
Abstract
Objective
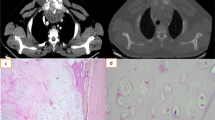
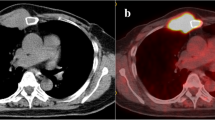
Sternal tumour, though an extremely rare entity in clinical practice, constitutes a great therapeutic challenge in view of its critical domain and function in thoracic cage. Neoplasm of sternum necessitates subtotal/total sternectomy that in turn mandates secure and concrete reconstruction to protect important thoracic organs and provide optimal cardio-respiratory function.
Methods
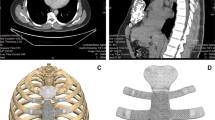
This report is based on retrospective study of three patients with sternal tumours for whom Senior Author performed subtotal sternal resection and reconstruction over a period from 2010 to 2012. A 29-year-old male presented with osteoclastoma of the manubrium and upper sternum and the other two with metachronal sternal metastasis from chondrosarcoma from the lower limb and carcinoma breast. Methyl methacrylate powder was initially mixed with sterile water to make into paste and then allowed to solidify exactly in the shape of excised sternum with or without costal cartilage and ribs. The rigid cast was then fitted into the gap and appropriately fixed which was reinforced with myocutaneous flap for cover using bilateral pectoralis major muscles.
Results
All three patients made satisfactory recovery with stable chest wall, normal cardio-respiratory function and satisfactory cosmesis. Patients were followed up after 3 weeks with clinical assessment and X-ray at 6 months and yearly thereafter. Follow-up ranged from 2 to 4 years with patients enjoying good quality of life. Secure repair was confirmed clinically and by CT scan (computed tomography) study performed at least once between 6 months to 1 year.
Conclusion
Our standardized technique of reconstruction of sternum using polymethyl methacrylate implant prepared exactly in the shape of excised sternum and costal cartilages/ ribs reinforced with pectoralis major myocutaneous flap yielded excellent results at medium-term follow-up.


Similar content being viewed by others
References
Martini N, Huvos AG, Burt ME, et al. Predictors of survival in malignant tumours of the sternum. J Thorac Cardiovasc Surg. 1996;111:96–106.
Watanabe A, Watanabe T, Obama T, Oshawa H, Mawatari T, Ichimiya Y. New material for reconstruction of anterior chest wall, including the sternum. J Thorac Cardiovasc Surg. 2003;126:1212–1214. 2003 The American Association for Thoracic Surgery.
Pedersen TA, Pilegaard HK. Reconstruction of the thorax with Ley prosthesis after resection of the sternum. Ann Thorac Surg. 2009;87:e31–3.
Rocco G, Fazioli F, Scognamiglio F, et al. The combination of multiple materials in the creation of an artificial anterior chest cage after extensive demolition for recurrent chondrosarcoma. J Thorac Cardiovasc Surg. 2007;133:1112–4.
Van Gool VA. Preformed polymethylmethacrylate cranioplasties. J Maxillofac Surg. 1985;13:2–8.
Acknowledgments
Authors gratefully acknowledge Dr Saffia, professor in plastic surgery, Medical College, Trivandrum, Kerala, India, for her contribution.
Conflict of interest
The authors declared that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Additional information
Recipient of a research scholarship
Corresponding author is not a recipient of any research scholarship
Rights and permissions
About this article

Cite this article
Veerbhadran, S., Venkat, E.H., Peter, A. et al. A strategy for near normal reconstruction of sternum. Indian J Thorac Cardiovasc Surg 31, 336–339 (2015). https://doi.org/10.1007/s12055-015-0396-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12055-015-0396-z