in vaccine coverage during the COVID pandemic. Hence, the impact of introduction of conjugate pneumococcal vaccination on reduction in under-five mortality is yet to be assessed.
Multi-country studies such as Pneumonia Etiology Research for Child Health (PERCH) study and Global Approach to Biological Research, Infectious diseases and Epidemics in Low-income countries (GABRIEL) have reported more than one microorganism, often combination of bacteria and virus, isolated using molecular techniques from the blood in children with pneumonia [14, 15]. Recent publications have reported that viruses are common etiological agents for pneumonia in developing countries, contrary to earlier belief that majority were caused by bacteria only [20]. It has also been postulated that viral respiratory tract infections open the gateway for secondary bacterial infections [21]. The focus of current international research has already changed from Pneumococcus to respiratory syncytial virus (RSV) as the proportionate contribution of viral diseases like RSV is predicted to rise with the launch and expansion of vaccinations against the primary causes of bacterial pneumonia (Pneumococcus and Haemophilus influenzae type B). Researches to develop vaccines and immunoglobulins against RSV are going on. The global data of various studies are suggesting increasing incidence and prevalence of RSV as important etiology of childhood pneumonia. Possible reason for these may be
-
I.
True increase in the incidence and prevalence of RSV pneumonia.
-
II.
Increased availability of diagnostic modalities of viral isolation (Multiplex PCR and culture).
-
III.
With increased coverage of vaccination against Haemophilus influenzae type B and Pneumococcus pneumoniae, prevalence and incidence of these organisms are decreasing continuously. This may have led to increase in viral pneumonia.
A recent systematic review by Shi et al. reported for the year 2015, 33.1 million episodes of RSV acute lower respiratory tract infections (ALRTI) occurred in under-five children globally and 10% (3.2 million) of these required hospitalisation, of which 59,600 died in the hospital [22]. Hospitalization as well as deaths were highest in infants below 6 mo of age across all regions. More than 93% of RSV ALRI episodes and 99% of related deaths occurred in developing countries [1, 22].
Among the under-five children, RSV is associated with around 28% of all ALRTI episodes and 10 to 22% of all ALRTI related deaths [1, 14, 22]. Approximately 10% of the global burden of RSV ALRTI occurs in developed countries, and rest 90% occurs in developing countries [1, 22]. About 20% of all RSV LRTI have lower chest indrawing (LCI) while among hospitalised, 85% have LCI. Among hospitalised under-five children due to RSV ALRTI, almost 20% showed hypoxemia, which increased the risk of death. It has been reported that RSV subtype A was the most common subtype and resulted in more severe disease and deaths.
The same group of investigators updated the review for 2019 and published their findings very recently in 2022, which reported almost similar number episodes of RSV ALRTI in under-five children occurred globally (33 million) and almost similar proportion of more than 10% (3.6 million) of these required hospitalisation but there was lower deaths (26,300) among hospitalised children [20]. Thus, overall prevalence of hospitalisations increased marginally while deaths are decreased by more than half of the previous time period, possibly due to better health care. Various Indian studies published from 1991 till the 2022 have reported a rise from 14% to 40.1% isolation/detection of RSV (Supplementary Table S1).
Risk Factors
See supplementary file.
Clinical Features
See supplementary file.
Diagnosis
Pneumonia in children is primarily diagnosed clinically. A peripheral blood smear typically reveals leucocytosis with neutrophilic predominance. It is not always necessary to diagnose childhood pneumonia using a chest X-ray. When there is an uncertainty about the diagnosis, persistent symptoms, or there is suspicion of complications such as pleural effusion or pneumothorax, an X-ray of the chest may be necessary [23]. Since there is large inter as well as intra observer variation in the interpretation of X-ray chest, WHO categorised its abnormalities seen in childhood pneumonia into pleural effusion, end point consolidation, and non-end point infiltrates to reduce intra and inter observer variation [24]. The ability of an X-ray chest to distinguish between bacterial and viral pneumonia is generally poor [23]. However, the WHO states that end point consolidation and pleural effusion radiological findings are likely caused by bacterial etiology [24].
