
Abstract
Objectives
To describe the diagnostic test properties of Cardiac Troponin-T (cTnT) in predicting myocardial dysfunction in asphyxiated term neonates by taking echocardiography as the gold standard and to establish the optimum cut-off values of cTnT for myocardial dysfunction, shock, severe hypoxic ischemic encephalopathy (HIE) and mortality by receiver operator characteristic (ROC) curve analysis.
Methods
This was a prospective study based on diagnostic test evaluation. The study included 120 term asphyxiated neonates in a tertiary care neonatal intensive care unit (NICU) in Southern India from June 2011 through June 2015. All the neonates were clinically evaluated. Venous blood was taken at 4 h of life for cTnT estimation. Echocardiography was done within 24 h of birth.
Results
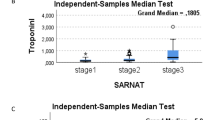
The mean cTnT level of asphyxiated term neonates was 0.207±0.289 ng/ml (mean ± SD). Asphyxiated neonates with myocardial dysfunction had higher cTnT levels (0.277±0.231) as compared to those without myocardial dysfunction (0.061±0.036, p = 0.0001). Using ROC curve, the cut-off cTnT values for myocardial dysfunction was 0.1145 ng/ml with sensitivity 92.4% and specificity 94.1%. Cardiac Troponin-T levels were significantly higher among asphyxiated neonates with shock (0.378±0.348, p = 0.0001) and the levels also correlated positively with increasing grades of HIE. The cut-off cTnT value for mortality was 0.2505 ng/ml with sensitivity 83.9% and specificity 96.6%.
Conclusions
In asphyxiated term neonates, early cTnT elevation is a marker for predicting myocardial dysfunction and elevated cTnT levels had high sensitivity and specificity. There was significant relation with increasing cTnT values and increasing grades of HIE.






