
Abstract
Background
Hyperglycemia in out-of-hospital cardiac arrest (OHCA) survivors is associated with poor outcomes. However, in the control of initial hyperglycemia, an adequate strategy to improve patients’ neurologic outcomes remains undetermined. Prior to the establishment of such strategy, we need to determine whether a decreased rate of initial blood glucose (BG) affects patient outcomes.
Methods
One hundred and forty-five adult non-traumatic OHCA survivors treated with therapeutic hypothermia between April 2007 and December 2011 were enrolled in this single-center retrospective cohort study. Based on the cerebral performance category (CPC) at 6 months after OHCA, study populations were categorized as “Good CPC group” (favorable outcome, CPC1 and CPC2) and “Poor CPC group” (unfavorable outcome, CPC3–CPC5). Variables related to BG were obtained, and the rate of BG change was calculated.
Results
In the Good CPC group, the time required to attain target BG levels was shorter [7.4 (2.97–18.13) vs. 13.17 (7.55–27.0) h, p < 0.001], and the average rate of glucose decrease until the attainment of target BG levels was faster [17.06 (6.67–34.49) vs. 8.33 (4.26–18.55) mg/dl/h, p = 0.005] than in the Poor CPC group. Using multivariate analysis, the faster rate (odds ratio 1.074; 95% confidence interval 1.029–1.12; p = 0.001) and the shorter time (odds ratio 13.888; 95% confidence interval 2.271–84.906; p = 0.004) required to attain target BG levels were independently related to favorable neurologic outcomes.
Conclusions
Faster rates of initial BG decrease and the shorter time required to attain target BG levels were associated with favorable neurologic outcome in survivors of OHCA receiving therapeutic hypothermia.


