
Abstract
Acute respiratory infections pose a constant threat to society and health care professionals. The effectiveness of face masks covering mouth and nose in reducing aerosol spread and curbing respiratory infection acquisition is well-studied. Despite enough beneficial evidence in favour of wearing masks, general population and the health care workers needs to be convinced to wear it and often enforcement is required for the same. This study was designed to study various barriers perceived and experienced with poor mask usage among hospital staff from an otorhinolaryngological perspective. An online survey was conducted to study the awareness of health care professionals and other hospital staff about advantages and disadvantages of mask use. Total 100 questionnaire based responses were obtained using this method. The participants included the ministerial staff, nursing and paramedical staff and faculty and residents of various medical and surgical specialties. The data thus collected was analyzed to identify the perceived benefits and limitations in mask usage. The participants wore surgical mask more commonly (50%) as compared to N95 respirator and cloth mask. 58% of the participants were using masks due to professional need. Majority (40%) used masks for a period ranging from 4 to 8 h in a day. Most of the participants realized that the masks offered protection from aerosols (90%) and more than 60% also mentioned that it helped in avoiding touching the face inadvertently. 62% participants complained of fogging of vision while wearing masks and approximately 50% reported pain due to tight elastic bands, difficulty breathing through mask and excessive sweating in the masked area In non-pharmaceutical measures to contain the aerosol-associated pandemics, face masks play an important precautionary role. It is cheap, easy to use and protects against respiratory infections, pollution and allergies. Certain minor issues like fogging of spectacles, and difficulty breathing through mask may need revisions in mask fabric and design.
Similar content being viewed by others


Introduction
Use of surgical face mask to protect patients from surgical wound infection is almost a century old [1]. Its use also protects the operating personnel from contamination, while taking care of patients with blood borne infections, by protection against splashes or sprays of body fluids [1]. Acute upper respiratory tract infection is a very common illness and using face mask limits droplet transmission, thus controlling respiratory infections [2]. Well fitted face mask interrupts the movement of expelled droplets with airborne viruses from cough or sneeze, so these do not contaminate work space or enter in respiratory tract of person nearby [3]. The use of mask not only prevents inhalation of respiratory pathogens but also reduces hand to nose contact transmission, besides protection from airborne particulates and allergens. The transmission is reduced when both the infected person and the contact wear mask, but the compliance in latter is often poor [4].
The regular use of mask may cause respiratory discomfort and inconvenience that may hinder its usage even among the health care professionals at high risk of contracting the disease. Even the mask itself may harbor microbes if not changed at regular intervals and may cause other health problems.Thus, various determinants, issues and barriers associated with mask-wearing compliance need to be highlighted and uncovered. Keeping in mind various pros and cons associated with mask usage, this survey was conducted among the hospital staff to receive their feedback of using mask during recent COVID-19 (Coronavirus disease) pandemic. We are aware that COVID-19 is a highly contagious and serious illness that currently has no recommended treatment or vaccine and is spreadingin susceptible population worldwide. Realizing this, there is little to lose and potentiallysomething to gain from this precautionary measure, provided it is worn appropriately and consistently.
Materials and Methods
The computer assisted self-administered questionnaire was prepared by a team of otorhinolaryngologists and physician. The questionnaire had 12 close-ended questions with multiple choice options and also one open option. The Institutional Ethical approval was obtained for same. After obtaining informed consent, total 100 health care professionals of different categories working in a tertiary referral centre with COVID facility were asked to take this anonymous survey online. The responses were collected, compiled and analyzed.
Results
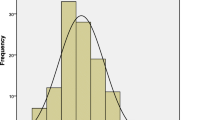
In our survey total of 100 participants (n = 100), there was preponderance of the middle-aged professionals as majority of our participants were between 25 and 54 y of age (Fig. 1) 0.58% of the participants were male and 42% were females. 89% of the participants were living in urban and 11% lived in rural areas respectively. Among our study participants, 32% were doctors from various fields, 52% were health care workers including nurses, paramedical workers, sanitation workers other than doctors and 16% were departmental administrative staff (Fig. 2).

