
Abstract
Coronavirus causes damage to chemosensory receptors resulting in olfactory and gustatory dysfunction. This study reports our observations on anosmia and ageusia in symptomatic COVID-19 positive patients admitted in the COVID centre of Western Rajasthan. A total of 98 symptomatic, RT-PCR positive COVID-19 patients admitted in the M.G. Hospital during November 2020 were evaluated with detailed history regarding symptoms along with duration and resolution including response to antiviral therapy. Olfactory and Gustatory dysfunction was seen in 53.1% patients. Both anosmia and ageusia coexisted in 61.5% patients followed by isolated anosmia (25%), while isolated ageusia was rare. History of preceding fever was present in 69.2% cases. 100% of the patients with ageusia had loss of salty and sour taste, while 90.1% did not feel sweet taste. Bitter taste sensation was altered only in 63.6%. Symptoms reversed within 7 days in 94.2% cases and after 15 days in 5.8% cases irrespective of antiviral therapy. Chemosensory dysfunction has no racial predominance. It is a self-limiting manifestation and a useful screening symptom. Co-existence of anosmia and ageusia is more common than isolated dysfunction. In ageusia, salty and sour is the most commonly lost taste sensation followed by sweet.
Similar content being viewed by others


Introduction
The world is amidst a fast growing pandemic of Severe Acute Respiratory Syndrome Coronavirus- 2 (SARS-CoV-2) caused by novel coronavirus (2019-nCoV). The increasing case spikes, severity and mortality are encouraging medics, paramedics and scientists for extensive and rapid research. While we have gained a little knowledge, a lot about the disease is yet oblivious to the mankind. At the time of outbreak of COVID-19 in Wuhan, China reported symptoms like fatigue, fever, dry and productive cough, shortness of breath, chest compression, myalgia, diarrhea, nausea, vomiting, anorexia, headache, sore throat, dizziness, palpitations, chest pain, conjunctival congestion, nasal congestion, hemoptysis etc., [1,2,3]. Further researches and clinical experience revealed presence of anosmia and ageusia in many patients. Mao et al. analyzed the frequency of neurological manifestations in 214 patients with coronavirus disease 2019 (COVID-19), identifying anosmia in 11 (5.1%) patients and ageusia in 12 (5.6%) patients [4]. Following this, Vaira L A. et al. were amongst the first to report the high incidence of chemoreceptive disorder in COVID-19 patients during the initial days of its outbreak in Italy [5]. They substantiated their previous study with a subsequent objective clinical evaluation of olfactory and gustatory dysfunction in COVID-19 patients and found a prevalence of 73.6% [6]. It was observed that all these patients did not have associated symptoms of nasal blockage, rhinitis or chronic rhinosinusistis. Thus, we come to an understanding that there is direct damage to the olfactory and gustatory chemosensory receptors by coronavirus. This damage is probably to the non-neuronal support cells, which once infected, alter the function of neurons. The difference in the incidence of these symptoms in the Chinese and European study was attributed to the different concentration of these receptors in Asians and Caucasians [7]. Many other clinicians from different areas of the world have reported their experience on olfactory and gustatory dysfunction in symptomatic and pauci-symptomatic patients [8, 9].
This study aims to report our observations on olfactory and gustatory dysfunction in symptomatic COVID-19 positive patients from the second largest COVID Centre of Rajasthan.
Materials and Methods
The study was conducted in M.G.Hospital, which is a COVID dedicated hospital allied to Dr. S.N. Medical College, Jodhpur, Rajasthan, India. It included 98 symptomatic COVID-19 positive patients above the age of 18 years admitted in the inpatient department of Medicine in the month of November 2020. All the patients enrolled in the study were tested positive by Real-Time Polymerase Chain Reaction (RT-PCR) test on rhino-pharyngeal swab.
Study Design: Observational Study.
Study Duration: 1 month.
Study Location: Department of Medicine, M.G. Hospital (COVID Hospital), Dr. S.N. Medical College, Jodhpur, Rajasthan, India.
The study was conducted by Department of Oto-rhinolaryngology, Dr. S.N. Medical College, Jodhpur, Rajasthan, India.
Inclusion Criteria:
-
1.
All admitted symptomatic patients above the age of 18 years who tested positive for COVID-19 by RT-PCR test on rhino-pharyngeal swab.
Exclusion Criteria:
-
1.
Severely or Critically ill patients admitted in Intensive Care Unit.
-
2.
Patients who are known cases of Rhinitis or Rhinosinusitis.
-
3.
Cancer patients who had undergone Chemotherapy or Radiotherapy.
-
4.
Patients who has history to previous anosmia or ageusia.
Methodology
Data was collected by taking detailed history regarding age, gender, history of contact with positive patient or recent travel, presenting symptoms along with their duration and progression and response to antiviral therapy.
Observations and Results
The study included 98 symptomatic COVID-19 positive patients, who were admitted in the inpatient department of Medicine. Out of these, 50 were female patients and 48 males with a mean age of 41.4 years.