Similar content being viewed by others


References
Nielsen N, Sunde K, Hovdenes J, et al. Adverse events and their relation to mortality in out-of-hospital cardiac arrest patients treated with therapeutic hypothermia. Crit Care Med. 2011;39:57–64.
Oksanen T, Skrifvars MB, Varpula T, et al. Strict versus moderate glucose control after resuscitation from ventricular fibrillation. Intensive Care Med. 2007;33:2093–100.
Longstreth WT Jr, Inui TS. High blood glucose level on hospital admission and poor neurological recovery after cardiac arrest. Ann Neurol. 1984;15:59–63.
Mullner M, Sterz F, Binder M, Schreiber W, Deimel A, Laggner AN. Blood glucose concentration after cardiopulmonary resuscitation influences functional neurological recovery in human cardiac arrest survivors. J Cereb Blood Flow Metab. 1997;17:430–6.
Kim SH, Choi SP, Park KN, et al. Association of blood glucose at admission with outcomes in patients treated with therapeutic hypothermia after cardiac arrest. Am J Emerg Med. 2014;32:900–4.
Langhelle A, Tyvold SS, Lexow K, Hapnes SA, Sunde K, Steen PA. In-hospital factors associated with improved outcome after out-of-hospital cardiac arrest. A comparison between four regions in Norway. Resuscitation. 2003;56:247–63.
Daviaud F, Dumas F, Demars N, et al. Blood glucose level and outcome after cardiac arrest: insights from a large registry in the hypothermia era. Intensive Care Med. 2014;40:855–62.
Beiser DG, Carr GE, Edelson DP, Peberdy MA, Hoek TL. Derangements in blood glucose following initial resuscitation from in-hospital cardiac arrest: a report from the national registry of cardiopulmonary resuscitation. Resuscitation. 2009;80:624–30.
Losert H, Sterz F, Roine RO, et al. Strict normoglycaemic blood glucose levels in the therapeutic management of patients within 12 h after cardiac arrest might not be necessary. Resuscitation. 2008;76:214–20.
Lee BK, Lee HY, Jeung KW, Jung YH, Lee GS, You Y. Association of blood glucose variability with outcomes in comatose cardiac arrest survivors treated with therapeutic hypothermia. Am J Emerg Med. 2013;31:566–72.
Cueni-Villoz N, Devigili A, Delodder F, et al. Increased blood glucose variability during therapeutic hypothermia and outcome after cardiac arrest. Crit Care Med. 2011;39:2225–31.
Callaway CW, Donnino MW, Fink EL, et al. Part 8: post-cardiac arrest care: 2015 American heart association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132:S465–82.
Woo JH, Lim YS, Yang HJ, et al. Factors associated with pneumonia in post-cardiac arrest patients receiving therapeutic hypothermia. Am J Emerg Med. 2014;32:150–5.
Hermanides J, Vriesendorp TM, Bosman RJ, Zandstra DF, Hoekstra JB, Devries JH. Glucose variability is associated with intensive care unit mortality. Crit Care Med. 2010;38:838–42.
Song GH, You YH, Jeong WJ, et al. Vasopressor requirement during targeted temperature management for out-of-hospital cardiac arrest caused by acute myocardial infarction without cardiogenic shock. Clin Exp Emerg Med. 2016;3:20–6.
Trzeciak S, McCoy JV, Phillip DR, et al. Early increases in microcirculatory perfusion during protocol-directed resuscitation are associated with reduced multi-organ failure at 24 h in patients with sepsis. Intensive Care Med. 2008;34:2210–7.
Nurmi J, Boyd J, Anttalainen N, Westerbacka J, Kuisma M. Early increase in blood glucose in patients resuscitated from out-of-hospital ventricular fibrillation predicts poor outcome. Diabetes Care. 2012;35:510–2.
Longstreth WT Jr, Diehr P, Cobb LA, Hanson RW, Blair AD. Neurologic outcome and blood glucose levels during out-of-hospital cardiopulmonary resuscitation. Neurology. 1986;36:1186–91.
Martin GB, O’Brien JF, Best R, Goldman J, Tomlanovich MC, Nowak RM. Insulin and glucose levels during CPR in the canine model. Ann Emerg Med. 1985;14:293–7.
Drews G, Debuyser A, Nenquin M, Henquin JC. Galanin and epinephrine act on distinct receptors to inhibit insulin release by the same mechanisms including an increase in K+ permeability of the B-cell membrane. Endocrinology. 1990;126:1646–53.
Callaham M, Madsen CD, Barton CW, Saunders CE, Pointer J. A randomized clinical trial of high-dose epinephrine and norepinephrine vs standard-dose epinephrine in prehospital cardiac arrest. JAMA. 1992;268:2667–72.
Kim JJ, Hyun SY, Hwang SY, et al. Hormonal responses upon return of spontaneous circulation after cardiac arrest: a retrospective cohort study. Crit Care. 2011;15:R53.
Oshima C, Kaneko T, Tsuruta R, et al. Increase in plasma glucagon, a factor in hyperglycemia, is related to neurological outcome in postcardiac-arrest patients. Resuscitation. 2010;81:187–92.
Ettleson MD, Arguello V, Wallia A, Arguelles L, Bernstein RA, Molitch ME. Hyperglycemia and insulin resistance in cardiac arrest patients treated with moderate hypothermia. J Clin Endocrinol Metab. 2014;99:E2010–4.
Busch M, Soreide E, Lossius HM, Lexow K, Dickstein K. Rapid implementation of therapeutic hypothermia in comatose out-of-hospital cardiac arrest survivors. Acta Anaesthesiol Scand. 2006;50:1277–83.
Sah Pri A, Chase JG, Pretty CG, et al. Evolution of insulin sensitivity and its variability in out-of-hospital cardiac arrest (OHCA) patients treated with hypothermia. Crit Care. 2014;18:586.
Torlinska T, Perz M, Madry E, Hryniewiecki T, Nowak KW, Mackowiak P. Effect of hypothermia on insulin-receptor interaction in different rat tissues. Physiol Res. 2002;51:261–6.
Helman A, Gilbert M, Pfister-Lemaire N, Reach G, Assan R. Glucagon and insulin secretion and their biological activities in hypothermic rats. Endocrinology. 1984;115:1722–8.
Kim SH, Park KN, Choi SP, et al. Time to reach target glucose level and outcome after cardiac arrest patients treated with therapeutic hypothermia. J Crit Care. 2015;30:1204–9.
Peng TJ, Andersen LW, Saindon BZ, et al. The administration of dextrose during in-hospital cardiac arrest is associated with increased mortality and neurologic morbidity. Crit Care. 2015;19:160.
Lundy EF, Kuhn JE, Kwon JM, Zelenock GB, D’Alecy LG. Infusion of five percent dextrose increases mortality and morbidity following six minutes of cardiac arrest in resuscitated dogs. J Crit Care. 1987;2:4–14.
Nakakimura K, Fleischer J, Drummond J, et al. Glucose administration before cardiac arrest worsens neurologic outcome in cats. Anesthesiology. 1990;72:1005–11.
Voll CL, Whishaw IQ, Auer RN. Postischemic insulin reduces spatial learning deficit following transient forebrain ischemia in rats. Stroke. 1989;20:646–51.
Acknowledgements
None.
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
“All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards”. “For this type of study formal consent is not required.”
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
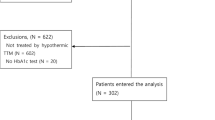
12028_2016_353_MOESM1_ESM.tif
Supplementary Material 1 Flow chart of patient enrollment and exclusion. TH, therapeutic hypothermia; OHCA, out-of-hospital cardiac arrest; ROSC, return of spontaneous circulation; BG, blood glucose; CPC, cerebral performance category (TIFF 403 kb)
Rights and permissions
About this article

Cite this article
Woo, JH., Lim, Y.S., Yang, H.J. et al. The Relationship Between the Decreased Rate of Initial Blood Glucose and Neurologic Outcomes in Survivors of Out-of-Hospital Cardiac Arrest Receiving Therapeutic Hypothermia. Neurocrit Care 26, 402–410 (2017). https://doi.org/10.1007/s12028-016-0353-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-016-0353-8