
Abstract
Purpose
The objective of this study is to describe the anatomic location of the sentinel lymph node (SLN) of patients with lung carcinoma and to analyze its relationship with the characteristics of the tumor.
Patients and methods
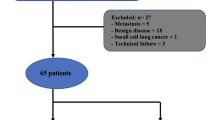
98 Stage I lung cancer patients were included in the study. SLN was marked just after performing the thoracotomy by injecting peritumorally 0.25 mCi of nanocolloid of albumin (Nanocol1) labeled with Tc-99 m in 0.3 ml, and later, it was resected. For SLN micrometastasis analysis, CEACAM5, BPIFA1, and CK7 gene expression at mRNA level was studied. Possible relation between tumor characteristics and SLN location was analyzed.
Results
While most of the SLN were located in hilar area, we find a significantly higher number of SLN located in mediastinal stations when the lesion is in the left upper lobe (LUL). This difference disappears in the group of SLN with a positive result in the micrometastasis study. Regarding tumor size, squamous tumors and tumors located in the left lower lobe (LLL) were found significantly larger.
Conclusion
The location of the SLN in patients with stage I lung cancer is predominantly hilar, being less consistent in the left hemithorax. The tumor size or histological type is not variables that affect this distribution. The distribution of SLNs with a positive result in the analysis of micrometastasis suggests further spread to the hilar areas when the lesion is in the LUL and to the mediastinal zones when it is in the LLL.


Similar content being viewed by others


References
Naruke T, Suemasu K, Ishikawa S. Lymph node mapping and curability at various of metastasis in resected lung cancer. J Thorac Cardiovasc Surg. 1978;76:832–9.
American Thoracic Society. Clinical staging of primary lung cancer: American Thoracic Society node mapping scheme. Am Rev Respir Dis. 1983;127:659–69.
Ou S-HI, Zell JA. Prognostic significance of the number of lymph nodes removed at lobectomy in stage IA non-small cell lung cancer. J Thorac Oncol. 2008;3:880–6.
Varlotto JM, Recht A, Nikolov M, Flickinger JC, de Camp MM. Extent of lymphadenectomy and outcome for patients with stage I non-small cell lung cancer. Cancer. 2009;115:851–8.
Whitson B, Groth S, Maddaus M. Surgical assessment and intraoperative management of mediastinal lymph nodes in non-small cell lung cancer. Ann Thorac Surg. 2007;84:1059–65.
Galbis J, Cremades A, Zuñiga A, Estors M, Tembl Ferrairó A, Martínez-Hernández N, et al. El ganglio centinela en el carcinoma pulmonar. Estudio molecular tras detección con radio isótopo. Cir Esp. 2014;92:1–3.
Benlloch S, Galbis JM, Alenda C, Peiró FM, Sánchez-Ronco M, Rodríguez-Paniagua JM, et al. Expression of molecular markers in mediastinal nodes from resected stage I non-small cell lung cancer (NSCLC): prognostic impact and potential role as markers of occult micrometastases. Ann Oncol. 2009;20:91–7.
Darling GE, Allen MS, Decker PA, Ballman K, Malthaner RA, Inculet RI, et al. Number of lymph nodes harvested from a mediastinal lymphadenectomy. Results of the Randomized, Prospective American College of Surgeons Oncology Group Z0030 Trial. Chest. 2011;139:1124–9.
Liptay M, Masters G, Winchester D, Eldelman BL, Garrido BJ, Hirschtritt TR, et al. Intraoperative radioisotope sentinel lymph node mapping in non-small cell lung cancer. Ann Thorac Surg. 2000;70:384–90.
Giroux DJ, Rami-Porta R, Chansky K, Crowley JJ, Groome PA, Postmus PE, et al. On behalf of the International Association for the Study of Lung Cancer International Staging Committee the IASLC lung cancer staging project. Data elements for the prospective project. J Thorac Oncol 2009;4:679–83.
Ignatius S, Zell J. Prognostic significance of the number of lymph nodes removed at lobectomy in stage IA non-small cell lung cancer. J Thorac Oncol. 2008;4:880–6.
Xu F, Qi L, Yue D, Wang Ch. The effect of the extent of lymph node dissection for stage IA non-small cell lung cancer on patients’ disease free survival. Clin Lung Cancer. 2013;14(2):181–7.
Nomori H, Kohno M, Izumi Y, Ohtsuka T, Asakura K. Sentinel nodes in lung cancer: review of our 10-year experience. Surg Today. 2011;41:889–95.
Little AG, de Hoyos A, Kirgan DM, Arcomno TR, Murray KD. Intraoperative lymphatic mapping for non-small cell lung cancer: the sentinel nodel technique. J Thorac Cardiovasc Surg. 1999;117:220–4.
Riquet M, Bagan P, Le Pimpec BF, Banu E, Scotte F, Foucault C, et al. Completely resected non-small cell lung cancer: reconsidering prognostic value and significance of N2 metastases. Ann Thorac Surg. 2007;84:1818–24.
Puma B. Isolated mediastinal skip metastasis in lung cancer: is it real N2 disease? J Thorac Cardiovasc Surg. 2005;129:235.
Misthos P, Sepsas E, Kokotsakis J, Skottis I, Lioulias A. The significance of one station N2 disease in the prognosis of patients with non-small cell lung cancer. Ann Thorac Surg. 2008;86:1626–31.
Benoit L, Anusca A, Ortega-Deballon P, Cheynel N, Bernard A, Favre JP. Analysis of risk factors for skip lymphatic metastasis and their prognostic value in operated N2 non- small-cell lung carcinoma. Eur J Surg Oncol. 2006;32:583–7.
Tomaszek SC, Kim Y, Cassivi SD, Jensen MR, Shen KH, Nichols FC, et al. Bronchial resection margin length and clinical outcome in non-small cell lung cancer. Eur J Cardiothorac Surg. 40(5):1151–6.
Maeda R, Yoshida J, Ishii G, Hishida T, Nishimura M, Nagai K. Risk factors for tumor recurrence in patients with early-stage (stage I and II) non-small cell lung cancer: Patient selection criteria for adjuvant chemotherapy according to the 7th edition TNM classification. Chest 2011;140(6):1494–502.
Karamustafaoglu YA, Yoruk Y, Yanik F, Sarikaya A. Sentinel lymph node mapping in patients with operable non-small cell lung cancer. J Thorac Dis. 2013;5(3):317–20.
Pulte D, Li E, Crawford BK, Newman E, Alexander A, Mustalish DC, et al. Sentinel lymph node mapping and molecular staging in nonsmall cell lung carcinoma. Cancer. 2005;104(7):1453–61.
Melfi FM, Lucchi M, Davinj F, Viti A, Fontanini G, Boldrini L, et al. Intraoperative sentinel lymph node mapping in stage I non-small cell lung cancer: detection of micrometastases by polymerase chain reaction. Eur J Cardiothorac Surg. 2008;34(1):181–6.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
None.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Galbis-Caravajal, J.M., Lafuente-Sanchis, A., Estors-Guerrero, M. et al. Topography of the sentinel node according to the affected lobe in lung cancer. Clin Transl Oncol 19, 858–864 (2017). https://doi.org/10.1007/s12094-017-1615-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12094-017-1615-4