Similar content being viewed by others


References
Lawn JE, Cousins S, Zupan J; Lancet Neonatal Survival Steering Team. 4 million neonatal deaths: when? where? why? Lancet. 2005;365:891–900.
Tapia-Rombo CA, Carpio-Hernández JC, Salazar-Acuña AH, et al. Detection of transitory myocardial ischemia secondary to perinatal asphyxia. Arch Med Res. 2000;31:377–83.
Rajkumar PS, Bhat BV, Sridhar MG, et al. Cardiac enzyme levels in myocardial dysfunction in newborns with perinatal asphyxia. Indian J Pediatr. 2008;75:1223–5.
Vijlbrief DC, Benders MJ, Kemperman H, van Bel F, de Vries WB. Use of cardiac biomarkers in neonatology. Pediatr Res. 2012;72:337–43.
Güneś T, Oztürk MA, Köklü SM, Narin N, Köklü E. Troponin –T levels in perinatally asphyxiated neonates during the first 15 days of life. Acta Pediatr. 2005;94:1638–43.
Moller JC, Thidson B, Schaible TF. Value of myocardial hypoxic markers and serum creatinine for retrospective diagnosis of perinatal asphyxia. Biol Neonate. 1998;73:367–74.
Agarwal J, Shah GS, Paudel P, Baral N, Agrawal A, Mishra OP. Electrocardiographic and enzymatic correlations with outcome in neonates with hypoxic–ischemic encephalopathy. Ital J Pediatr. 2012;38:33.
EL Khuffash AF, Molloy CT. Serum Troponin in neonatal intensive care. Neonatology. 2008;94:1–7.
Clark SJ, Newland P, Yoxall CW, Subhedar NV. Concentrations of cardiac troponin T in neonates with and without respiratory distress. Arch Dis Child Fetal Neonatal Ed. 2004;89:348–52.
Omokhodion SI, Losekoot TG, Jaiyesimi F. Serum creatine kinase and creatine kinase MB isoenzyme activities in perinatally asphyxiated newborns. Eur Heart J. 1991;12:980–4.
Mandal Ravi RN, Gupta R, Kapoor AK. Evaluation of activity of creatine phosphokinase (CPK) and its isoenzyme CPK-MB in perinatal asphyxia and its implications for myocardial involvement. Bull NNF. 1999;13:2–7.
Clark SJ, Newland P, Yoxall CW, Subhedar NV. Cardiac troponin T in cord blood. Arch Dis Child Fetal Neonatal Ed. 2001;84:F34–7.
Lopes DN, Ramos JMM, Moreira MEL, Cabral JA, de Carvalho M, Lopes JM. Cardiac troponin T and illness severity in very low birth weight infant. Int J Pediatr. 2012;2012:479242.
Goel M, Gohiya P, Yadav BS. Assessment of myocardial function in birth asphyxia. Int J Med Res Rev. 2013;1:228–32.
Mertens L, Seri I, Marek J, et al. Targeted neonatal echocardiography in the neonatal intensive care unit: practice guidelines and recommendations for training. J Am Soc Echocardiogr. 2011;24:1057–78.
Szymankiewicz M, Matuszczak-Wleklak M, Hodgman JE, Gadzinowski J. Usefulness of cardiac troponin- T and echocardiography in the diagnosis of hypoxic myocardial injury of full term neonates. Biol Neonate. 2005;88:19–23.
Costa S, Zecca E, De Rosa G, et al. Is serum troponin-T a useful marker of myocardial damage in newborn infants with perinatal asphyxia? Acta Paediatr. 2007;96:181–4.
Awada H, Ai Tannir M, Ziade, et al. Cardiac troponin T: useful early marker for cardiac and respiratory dysfunction in neonates. Neonatology. 2007;92:105–10.
Trevisanuto D, Zaninott M, Altiniers S, et al. High serum cardiac troponin T concentrations in preterm infants with respiratory distress syndrome. Acta Paediatr. 2000;89:1134–6.
Boo NY, Hafidz H, Nawaui HM, et al. Comparison of serum cardiac troponin T and creatine kinase MB isoenzyme concentration in asphyxiated term infants during the first 48 hrs of life. J Paediatr Child Health. 2005;41:331–7.
Kanik E, Ozer EA, Bakibi AR, et al. Assessment of myocardial dysfunction in neonates with hypoxic ischemic encephalopathy: is it a significant predictor of mortality? J Matern Fetal Neonatal Med. 2009;22:239–42.
Simovic AM, Prijic SM, Knezevic JB, Igrutinovic ZR, Vujic AJ, Kosutic JLJ. Predictive value of biochemical, echocardiographic and electrocardiographic markers in non–surviving and surviving asphyxiated full term neonates. Turk J Pediatr. 2014;56:243–9.
Matter M, Abdel-Hady H, Attia G, Hafez M, Seliem W, Al-Arman M. Myocardial performance in asphyxiated full term infants assessed by Doppler tissue imaging. Pediatr Cardiol. 2010;31:634–42.
Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarction redefined --a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol. 2000;36:959–69.
Gaze DC, Collinson PO. Cardiac troponin I should be interpreted with caution in pediatric neonatal patients. Concerning Turker et al: cord blood troponin I as an early predictor of short term outcome in perinatal hypoxia. Biol Neonate. 2005;87:19.
Bodor GS, Survant L, Voss EM, Smith S, Porterfield D, Apple FS. Cardiac troponin T composition in normal and regenerating human skeletal muscle. Clin Chem. 1997;43:476–84.
Sasse S, Brand NJ, Kyprianov P, et al. Troponin I gene expression during human cardiac development and in end – stage heart failure. Circ Res. 1993;72:932–8.
Adamcová M, Kokstein Z, Palicka V, Podholová M, Kostál M. Troponin T levels in the cord blood of healthy term neonates. Physiol Res. 1995;44:99–104.
Martín-Ancel A, García-Alix A, Gayá F, Cabañas F, Burgueros M, Quero J. Multiple organ involvement in perinatal asphyxia. J Pediatr. 1995;127:786–93.
Acknowledgements
Dr Saboora Beegum - Professor & HOD, Department of Biochemistry, Govt. Medical college, Thiruvananthapuram for her role in supervising the biochemical estimation of cTnT.Dr Muralidharan Nair – Asst. Prof. of Medical Statistics (Retd), CERTC, Govt. Medical College, Thiruvananthapuram for his help in the statistical analysis.
Author information
Authors and Affiliations
Contributions
SJ: Designed the study, collected & analysed the data, did the literature work, wrote the paper; SL and ZAM: Conducted the echocardiographic analysis; SK: Permitted to do the study in NICU, critically reviewed the manuscript and approved the final version. SK will act as guarantor for this paper.
Corresponding author
Ethics declarations
Conflict of Interest
None.
Source of Funding
State Board of Medical Research (SBMR), Govt. of Kerala.
Rights and permissions
About this article

Cite this article
Joseph, S., Kumar, S., Ahamed M, Z. et al. Cardiac Troponin-T as a Marker of Myocardial Dysfunction in Term Neonates with Perinatal Asphyxia. Indian J Pediatr 85, 877–884 (2018). https://doi.org/10.1007/s12098-018-2667-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12098-018-2667-3