Percentage of participants from different age groups

Percentage of participants according to their profession
72% of our patients were married and 21% were un-married and 7% were married but not living together. 60 individuals in married group were compliant with wearing masks, while only 5 in unmarried were using mask regularly. 68% of our participants were post graduates, 20% were qualified graduates and 12% were undergraduates.
The type of mask usage differed among the various participants. 17% used N95 respirator mask, 50% participants used surgical mask, while 23% used mask prepared from cotton cloth.Among all the participants risk of aerosol was high in 25%, moderate in 38% and low in 37% of the surveyed populationrespectively.
In the study, 58% of the participants used the mask due to professional need, 33% used due to self-awareness, 6% on the advice of doctors and 3% under pressure from government or administrative authorities. The duration of face mask use differed among the participants. Majority (40%) of the people used it for 4–8 h per day, 28% for less than 4 h, 26% between 8–12 h and 5% and 1% for 12–16 h and more than 16 h respectively.
Among the benefits of using mask by the participants (Fig. 3), 90% perceived that it reduced aerosol and droplet transmission. 67% expressed that it reduced the habit of touching face. 64% conveyed that it offered protection from air pollution and dust. 58% replied that it provided a sense of protection against infection. 45% reported reduced exposure to blood and body fluids during various surgeries. 33% reported reduction in nasal allergies and sneezing. 21% reported that it reduced nasal crusting and habit of nose picking. 21% reported that it reduced the habit of spitting in public. 15% reported reduced habit of smoking and tobacco use.13%, 9%, 8%, 7% reported reduced tendency to nail biting, reduced incidence of nasal bleeding, recurrent tonsillitis, nasal myiasis infection respectively.

Benefits of using mask as listed by participants
Among the various side effects mentioned by the participants (Fig. 4), 62% indicated fogging of spectacles which hindered their vision.56% expressed that mask was very uncomfortable due to the pain caused by elastic bands. 55% reported suffocation and difficult and heavy breathing, especially while climbing stairs. 49% reported excessive sweating inside the masked area of the face. 44% expressed reduced quality and volume of speech. 43% conveyed development of skin marks and scarring due to pressure. 40% reported pain and redness due to friction. 28% revealed a false sense of securitywhile wearing the mask. 19% reported significant ear discomfort due to constant pull from mask.17% were concerned about the increased expenditure on purchasing masks due to shortage in hospital supply.16% pointed out increased incidence of furunculosis on face.14% manifested increased incidence of eyes irritation and claustrophobia. 4% indicated increased sense of embarrassment due to use of face mask. 3% reported ill-fitting of mask due to beard and moustache. Most these issues forced the participants to keep on readjusting, touching and removing the mask temporarily.

Drawbacks of using mask, as listed by participants
Discussion
The respiratory infections associated morbidity and mortality may be reduced significantly by cheap and non-invasive non-pharmaceutical interventions like frequent hand washing, respiratory etiquettes (during sneeze or cough) and use of facemask [2]. According to a study, the compliance with face mask use was lowest in comparison with other two methods of curbing spread of disease, i.e. vaccination and isolationused to contain influenza pandemic [5]. Nevertheless, during outbreaks, perceived susceptibility and perceived severity often overrides the effect of perceived barriers with regard to facemask use among health care professionals and frontline staff. Still, it is essential to know the factors responsible for poor or irregular mask usage, which when taken care of, may increase the adherence and acceptability.
Healthcare workers in general are more compliant with mask usage than general population. However, there is lack of awareness among hospital staff on which type of mask should be worn in the hospital as can be observed from our study. This was clarified in a study that assessed the filtration efficiency of common household material like cotton T-shirt, scarf, tea towel, pillow case, surgical mask, cotton mix, linen, silk etc. [6]. Cloth mask are cheap, easily available, washable, reusable, while surgical masks are costly as they are made up of multiple layers of synthetic microfiber and are single use/disposable. The authors found surgical mask to be three times more effective than routine cloth mask in terms of protection from virus transmission, thus concluding to stop cloth mask use by health care workers. Among the surgical masks also, mask with ties behind straps provided better fit sealwhile the mask with looped elastic straps to be worn on ear was easier to use [6].