There is growing evidence that lung ultrasound (LUS) has potential to replace the X-ray chest not only at the point of care but also in routine use [25, 26]. LUS has high sensitivity and specificity for detecting consolidation (96% and 93%) and pneumothorax (88% and 100%) [27].
Biomarkers
While pneumonia can be of bacterial or viral etiology, only 5% of bacterial pneumonia are bacteremic and can be termed as “pyogenic” pneumonia. Hence there is a diagnostic dilemma in differentiating viral from bacterial pneumonia which has led to investigating the role of various biomarkers for this purpose.
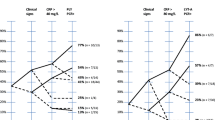
C-reactive protein (CRP) and procalcitonin (PCT) are the most widely used biomarkers in pneumonia. Interleukin 6 (IL-6) and presepsin has also been subjected to research works. PCT is a prohormone of calcitonin. Soon, after bacterial infection, the CALC-1 gene is upregulated which stimulates macrophage and monocytes to produce large amounts of PCT [28]. Due to its cytokine like behavior, rise of PCT is immediate and detected within 2–3 h, with a peak at 6 h [28]. The limitation though is that diagnostic and predictive value of PCT declines in severe sepsis and in localized infections, such as empyema [29]. Studies differ as to what are the appropriate cut-off points for PCT [29]. A PCT level of 0.25 ng/ml has 90% sensitivity and only 25% specificity, whereas value of 20 ng/ml has 90% specificity and 30% sensitivity for pyogenic pneumonia in a systematic review [30].
In response to cytokines, especially IL-6, produced at the infection site, CRP synthesis is quickly increased in the liver. Thus, in comparison to fever and leukocytosis, CRP is a superior biomarker for pyogenic infection but its secretion begins relatively late, in 4–6 h, and peaks at 36–50 h, and therefore it cannot be used for early detection of pyogenic pneumonia [31]. A CRP level of >30 mg/L has 90% sensitivity but <25% specificity and a cut-off of >300 mg/L has 90% specificity but only about 30% sensitivity for pyogenic pneumonia [30]. To distinguish between bacterial and viral, both CRP and PCT are similar but for detection of severity, prognostication and guidance on use of antibiotics, PCT is better than CRP [32, 33]. Instead of using a fixed cut-off level of PCT, decrease from initial levels could be used to determine when to stop using antibiotics altogether or to gradually reduce their use [33].
IL-6 has also been investigated as a biomarker for pneumonia. IL-6 levels rise faster than PCT and CRP after infection [29]. IL-6 is a more sensitive biomarker of localized infection such as effusions and empyema than PCT [29]. IL-6 has shown to have a utility as predictor of treatment failure and mortality [34]. Elevated IL-6 predicts a higher risk of 30-d mortality (84% sensitivity and 87% specificity) and IL-6 levels have a good correlation with various clinical severity scores such as pneumonia severity index in adults but further studies are required in children [34]. There are certain limitations to use IL-6 as a biomarker of pyogenic pneumonia. It has very short half-life and decreases rapidly even before clinical presentation [35]. It also lacks specificity as it increases in non-inflammatory conditions including connective tissue disorders and malignancies [36].
Presepsin, a fragment of monocyte lipopolysaccharide receptor CD14, is released in the blood during phagocytosis of bacteria. High levels of presepsin predict progression to septic shock and severe pneumonia [37]. It can be used with other biomarkers like PCT to increase the diagnostic and prognostic precision [37].
Triggering receptor expressed on myeloid cells 1 (TREM-1), a glycoprotein member of the immunoglobin family, is upregulated in the presence of extracellular bacteria and fungi [38]. Normally, TREM-1 is not detectable in healthy individuals, however, it becomes measurable in response to infection [38]. Further studies are needed to establish the diagnostic power of TREM-1 in pneumonia.
Despite research on biomarkers in pneumonia, prognosis is related to individual characteristics, and thus an area under the domain of precision or personalized medicine. This is the area of future work. It includes measures such as early clinical stability, inflammatory response and the response to antibiotics, the host’s genetic and metabolic characteristics, susceptibility to various organisms especially those causing infection, and the saprophytic flora colonizing the lower airways.
