
Abstract
Although the number of postoperative maxillary cyst (POMC) cases has declined recently, a few reports of refractory cases have also been reported. The indications for endoscopic sinus surgery (ESS) for POMC removal are broadening and attempts to prevent postoperative recurrence at the cyst opening site have been widely investigated. Here, we have advocated our original pedunculated mucoperiosteal flap (CLAP flap; covered lateral and posterior wall flap of the maxillary sinus), where the bony area exposed intraoperatively is covered, to prevent postoperative recurrence. We have also presented the method for creating the CLAP flap. We classified the POMC as being medial, lateral, or anterior superior type and performed ESS. We introduced the CLAP flap after 2015 for the lateral type and some of the medial types of POMCs. We examined the cyst opening rate using computed tomography, age, sex, cyst position, and a follow-up period in four patients (five sides) who did not undergo flap surgery, but who were managed in our hospital in 2015, and in eight patients (nine sides) who underwent the CLAP flap technique in our hospital. In the group with the CLAP flap, the cyst opening rate was significantly higher (P < 0.05). The CLAP flap was effective for preventing postoperative bony regrowth. It may be one of the options for covering the exposed bone surface as widely as possible.




Similar content being viewed by others


Data Availability
The datasets during and/or analysed during the current study available from the corresponding author on reasonable request.
References
Lee JY, Baek BJ, Byun JY, Shin JM (2014) Long-term efficacy of inferior meatal antrostomy for treatment of postoperative maxillary mucoceles. Am J Otolaryngol 35:727–730. https://doi.org/10.1016/j.amjoto.2014.07.008
Sawatsubashi M, Murakami D, Oda M, Komune S (2015) Transnasal endoscopic surgery of postoperative maxillary cysts. J Laryngol Otol 129:S46–S51. https://doi.org/10.1017/s0022215114002382
Durr ML, Goldberg AN (2014) Endoscopic partial medial maxillectomy with mucosal flap for maxillary sinus mucoceles. Am J Otolaryngol 35:115–119. https://doi.org/10.1016/j.amjoto.2013.10.010
Yanagi K, Ohtori N, Hukami M, Moriyama H (1992) Endoscopic endonasal surgery in postoperative maxillary cysts. Oto-Rhino-Laryngol 35:425–433 ([in Japanese])
Tochigi K, Omura K, Miyashita K, Aoki S, Otori N, Tanaka Y (2020) Pathological features of free graft and pedicled flap in the nasal cavity: an animal study. Laryngoscope 131:E428–E433. https://doi.org/10.1002/lary.28630
Kim HY, Dhong HJ, Min JY, Jung YG, Park SH, Chung SK (2009) Postoperative maxillary sinus mucocoele: risk factors for restenosis after surgery and preventive effects of mytomycin-C. Rhinol 47:79–84
Mohri M, Nishio M, Mohri J, Shimazu K, Akane K (1977) Problems relating to postoperative maxillary cyst. Nihon Jibiinkoka Gakkai Kaiho 80:326–333 (Article in Japanese)
Harvey RJ, Sheahan PO, Schlosser RJ (2009) Inferior turbinate pedicle flap for endoscopic skull base defect repair. Am J Rhinol Allergy 23:522–526. https://doi.org/10.2500/ajra.2009.23.3354
Hadad G, Bassagasteguy L, Carrau RL, Mataza JC, Kassam A, Snyderman CH, Mintz A (2006) A novel reconstructive technique after endoscopic expanded endonasal approaches: vascular pedicle nasoseptal flap. Laryngoscope 116:1882–1886. https://doi.org/10.1097/01.mlg.0000234933.37779.e4
Wu P, Li Z, Liu C, Ouyang J, Zhong S (2016) The posterior pedicled inferior turbinate-nasoseptal flap: a potential combined flap for skull base reconstruction. Surg Radiol Anat 38:187–194. https://doi.org/10.1007/s00276-015-1516-6
Acknowledgements
We would like to thank Editage (www.editage.com) for English language editing.
Funding
No funding was received for conducting this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose.
Ethical Approval
The study protocol was approved by the ethics committee of Dokkyo Medical University Saitama Medical Center (Authorization No. 1736).
Patient Consent
The requirement for the acquisition of informed consent from all participants in this study was waived due to this study's retrospective nature.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
The CLAP flap (covered lateral and posterior wall flap of the maxillary sinus) was used in combination with the inferior meatus lateral flap in all cases.
In both flaps, the pedicle is located behind the nasal cavity, with the sphenopalatine artery acting as the main feeding vessel. The cyst is located laterally, outside the infraorbital nerve.
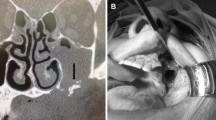
Left nostril: The cyst was released using the endoscopic modified medial maxillectomy approach. The bone surrounding the cyst opening was drilled until there was no overhang.
The mucosa on the lateral side of the inferior turbinate was incised with a slit knife, number 15 scalpel, and scissors, creating the CLAP flap with the dorsal side of the inferior turbinate as the base. The exposed bone was covered by overlaying the CLAP flap and the inferior meatus lateral flap. The nasal cavity configuration is not changed by suturing the inferior turbinate end.
Three months after surgery, computed tomography demonstrated that the cyst opening had good patency and no bony regrowth. The endoscopic findings at 3 months postoperatively showed that the cysts were firmly opened and the flaps were well engrafted.
Rights and permissions
About this article

Cite this article
Aoki, S., Omura, K., Miyashita, K. et al. A Covered Lateral and Posterior Wall Flap of the Maxillary Sinus Prevents Reocclusion of the Postoperative Maxillary Cyst. Indian J Otolaryngol Head Neck Surg 73, 504–509 (2021). https://doi.org/10.1007/s12070-021-02658-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12070-021-02658-x