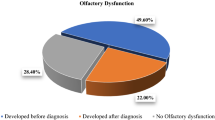
In our observation, 52 (53.1%) patients had olfactory and gustatory dysfunction while the remaining 46 (46.9%) did not have complaints pertaining to smell or taste.
Out of these 52 (53.1%) patients complaining of altered smell and taste, 13 (25%) had isolated anosmia, 7 (13.5%) had isolated ageusia and 32 (61.5%) complained of both.

And, 36 of these 52 patients (69.2%) had a history of preceding fever, following which they developed olfactory and gustatory dysfunction.

A total of 39 patients complained of ageusia, however, on careful and detailed questioning, it was observed that not all taste sensations were lost in every patient. 100% of the patients with ageusia had loss of salty and sour taste, while 90.1% did not feel sweet taste. Bitter taste sensation was altered only in 63.6%.
Almost all these patients, 49 of 52 (94.2%) showed reversal of olfactory and gustatory symptoms within 7 days and only in 3 (5.8%) the symptoms persisted over 15 days, irrespective of antiviral (Remdesivir or Favipiravir) drug therapy initiation.

Discussion
Chemosensory dysfunction is one of the common symptom observed in COVID infected cases and by now has been sufficiently reported by various authors from different countries. In mouse models, the SARS-CoV showed transneuronal penetration through the olfactory bulb and therefore, transneuronal spread of infection [10]. As seen in humans, these symptoms are mostly reversible. Human Angiotensin Converting Enzyme-2 (ACE-2) is found to be the functional receptor for binding and penetration of SARS-CoV-2 [11]. Brann et al. suggested that the virus targets the non-neuronal support cells of the olfactory nerves and these cells are rich in ACE-2 receptors [12]. This receptor is also widely expressed on the epithelial cells of oral mucosa [13]. Thus damage to mucosal epithelial cells may explain ageusia experienced by the patients. In March 2020, the American Academy of Otolaryngology-Head and Neck Surgery reported that anosmia and dysgeusia has been found in COVID-19 positive individuals and now recommends it to be added to the screening list for COVID-19 infection. There are discrepant observations among Asian and Caucasian population. Lee Y. et al. reported the prevalence and duration of acute loss of smell and taste in Korean population in April 2020. They concluded, acute anosmia or ageusia was observed in 15.3% (488/3,191) patients in the early stage of COVID-19 and in 15.7% (367/2,342) patients with asymptomatic-to-mild disease severity [8]. While a multicenter European study by Lechien J R. et al. reports 85.6% and 88.0% of patients with olfactory and gustatory dysfunctions, respectively [11]. The overall frequency of olfactory and gustatory dysfunction in our series is 86.5% and 75% respectively. This is close to the observations made by the European study. There by, defying the racial discrepancy that has been hypothesised.
Dysgeusia or Ageusia alone is a very rare presenting symptom. Klopfenstein et al. reported that anosmia and dysgeusia co-occurred 85% of the time [14]. Altin F. et al. observed that isolated anosmia was seen in 35.8% of infected cases in Germany, isolated dysgeusia was found in 1 case and co-occurence was seen in 24.69% cases [15]. In contradiction, Vaira L. et al. explained that there is no causal relationship between anosmia and ageusia and rather they experienced that gustatory impairment was in fact more common than olfactory changes [7]. A prospective case control study by Eduardo Martin-Sanz and his colleagues reported the incidence of isolated subjective hyposmia or hypogeusia was present in just 1.3% of our population [16]. In our study, we observed isolated ageusia only in 13.5% and isolated anosmia in 25% cases. But, they were observed simultaneously in 61.5% cases.
In our series, we tried to evaluate taste impairment individually for all four primary tastes and observed that sour and salty taste were affected in all the cases of ageusia followed by sweet which was lost in 90.1% cases while bitter taste sensation was least lost, only in 63.6% cases. A nearly similar finding was also reported by Vaira L. et al. as regards with the gustatory function, the most affected sensitivities were those for sweet (23 patients) and sour (21 patients), but there was no clear predominance of disturbances toward a primary taste in particular [6]. Further studies will be required to establish and testify these findings.