Management
The best methods to lower child mortality from pneumonia are early detection, rational use of antibiotics and appropriate supportive care. Oral antibiotics are recommended to treat non-severe pneumonia at home, but close monitoring for appearance of danger signs at any time and/or non-resolution of symptoms after 48 h of treatment and prompt and appropriate referral, and follow-up are essential. A recent Cochrane review concluded that oral cotrimoxazole and amoxicillin had comparable treatment failure (OR 0.92, 95% CI 0.58-1.47), cure rate (OR 1.12, 95% CI 0.61-2.03) and mortality (OR 2.08, 95% CI 0.22-20.06) in non-severe pneumonia [39]. Similar findings are also reported in another study conducted in 2008 [40]. The same review also reported that cotrimoxazole vs. procaine penicillin and co-amoxiclav vs. amoxicillin were comparable in terms of cure rate, hospitalisation and mortality in non-severe pneumonia [39]. In severe pneumonia, chloramphenicol showed greater treatment failure (OR 1.46, 95% CI 01.04-2.06 on day 10) and higher mortality (OR 1.65, 95% CI 0.99-2.77) in comparison to ampicillin plus gentamicin. WHO has recommended oral amoxicillin at a dose of 80 mg/kg/d for five days to treat non-severe pneumonia in under-five children as first-line treatment [2]. Children with severe pneumonia should be treated by injectable ampicillin at a dose of 50 mg/kg or benzyl penicillin at a dose of 50,000 units/kg IV or IM six hourly for a minimum duration of five days. Third generation cephalosporin (e.g., ceftriaxone) should be used as second-line of treatment in severe pneumonia if first-line antibiotics have failed.
Hypoxia is an important determinant of mortality and needs to be identified early and managed on priority. A recent study done by Awasthi et al. reported 35.9% of 7196 under-five children hospitalised with WHO defined severe pneumonia had hypoxia among those unvaccinated with PCV13 [41]. Oxygen saturation <90% on pulse oximetry or requiring oxygen therapy during hospital stay was considered as hypoxic. Adjusted odds ratio for mortality with hypoxia was 2.36 (95% CI: 1.42–3.92). The PERCH study conducted in seven countries reported prevalence of hypoxia as 35.8% in under-five children hospitalised with WHO defined severe and very severe pneumonia [14]. Hypoxia was more prevalent (42.3%, 748/1,769) among children with abnormal X-ray chest. Pulse oximetry must be used for early diagnosis of hypoxia because clinical signs and symptoms have low diagnostic accuracy for predicting it [42]. Pulse oximetry has demonstrated encouraging outcomes in the early diagnosis and subsequent treatment of hypoxemia, which reduce mortality due to pneumonia [43]. In situations where pulse oximetry is not possible, certain clinical signs of respiratory distress/failure (nasal flaring, grunting, and head nodding, lower chest indrawing, and central cyanosis) can be used as indicators for hospitalization and as predictors of hypoxia as well as mortality due to it [44]. Additionally, in cases of severe and very severe pneumonia, the WHO advises oxygen therapy when pulse oximetry is not possible and SpO2 less than 90% at room air.
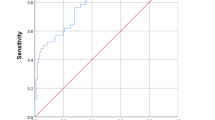
A risk assessment to predict childhood pneumonia related mortality is urgently required for triage and treatment/referral. There are numerous risk assessment tools, but only one, the Respiratory Index of Severity in Children-Malawi (RISC-Malawi) score, has shown fair discriminatory value (AUC 0.75, 95% CI 0.74-0.77), while the Respiratory Index of Severity in Children (RISC) score and a modified Pneumonia Etiology Research for Child Health (PERCH) score have limited discriminatory value in identifying hospitalised children at risk of pneumonia related mortality (AUC 0.66, 95% CI 0.58 to 0.73%, and AUC 0.55, 95% CI 0.37 to 0.73, respectively) [45].