In another study, the older participants were more willing to wear facemasks in comparison to younger people [5, 7]. This is explained by the increased risk-taking behaviors of the younger health care workers. There was similarlyan increased adherence of mask usage in married people as compared to unmarried ones [5, 7]. This is because married are anxious about the health of their spouse and children and feel a sense of responsibility and conscious awareness towards their family’s safety [8]. The same was confirmed by our survey.
The survey conducted among traditional market workers and shoppers in Taiwan, revealed that people with higher education are more likely to adorn facemasks [9]. Illiteracy and unawareness lead to poor sense of perceived susceptibility and severity of disease; while it is otherwise for highly educated individuals [8]. In several studies, women were found to be more compliant of using facemasks in public, compared to men [10]. Though, in our survey both genders were equally compliant for regular mask usage. The literature shows that location of residence plays a role in mask usage. The people in rural areas were more compliant, in comparison to urban [5]. As majority of our survey participants were from urban area, there was no significant difference between two groups.
According to an observational study, exhalation during normal breathing produces predominantly aerosol i.e. particle size < 5 µm as compared to sneezing and coughing, which produces droplets [11]. Thus, virus in aerosol remain suspended in indoor environment for hours and likely to inhaled or disseminated by air currents, while droplets settle down, reducing time window of droplets having mucosal deposition. Another study on population-wide use of mask concluded that mask not only helps in containing influenza pandemic, but also reduces virus infection attack rate, by reducing transmission in healthy individuals and reducing infectiousness of carriers [12].
The regular use of mask in areas with fine particulate matter with an aerodynamic diameter < 2.5 µm (PM2.5) and levels greater than World Health Organization air quality guidelines (< 10 µg/m3), is recommended to avoid respiratory and cardiovascular illness [13]. These originate from burning of fossil fuels like coal in power plants and petrol, diesel combustion in vehicles and more troublesome during winter months, in the form of smog.
The surgical mask and N95 respirator mask (N denote non-oil, meaning mask filters out non-oil-based particles and number denotes the percentage blocked) can effectively block transmission of severe acute respiratory syndrome (SARS) causing viruses by 68% and 91% respectively [14]. Thus, surgical masks are of limited value when used in high or moderate risk environment. The absence of tight fit in surgical mask as compared to N95 respirator may be responsible for inward leak. The tight fit is provided by elastic bands, clip over nose and form fitted on sides. With these benefits, still the N95 respirator is not recommended for general public, due to high cost and limited supply, thus reserved for healthcare workers, immune-compromised persons and attendants of the patients [15]. Reuse of these masks may reduce cost, wastage and also protect the environment. But this requires thorough disinfection, which carries risk of damaging the blocking structure of these masks.
In a study on barriers to mask usage, it was found to cause discomfort by sliding repeatedly due to low cheekbones and small nose bridges as in children and became damp, more so in warm conditions [16]. Another study revealed, poor compliance for wearing mask due to social embarrassment and being considered a dangerous person by others [17]. The long beard may prevent good fitting of mask, thus exposing to contaminated air.
The N95 respirator mask without valve may increase the end tidal CO2 and fractional concentration of inspired CO2, reducing oxygen delivered to tissues [18]. The wearer has to work harder to inhale, suffering suffocation and respiratory trouble in return. Further, the moisture gets build up in N95 respirator mask without valve, especially in high humidity atmosphere, thus reducing filtration efficiency and become a harbor for bacteria to thrive [19]. The N95 respirator mask with a one-way smart valve enhances the comfort to the wearer, by improving the flow of exhaled gas out of the mask, while inhaled air must pass through filter material [20]. But, using mask with smart valve has one drawback of passing the pathogen in unfiltered exhaled air, thus not providing protection to other patients or health care workers.