Vaira L. et al. reported spontaneous regression of chemosensory dysfunction in 66% cases in their subjective study [6]. Lechien J R. concluded that 25.5% of patients recovered both olfactory and gustatory functions throughout the 2 weeks after the resolution of general symptoms. And, they estimated that 56% of patients have persistent olfactory dysfunction over the days following the resolution of general symptoms [11]. In a much recent prospective case control study by Eduardo Martin-Sanz and his colleagues it was stated that in most cases, smell impairment is self-limiting. In their study, 85.4% of these patients recovered olfactory function within the first 14 days of the onset of the symptoms [16]. In our study, we saw resolution of chemosensory dysfunction in 100% cases, 94.2% showed reversal within 7 days of onset while 5.8% cases had persistent symptoms for over 15 days which could be due to a much direct insult by the virus. Permanent persistence of chemosensory dysfunction has not been reported so far.
Conclusion
SARS-CoV-2 is a new disease and our understanding about it is only growing. Through our study, we observed and defied the concept of racial predominance of olfactory and gustatory dysfunction in Caucasians over Asians. It was seen that probability of anosmia and ageusia co-existing is much higher as compared to isolated dysfunction. We also conclude that most commonly affected taste sensation is sour and salty followed by sweet and then least to be affected is bitter. Lastly, we conclude that chemosensory dysfunction is a self-limiting manifestation of COVID-19 infection but it can be a very useful screening symptom for the ENT specialists and must be kept in mind for differentials.
References
Yang X, Yu Y, Xu J, Shu H, Xia J, Liu H et al (2020) Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med 8(5):475–481
Guan W, Ni Z, Hu Y, Liang W, Ou C, He J et al (2020) Clinical Characteristics of coronavirus disease 2019 in China. N Engl J Med 382(18):1708–1720
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y et al (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan. China Lancet 395(10223):497–506
Mao L, Wang M, Chen S, He Q, Chang J, Hong C et al (2020) Neurological Manifestations of Hospitalized Patients with COVID-19 in Wuhan, China: a retrospective case series study
Vaira LA, Salzano G, Deiana G, De Riu G (2020) Anosmia and ageusia: common findings in COVID-19 patients. Laryngoscope 130(7):1787
Vaira LA, Deiana G, Fois AG, Pirina P, Madeddu G, De Vito A et al (2020) Objective evaluation of anosmia and ageusia in COVID-19 patients: Single-center experience on 72 cases. Head Neck 42(6):1252–1258
Vaira LA, Salzano G, Deiana G, De Riu G (2020) In response to anosmia and ageusia: common findings in COVID-19 patients. Laryngoscope 130(11):E695
Lee Y, Min P, Lee S, Kim SW (2020) Prevalence and duration of acute loss of smell or taste in COVID-19 patients. J Korean Med Sci 35(18):1–6
Mohamud MFY, Mohamed YG, Ali AM, Adam BA (2020) Loss of taste and smell are common clinical characteristics of patients with COVID-19 in somalia: a retrospective double centre study. Infect Drug Resist 13:2631–2635
Netland J, Meyerholz DK, Moore S, Cassell M, Perlman S (2008) Severe acute respiratory syndrome coronavirus infection causes neuronal death in the absence of encephalitis in mice transgenic for human ACE2. J Virol 82(15):7264–7275
Lechien JR, Chiesa-Estomba CM, De Siati DR, Horoi M, Le Bon SD, Rodriguez A et al (2020) Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): a multicenter European study. Eur Arch Oto-Rhino-Laryngology 277(8):2251–2261
Brann DH, Tsukahara T, Weinreb C, Lipovsek M, Van Den Berge K, Gong B et al (2020) Non-neuronal expression of SARS-CoV-2 entry genes in the olfactory system suggests mechanisms underlying COVID-19-associated anosmia. Sci Adv 6(31)
Xu H, Zhong L, Deng J, Peng J, Dan H, Zeng X et al (2020) High expression of ACE2 receptor of 2019-nCoV on the epithelial cells of oral mucosa. Int J Oral Sci 12(1)
Klopfenstein T, Kadiane-Oussou NJ, Toko L, Royer PY, Lepiller Q, Gendrin V et al (2020) Features of anosmia in COVID-19. Med Mal Infect 50(5):436–439
Altin F, Cingi C, Uzun T, Bal C (2020) Olfactory and gustatory abnormalities in COVID-19 cases. Eur Arch Oto-Rhino-Laryngol 277(10):2775–2781
Martin-Sanz E, Riestra J, Yebra L, Larran A, Mancino F, Yanes-Diaz J et al (2020) Prospective study in 355 patients with suspected COVID-19 infection: value of cough, subjective hyposmia, and hypogeusia. Laryngoscope 130(11):2674–2679
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the1964 Helsinki declaration and its later amendments or comparable ethical standards.
Consent for Publication
Informed consent was obtained from all individual participants included in the study.
Conflict of interest
Authors Semridhi Gupta, Payal Kumbhat and Manohar Seervi declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Gupta, S., Kumbhat, P. & Seervi, M. Olfactory and Gustatory Dysfunction in Covid-19: An Observational Study in a Tertiary Care Institute of Western Rajasthan. Indian J Otolaryngol Head Neck Surg 74 (Suppl 2), 2930–2934 (2022). https://doi.org/10.1007/s12070-021-02563-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12070-021-02563-3