The risk assessment instrument developed by the Pneumonia Research Partnership to Assess WHO Recommendations (PREPARE) is relatively new and offers excellent discriminatory power for identifying children at risk of pneumonia-related in-hospital mortality [46]. The data from 11 studies, including pneumonia evaluations in children in 20 low and middle-income countries, were used in the PREPARE study. The analysis involved a total of 27,388 children with mean age 14.0 mo and pneumonia-related case fatality ratio 3.1%. This tool has 200 repetitions to internal validation. Age, sex, weight-for-age Z-score, body temperature, respiratory rate, unconsciousness or diminished state of consciousness, convulsions, cyanosis, and hypoxemia were baseline variables in the PREPARE risk assessment tool. When internally tested, the PREPARE risk assessment tool exhibited a good discriminating value (area under the curve: 0.83, 95% CI: 0.81 to 0.84). The PREPARE tool is therefore the best risk assessment tool currently available for under-five childhood pneumonia. External validation of PREPARE tool is needed.
The Government of India's Ministry of Health and Family Welfare recently started its Social Awareness and Action Plan to Neutralise Pneumonia successfully (SAANS) in 2019 with the goal of stepping up efforts to reduce pneumonia-related mortality to less than 3 per 1000 live births by 2025 [47]. The remote health facilities must be equipped to manage both outdoor and indoor pneumonia which includes (i) having dispersible amoxicillin tablets for outdoor management, (ii) having injectable antibiotics, pulse oximeter and oxygen for better indoor management, (iii) having standard management protocols available at every facility, and (iv) setting up a SAANS booth at the facility's entrance to provide counselling and messaging for childhood pneumonia [47].
Conclusions
Even though there has been a reduction in the global incidence and corresponding mortality due to pneumonia in children under-five years of age, yet concentrated efforts are required at global and country levels, health systems strengthening and operations, implementation as well as basic research aimed at surveillance for etiology of pneumonia, vaccine development and identifying point of care tests, perhaps by using novel biomarkers with clinical signs, to differentiate viral from bacterial pneumonia to ensure rational use of antibiotics and prevent development of antimicrobial resistance. In addition, improved nutritional status through appropriate feeding practices, immunization coverage, environmental and hand hygiene etc. will have to be augmented along with improved case management algorithms and health systems preparedness to fight pneumonia.
References
GBD 2015 LRI Collaborators. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory tract infections in 195 countries: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Infect Dis. 2017;17:1133–61.
Revised WHO classification and treatment of childhood pneumonia at health facilities. Evidence Summaries, Word Health Oranization. 2014. Available at: http://apps.who.int/iris/bitstream/10665/137319/1/9789241507813_eng.pdf. Accessed on 18 Sept 2022.
Wahl B, Knoll MD, Shet A, et al. National, regional and state level pneumonia and severe pneumonia morbidity in children in India: Modelled estimates for 2000 and 2015. Lancet Child Adolesc Health. 2020;4:678–87.
Rudan I, O’Brien K, Nair H, et al; Child Health Epidemiology Reference Group (CHERG). Epidemiology and etiology of childhood pneumonia in 2010: Estimates of incidence, severe morbidity, mortality, underlying risk factors and causative pathogens for 192 countries. J Glob Health. 2013;3:010401.
United Nation’s Organisation (UNO). Sustainable Development Goals (SDG), 2015. Available at: http://www.un.org/sustainabledevelopment/health/. Accessed on 27 Sept 2022.
National Family Health Survey-5, 2019-21. India Fact Sheet. Available at: http://rchiips.org/nfhs/NFHS-5_FCTS/India.pdf. Accessed on 30 Sept 2022.
Gupta M, Kumar R, Deb AK, et al. Multi-center surveillance for pneumonia & meningitis among children (<2 yr) for Hib vaccine probe trial preparation in India. Indian J Med Res. 2010;131:649–58.
Bassani DG, Kumar R, Awasthi S, et al. The Million Death Study Collaborators: Causes of neonatal and child mortality in India: A nationally representative mortality survey. Lancet. 2010;376:1853–60.
Registrar General of India. Report on causes of death in India 2001-2003. Sample registration system. New Delhi: RGI, Ministry of Home Affairs; 2009. p. 19–27.
Ramachandran P, Nedunchelian K, Vengatesan A, Suresh S. Risk factors for mortality in community acquired pneumonia among children aged 1–59 months admitted in a referral hospital. Indian Pediatr. 2012;49:889–95.