The study in detail of various disadvantages listed by our participants revealed fogging on spectacles, pain at elastic site and difficulty breathing to be complained by more than 50%. While sweating, ear pull, cost or social embarrassments were minor issues. This may be explained, as majority were health care workers (68%), with free supply of mask in their facility and usage was professional need, so less embarrassment. These issues can be resolved by research on the development of ideal mask having the optimum fabric, thickness, outer water repellent layer and best adjustable fit. Masks which are comfortable yet effective are likely to be worn consistently and effectively.
The government and media play important role in educating population regarding their immune susceptibility and promoting anti-contagion measures including appropriate use of mask to prevent disease transmission and contain this pandemic [8]. The health care workers oughtto educate and motivate their patients of proper mask-wearing and hand hygiene techniques and bring about positive behavior change by setting an example themselves. Mask wearing has to be the new norm. The availability of attractive, easy to wear and comfortable mask may further increase their potential usage. Moreover, universal use of mask will actively involve every citizen and may provide sense of social solidarity in response to the national response to the pandemic [21].
Conclusion
In conclusion, it is prudent to make efforts to decrease perceived barriers and to increase perceived benefits, thereby improving the essentiality of wearing the facemask appropriately and regularly. Considering various pros and cons associated with different variety of masks, the N95 respirator mask should be used by moderate and high risk population like health care workers actively handling COVID cases, aerosol-generating procedures, the laboratory staff responsible for processing of the swab sample and those in first contact with the patient. The 3-layered surgical mask is useful for mild risk personnel. The cloth mask is cheap, accessible and more convenient for population in general. Healthcare policy makers, mass media and educational institutions can make concerted campaigning to ensure social distancing and high mask-wearing compliance among all categories of citizens to substantially curb the spread of airborne infections.
References
Tunevall TG (1991) Postoperative wound infections and surgical face masks: a controlled study. World J Surg 15(3):383–388. https://doi.org/10.1007/BF01658736
Furuya H (2007) Risk of transmission of airborne infection during train commute based on mathematical model. Environ Health Prev Med 12(2):78–83. https://doi.org/10.1007/BF02898153
Tang JW, Liebner TJ, Craven BA, Settles GS (2009) A schlieren optical study of the human cough with and without wearing masks for aerosol infection control. J R Soc Interface 6(Suppl 6):S727–S736. https://doi.org/10.1098/rsif.2009.0295.focus
MacIntyre CR, Cauchemez S, Dwyer DE et al (2009) Face mask use and control of respiratory virus transmission in households. Emerg Infect Dis 15(2):233–241. https://doi.org/10.3201/eid1502.081167
Taylor M, Raphael B, Barr M, Agho K, Stevens G, Jorm L (2009) Public health measures during an anticipated influenza pandemic: factors influencing willingness to comply. Risk Manag Healthc Policy 2:9–20. https://doi.org/10.2147/RMHP.S4810
Davies A, Thompson KA, Giri K, Kafatos G, Walker J, Bennett A (2013) Testing the efficacy of homemade masks: would they protect in an influenza pandemic? Disaster Med Pub Health Prep 7(4):413–418. https://doi.org/10.1017/dmp.2013.43
Tang CS, Wong CY (2004) Factors influencing the wearing of facemasks to prevent the severe acute respiratory syndrome among adult Chinese in Hong Kong. Prev Med 39(6):1187–1193. https://doi.org/10.1016/j.ypmed.2004.04.032
Sim SW, Moey KS, Tan NC (2014) The use of facemasks to prevent respiratory infection: a literature review in the context of the Health Belief Model. Singapore Med J 55(3):160–167. https://doi.org/10.11622/smedj.2014037
Kuo PC, Huang JH, Liu MD (2011) Avian influenza risk perception and preventive behavior among traditional market workers and shoppers in Taiwan: practical implications for prevention. PLoS ONE 6(9):e24157. https://doi.org/10.1371/journal.pone.0024157
