
Abstract
Background
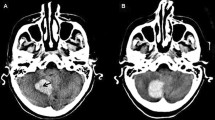
Blend sign on initial computed tomography (CT) is associated with poor outcome in patients with intracerebral hemorrhage (ICH). However, the mechanisms underlying the blend sign formation are poorly understood. The present study aimed to explore the possible mechanism of the CT blend sign in patients with ICH.
Methods
Seventy healthy rabbits were selected to prepare an ICH model. The animals were assigned to a whole blood group + whole blood group (ww group, 50 rabbits), a whole blood + plasma group (wp group, 10 rabbits) or a whole blood + serum group (ws group, 10 rabbits). The animals of the ww group were allocated to five subgroups based on the interval between the first infusion of blood and the second one. The subgroups included ww 1 h group (with an interval of 1 h), ww 2 h group, ww 3 h group, ww 4 h group and ww 5 h group. The rabbits from each group received first infusion of 0.3 mL of whole blood into the basal ganglia area to form a hematoma. Then, they received a second infusion of the same amount of whole blood, plasma or serum into the brain to form another hematoma adjacent to the first one.
Results
A hematoma with two densities on brain CT could be formed in each group after a second infusion of blood into the brain. A significant difference in CT attenuation values was observed between the hyperattenuation and the hypoattenuation in all the groups. However, only the morphological features of the hematoma in the ww group was in accordance with the CT blend sign observed in humans. The CT attenuation values in the hypodensity area of the ww 4 h group or the ww 5 h group were decreased compared with the ww 1 h group to the ww 3 h group.
Conclusions
The CT blend sign observed in humans might be composed of two parts of blood with different ages. The hypodense area might be blood with older age and the hyperdense area might be new bleeding.









Similar content being viewed by others


References
Aguilar MI, Brott TG. Update in intracerebral hemorrhage. The Neurohospitalist. 2011;1(3):148–59.
Chen S, Yang Q, Chen G, Zhang JH. An update on inflammation in the acute phase of intracerebral hemorrhage. Transl Stroke Res. 2015;6(1):4–8.
Wu G, Shi J, Wang F, Wang L, Feng A, Ren S. Effects of minimally invasive procedures for evacuation of intracerebral hematoma in early stages on MMP-9 and BBB permeability in rabbits. BMC Neurol. 2014;14:85.
Blacquiere D, Demchuk AM, Al-Hazzaa M, et al. Intracerebral hematoma morphologic appearance on noncontrast computed tomography predicts significant hematoma expansion. Stroke. 2015;46(11):3111–6.
Dowlatshahi D, Brouwers HB, Demchuk AM, et al. Predicting intracerebral hemorrhage growth with the spot sign: the effect of onset-to-scan time. Stroke. 2016;47(3):695–700.
Barras CD, Tress BM, Christensen S, et al. Quantitative CT densitometry for predicting intracerebral hemorrhage growth. AJNR Am J Neuroradiol. 2013;34(6):1139–44.
Li Q, Zhang G, Huang YJ, et al. Blend sign on computed tomography: novel and reliable predictor for early hematoma growth in patients with intracerebral hemorrhage. Stroke. 2015;46(8):2119–23.
Zheng J, Yu Z, Xu Z, et al. The accuracy of the spot sign and the blend sign for predicting hematoma expansion in patients with spontaneous intracerebral hemorrhage. Med Sci Monit Int Med J Exp Clin Res. 2017;23:2250–7.
Wu G, Shen Z, Wang L, Sun S, Luo J, Mao Y. Post-operative re-bleeding in patients with hypertensive ICH is closely associated with the CT blend sign. BMC Neurol. 2017;17(1):131.
Li Q, Zhang G, Xiong X, et al. Black hole sign: novel imaging marker that predicts hematoma growth in patients with intracerebral hemorrhage. Stroke. 2016;47(7):1777–81.
Wu G, Wu J, Jiao Y, Wang L, Wang F, Zhang Y. Rosiglitazone infusion therapy following minimally invasive surgery for intracerebral hemorrhage evacuation decreases matrix metalloproteinase-9 and blood-brain barrier disruption in rabbits. BMC Neurol. 2015;15:37.
Wu G, Jiao Y, Wu J, et al. Rosiglitazone infusion therapy following minimally invasive surgery for intracranial hemorrhage evacuation decreased perihematomal glutamate content and blood–brain barrier permeability in rabbits. World Neurosurg. 2018;111:e40–6.