Tiewsoh K, Lodha R, Pandey RM, Broor S, Kalaivani M, Kabra SK. Factors determining the outcome of children hospitalized with severe pneumonia. BMC Pediatr. 2009;9:15.
Mathew JL, Singhi S, Ray P, et al. Etiology of community acquired pneumonia among children in India: Prospective, cohort study. J Glob Health. 2015;5:050418.
Pandey A, Chaudhry R, Nisar N, Kabra SK. Acute respiratory tract infections in Indian children with special reference to Mycoplasma pneumoniae. J Trop Pediatr. 2000;46:371–4.
Levine OS, O’Brien KL, Deloria-Knoll M, et al. The Pneumonia Etiology Research For Child Health (PERCH) project: A 21st century childhood pneumonia etiology study. Clin Infect Dis. 2012;54:S93–101.
Picot VS, Bénet T, Messaoudi M, et al; Pneumonia GABRIEL Network. Multicenter case–control study protocol of pneumonia etiology in children: Global approach to biological research, infectious diseases and epidemics in low-income countries (GABRIEL network). BMC Infect Dis. 2014;14:635.
Kuo CC, Jackson LA, Campbell LA, Grayston JT. Chlamydia pneumoniae (TWAR). Clin Microbiol Rev. 1995;8:451–61.
Hyams C, Williams OM, Williams P. Urinary antigen testing for pneumococcal pneumonia: Is there evidence to make its use uncommon in clinical practice? ERJ Open Res. 2020;6:00223–2019.
Nisarga, R, Premalatha, R, Shivananda, et al. Hospital-based surveillance of invasive pneumococcal disease and pneumonia in south Bangalore, India. Indian Pediatr. 2015,52:205–11.
Balaji V, Jayaraman R, Verghese VP, Baliga PR, Kurien T. Pneumococcal serotypes associated with invasive disease in under five children in India & implications for vaccine policy. Indian J Med Res. 2015;142:286–92.
Li Y, Wang X, Blau DM, et al. Respiratory Virus Global Epidemiology Network, Nair H; RESCEU investigators. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: A systematic analysis. Lancet. 2022;399:2047–64
Hendaus MA, Jomha FA, Alhammadi AH. Virus-induced secondary bacterial infection: A concise review. Ther Clin Risk Manag. 2015;11:1265–71.
Shi T, McAllister DA, O'Brien KL, et al; RSV Global Epidemiology Network. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: A systematic review and modelling study. Lancet. 2017;390:946–58.
Harris M, Clark J, Coote N, et al. British Thoracic Society guidelines for the management of community acquired pneumonia in children: Update 2011. Thorax. 2011;66:ii1–23.
Standardization of interpretation of chest radiographs for the diagnosis of pneumonia in children. Geneva: WHO. 2001. Available at: http://apps.who.int/iris/bitstream/10665/66956/1/WHO_V_and_B_01.35.pdf. Accessed on 13 Sept 2022.
Yadav KK, Awasthi S, Parihar A. Lung ultrasound is comparable with chest roentgenogram for diagnosis of community-acquired pneumonia in hospitalised children. Indian J Pediatr. 2017;84:499–504.
Bhalla D, Naranje P, Jana M, Bhalla AS. Pediatric lung ultrasonography: Current perspectives. Pediatr Radiol. 2022;52:2038–50.
Biswas A, Lascano JE, Mehta HJ, Faruqi I. The utility of the “Shred sign” in the diagnosis of acute respiratory distress syndrome resulting from multifocal pneumonia. Am J Respir Crit Care Med. 2017;195:e20–2.
Prucha M, Bellingan G, Zazula R. Sepsis biomarkers. Clin Chim Acta. 2015;440:97–103.
Meisner M. Update on procalcitonin measurements. Ann Lab Med. 2014;34:263–73.
Dudognon D, Levy C, Chalumeau M, et al. Pneumonia Study Group. Diagnostic accuracy of routinely available biomarkers to predict bacteremia in children with community-acquired pneumonia: A secondary analysis of the GPIP/ACTIV pneumonia study in France, 2009-2018. Front Pediatr. 2021;9:684628.