Lau JT, Griffiths S, Choi KC, Lin C (2010) Prevalence of preventive behaviors and associated factors during early phase of the H1N1 influenza epidemic. Am J Infect Control 38(5):374–380. https://doi.org/10.1016/j.ajic.2010.03.002
Fabian P, McDevitt JJ, DeHaan WH et al (2008) Influenza virus in human exhaled breath: an observational study. PLoS ONE 3(7):e2691. https://doi.org/10.1371/journal.pone.0002691
Brienen NC, Timen A, Wallinga J, van Steenbergen JE, Teunis PF (2010) The effect of mask use on the spread of influenza during a pandemic. Risk Anal 30(8):1210–1218. https://doi.org/10.1111/j.1539-6924.2010.01428.x
Brook RD, Newby DE, Rajagopalan S (2017) The global threat of outdoor ambient air pollution to cardiovascular health: time for intervention. JAMA Cardiol 2(4):353–354. https://doi.org/10.1001/jamacardio.2017.0032
Jefferson T, Del Mar C, Dooley L et al (2009) Physical interventions to interrupt or reduce the spread of respiratory viruses: systematic review. BMJ 339:b3675. https://doi.org/10.1136/bmj.b3675
Xiao J, Shiu EYC, Gao H et al (2020) Nonpharmaceutical measures for pandemic influenza in nonhealthcare settings-personal protective and environmental measures. Emerg Infect Dis 26(5):967–975. https://doi.org/10.3201/eid2605.190994
Ferng YH, Wong-McLoughlin J, Barrett A, Currie L, Larson E (2011) Barriers to mask wearing for influenza-like illnesses among urban Hispanic households. Public Health Nurs 28(1):13–23. https://doi.org/10.1111/j.1525-1446.2010.00918.x
Seale H, Mak JP, Razee H, MacIntyre CR (2012) Examining the knowledge, attitudes and practices of domestic and international university students towards seasonal and pandemic influenza. BMC Public Health 12:307. https://doi.org/10.1186/1471-2458-12-307
Birgersson E, Tang EH, Lee WL, Sak KJ (2015) Reduction of carbon dioxide in filtering facepiece respirators with an active-venting system: a computational study. PLoS ONE 10(6):e0130306. https://doi.org/10.1371/journal.pone.0130306
Nikiforuk AM, Cutts TA, Theriault SS, Cook BWM (2017) Challenge of liquid stressed protective materials and environmental persistence of Ebola Virus. Sci Rep 7(1):4388. https://doi.org/10.1038/s41598-017-04137-2
Roberge RJ, Kim JH, Coca A (2012) Protective facemask impact on human thermoregulation: an overview. Ann OccupHyg 56(1):102–112. https://doi.org/10.1093/annhyg/mer069
Cheng KK, Lam TH, Leung CC (2020) Wearing face masks in the community during the COVID-19 pandemic: altruism and solidarity. Lancet S0140–6736(20):30918–30921. https://doi.org/10.1016/S0140-6736(20)30918-1
Funding
There was no support of any kind, which includes grants, equipment, drugs, and/or other support that facilitated conduct of the work described in the article or the writing of the article itself.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Consent for publication
The research ensured confidentiality of participant’s personal information along with the data they provided. Informed consent was obtained from an individual participant included in the study.
Ethical Approval
Survey research did not deliver any sort of intervention to research participants; thus, there is no risk of physical harm to participating individuals. No procedures or interventions were performed in the study. The survey methodology used in this study involved adult human participants and was strictly in accordance with the ethical standards of the institutional research and ethics committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. No vulnerable groups were included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Disclaimer: The views expressed in the submitted article are our own and not an official position of the institution or any funder.
Rights and permissions
About this article

Cite this article
Gupta, M., Singh, A. & Gupta, M. An Otorhinolaryngologists Perspective on Using Face Masks by Health Care Professionals Based on an Online Survey. Indian J Otolaryngol Head Neck Surg 74 (Suppl 2), 2785–2790 (2022). https://doi.org/10.1007/s12070-020-02248-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12070-020-02248-3