Al-Ryalat NT, AlRyalat SA, Malkawi LW, Al-Zeena EF, Najar MS, Hadidy AM. Factors affecting attenuation of dural sinuses on noncontrasted computed tomography scan. J Stroke Cerebrovasc Dis. 2016;25(10):2559–65.
Wang L, Wang F, Wu G, Shi J. Early-stage minimally invasive procedures decrease perihematomal endothelin-1 levels and improve neurological functioning in a rabbit model of intracerebral hemorrhage. Neurol Res. 2015;37(4):320–7.
Wang Z, Zhou F, Dou Y, et al. Melatonin alleviates intracerebral hemorrhage-induced secondary brain injury in rats via suppressing apoptosis, inflammation, oxidative stress, DNA damage, and mitochondria injury. Transl Stroke Res. 2018;9(1):74–91.
VanDerWerf J, Kurowski D, Siegler J, Ganguly T, Cucchiara B. Combination of intra-hematomal hypodensity on CT and BRAIN scoring improves prediction of hemorrhage expansion in ICH. Neurocrit Care. 2018;29(1):40–6.
Chen-Roetling J, Regan RF. Targeting the Nrf2-heme Oxygenase-1 axis after intracerebral hemorrhage. Curr Pharm Des. 2017;23(15):2226–37.
Parizel PM, Makkat S, Van Miert E, Van Goethem JW, van den Hauwe L, De Schepper AM. Intracranial hemorrhage: principles of CT and MRI interpretation. Eur Radiol. 2001;11(9):1770–83.
Petersen OF, Espersen JO. How to distinguish between bleeding and coagulated extradural hematomas on the plain CT scanning. Neuroradiology. 1984;26(4):285–92.
Del Marmol O, Coulier B. “Black” and “white” blood on unenhanced CT. J Belg Soc Radiol. 2019;103(1):16.
Ito H, Maeda M, Uehara T, Yamamoto S, Tamura M, Takashima T. Attenuation values of chronic subdural haematoma and subdural effusion in CT scans. Acta Neurochir. 1984;72(3–4):211–7.
Wu G, Wu J, Wang L, Jiao Y, Zhou H, Tang Z. Minimally invasive surgery for ICH evacuation followed by rosiglitazone infusion therapy increased perihematomal PPARγ expression and improved neurological outcomes in rabbits. Neurol Res. 2016;38(3):261–8.
Zhou Y, Wang Y, Wang J, Anne Stetler R, Yang QW. Inflammation in intracerebral hemorrhage: from mechanisms to clinical translation. Prog Neurobiol. 2014;115:25–44.
Pospísil J. Postirradiation haemorrhagic syndrome. Acta Univ Carol Med Monogr. 1987;99:1–187.
Cai J, Zhu H, Yang D, et al. Accuracy of imaging markers on noncontrast computed tomography in predicting intracerebral hemorrhage expansion. Neurol Res. 2020;42:973–9.
Zhang F, Li H, Qian J, et al. Hyperglycemia predicts blend sign in patients with intracerebral hemorrhage. Med Sci Monit. 2018;24:6237–44.
Kelley RE, Berger JR, Scheinberg P, Stokes N. Active bleeding in hypertensive intracerebral hemorrhage: computed tomography. Neurology. 1982;32(8):852–6.
Acknowledgements
We are grateful for the help provided by the Image Department of the Affiliated Wudang Hospital of Guizhou Medical University in the analysis of computed tomography. We also wish to thank all the postgraduates that were involved in this study for their hard work.
Funding
This research was supported by the Natural Science Foundation of China (81971126/H0906) and the Guizhou Science and Technology Foundation (qiankehe LH(2017)7187). The Funding body did not take part in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
GW, ZT and QL conceived the study, participated in the design of the study, coordinated the study and drafted the manuscript. YL, SR and YM conducted the clinical and experimental study and performed the statistical analyses. LW helped to draft the manuscript. All the authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Conflicts of interest
There are no conflicts of interest
Ethical approval/Informed consent
The present study was approved by the Experimental Animal Ethics Committee of Guizhou Medical University.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Li, Y., Ren, S., Wang, L. et al. Is the CT Blend Sign Composed of Two Parts of Blood with Different Age?. Neurocrit Care 35, 367–378 (2021). https://doi.org/10.1007/s12028-020-01165-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-020-01165-1