Povoa P. C-reactive protein: A valuable marker of sepsis. Intensive Care Med. 2002;28:235–43.
Yadav KK, Awasthi S, Takia L, Agarwal J, Agarwal GG. Procalcitonin and C reactive protein in WHO defined severe and very severe community acquired pneumonia: A hospital based cross sectional study. Clin Epidemiol Glob Health. 2015;3:S3–9.
de Jong, E van Oers, JA, Beishuizen A, et al. Efficacy and safety of procalcitonin guidance in reducing the duration of antibiotic treatment in critically ill patients: A randomised, controlled, open-label trial. Lancet Infect. Dis. 2016;16:819–27.
Andrijevic I, Matijasevic J, Andrijevic L, Kovacevic T, Zaric B. Interleukin-6 and procalcitonin as biomarkers in mortality prediction of hospitalized patients with community acquired pneumonia. Ann Thorac Med. 2014;9:162–7.
Morley D, Torres A, Cillóniz C, Martin-Loeches I. Predictors of treatment failure and clinical stability in patients with community acquired pneumonia. Ann Transl Med. 2017;5:443.
Kishimoto T. IL-6: From its discovery to clinical applications. Int Immunol. 2010;22:347–52.
Klouche K, Cristol JP, Devin J, et al. Diagnostic and prognostic value of soluble CD14 subtype (Presepsin) for sepsis and community-acquired pneumonia in ICU patients. Ann Intensive Care. 2016;6:59.
Salluh JIF, Souza-Dantas VC, Póvoa P. The current status of biomarkers for the diagnosis of nosocomial pneumonias. Curr Opin Crit Care. 2017;23:391–7.
Kabra SK, Lodha R, Pandey RM. Antibiotics for community-acquired pneumonia in children. Cochrane Database Syst Rev. 2010;23:CD004874.
Awasthi S, Agarwal G, Singh JV, et al; ICMR-IndiaClen Pneumonia Project Group. Effectiveness of 3-day amoxycillin vs. 5-day co-trimoxazole in the treatment of non-severe pneumonia in children aged 2-59 months of age: A multi-centric open labeled trial. J Trop Pediatr. 2008;54:382–9.
Awasthi S, Rastogi T, Pandey AK, et al. Epidemiology of hypoxic community-acquired pneumonia in children under 5 years of age: an observational study in northern India. Front Pediatr. 2022;9:790109.
Lodha R, Bhadauria PS, Kuttikat AV, et al. Can clinical symptoms or signs accurately predict hypoxemia in children with acute lower respiratory tract infections? Indian Pediatr. 2004;41:129–35.
Duke T, Subhi R, Peel D, Frey B. Pulse oximetry: technology to reduce child mortality in developing countries. Ann Tropic Paediatr. 2009;29:165–75.
Nascimento-Carvalho CM. Community-acquired pneumonia among children: The latest evidence for an updated management. J Pediatr (Rio J). 2020;96:29–38.
Rees CA, Hooli S, King C, et al; World Health Organization PREPARE Study Group. External validation of the RISC, RISC-Malawi, and PERCH clinical prediction rules to identify risk of death in children hospitalized with pneumonia. J Glob Health. 2021;11:04062.
Rees CA, Colbourn T, Hooli S, et al; World Health Organization PREPARE Study Group. Derivation and validation of a novel risk assessment tool to identify children aged 2–59 months at risk of hospitalised pneumonia- related mortality in 20 countries. BMJ Global Health. 2022;7:e008143.
SAANS 2019: Campaign Guidance Note. Social awareness and action plan to neutralise pneumonia successfully. MOHFW, GOI. Available at: https://nhm.gov.in/New_Updates_2018/SAANS/Saans_Campaign_Guidance_Note.zip. Accessed on 7 Oct 2022.
Author information
Authors and Affiliations
Contributions
Both authors equally contributed in the writing of the manuscript. SA will act as the guarantor for this manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Yadav, K.K., Awasthi, S. Childhood Pneumonia: What’s Unchanged, and What’s New?. Indian J Pediatr 90, 693–699 (2023). https://doi.org/10.1007/s12098-023-04628-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12098-023-04628-3