
Abstract
The therapeutic activity of 131I administered to patients with Graves’ disease can be calculated by means of Marinelli’s formula. The thyroidal iodine uptake (131IUmax) needed for the calculation is usually determined with the use of 131I. The purpose of the paper was to estimate 131IUmax on the basis of technetium uptake in the thyroid at 20 min (99mTcU20min). Eighty patients suffering from Graves’ disease were qualified for radioiodine therapy with measurement of fT4, fT3, thyroid-stimulating hormone and its receptor (TRAb). Prior to the treatment, all the patients were euthyroid. 131IUmax for each patient was determined according to the levels of 131I after 24 h (131IU24h), while effective half-life (T eff) according to the measurements of 131IU24h and 131I uptake after 48 h (131IU48h). Additionally, on the day before measuring 131IU24h, 99mTcU20min was calculated for each patient. It was demonstrated that there existed a correlation, with statistical significance at p < 0.05, between the following pairs of values: TRAb and 131IU24h, TRAb and 99mTcU20min, and 99mTcU20min and 131IU24h. The interdependence between 131IU24h and 99mTcU20min at the level of significance p < 0.05 is described by the following algorithms: 131IU24h = 17.72 × ln (99mTcU20min) + 30.485, if TRAb < 10 IU/ml, and 131IU24h = 18.03 × ln (99mTcU20min) + 38.726, if TRAb > 10 IU/ml. It is possible to predict thyroid iodine uptake 131IU24h in Graves’ disease on the basis of measuring the uptake of 99mTcU20min. This shortens the time necessary for diagnosis and enables the calculation of 131I activity using Marinelli’s formula.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Radiotherapy is, apart from pharmacotherapy and surgical intervention, one of the major methods of treatment for Graves’ disease (GD). Effective radioiodine therapy for GD consists in calculating an appropriate activity of the radioisotope in order to achieve the highest possible therapeutic efficacy, with the lowest possible radiation of the thyroid, and thus of the patient. The clinics that offer radioiodine therapy in Europe and around the world use various methods of selecting correct therapeutic activities of 131I. Our department applies the Marinelli formula, which is recommended by the European Association of Nuclear Medicine (EANM) [1]. Radioiodine 131I is usually used to determine the thyroidal iodine uptake required by the formula. Some also use the iodine isotope 123I, although much less frequently because of the high costs of its production in a cyclotron [2, 3]. The disadvantages of using 131I for therapeutic purposes include: beta radiation during radioactive decay, relatively high gamma radiation energy (364 keV) and the long time (usually 24 h) that is required for assessing the maximum iodine uptake in the thyroid. Technetium 99mTc is another isotope which, like 131I, is absorbed by thyrocytes, thanks to sodium/iodide symporter (NIS) proteins. Contrary to 131I, it is a pure emitter of gamma radiation, with a much shorter half-life (T 1/2) of 6.04 h (8 days in the case of 131I). Moreover, the gamma radiation of technetium carries far less energy than that of iodine (140 keV). Also the time needed for the assessment of its maximum uptake by the thyroid is much shorter than in the case of 131I and equals only 20 min. This allows to diminish the time of thyroid diagnostic. As far as their metabolism in thyroid cells is concerned, a major difference between 99mTc and 131I is that the former does not participate in the synthesis of hormones. Nevertheless, the thyroidal uptake of both 9mTc and 131I in GD depends primarily on the level of thyroid-stimulating hormone (TSH) receptor antibodies (TRAbs), which stimulate the NIS protein to active transport of isotopes into thyrocytes, as well as by intercellular metabolism [4, 5]. The question arises, therefore, whether the assessment of thyroid iodine uptake needed for Marinelli’s formula could be performed with the help of 99mTc. Thus the aims of this study were as follows:
-
(1)
An attempt to create an algorithm to assess thyroidal iodine uptake in GD patients qualified for radioactive iodine therapy on the basis of 99mTc scintigraphy of the thyroid.
-
(2)
Transformation of Marinelli’s formula used for calculating therapeutic activities of 131I by substituting thyroid iodine uptake with thyroid 99mTc uptake.
Materials and methods
The study sample comprised 80 GD patients: 61 women and 19 men. All the subjects had been referred to the Department of Nuclear Medicine with a view to treating hyperthyroidism, following unsuccessful attempts at pharmacotherapy with thyrostatic drugs (the treatment periods being no shorter than 1.5 years). Prior to the administration of a therapeutic dose of 131I, each patient had undergone routine eligibility screening, involving an initial measurement of the thyrotropic hormone, TSH (reference range 0.3–4.0 µIU/ml), free thyroxine, fT4 (reference range 0.71–1.85 ng/dl) and free triiodothyronine, fT3 (reference range 1.45–3.48 pg/mL), using the immunoenzymatic method, Microparticle Enzyme Immunoassay (Abbott Park, USA), and TSH-TRAb (normal < 2 IU/l) using the radioimmunological method (TRAK Human BRAHMS, Germany). Subsequently it was decided that further diagnostics could only involve those subjects who were euthyroid. Hyperthyroid patients continued to be treated with thyrostatics until euthyroid, up to 2 days before the study.
Next, the 24- and 48-h thyroidal iodine uptake tests were carried out after per os (fasting) administration of a capsule containing 131I with the activity of 4 MBq. Additionally, 1 day before the IU24h, scintigrams of the thyroid glands were performed, following an intravenous administration of 80 MBq 99mTc. The readouts of thyroid-absorbed radiation began at 20 min of the administration of the radio marker. Both the iodine uptake tests and the technetium scintigraphy estimating the marker’s uptake in the gland were performed with a gamma-camera (NuclineTM Th, Mediso, Hungary), in accordance with the standard procedures. The volume of the thyroid (m) was estimated by means of a ultrasonography (USG). USG device was equipped with a 12 L linear transducer (LOGIQ S8, GE Healthcare, USA).
The required therapeutic activity of 131I (A) was calculated with Marinelli’s formula [6]:
where
A—131 I therapeutic activity (MBq)
25—unit conversion coefficient
m—mass of thyroid gland calculated with USG (g)
D—absorbed dose of 131 I (Gy), with D = 150 Gy, as recommended by EANM for GD [1]
IU 24h —24-h 131 I uptake (%)
T eff—effective 131 I half-life in thyroid gland (days) calculated with gamma-camera based on 131 IU 24h and 131 IU 48h
The study was approved by the Ethics Committee for Medical Research, Medical University, and is compliant with the good clinical practice guidelines. Informed consent was given by all patients participating in the study.
Statistical analysis
The statistical analysis of the results of the study was conducted using the software package Statistica 10 (Stat Soft, Tulsa, USA).
A multivariate analysis of variance was used to investigate the influence of fT4, fT3, TSH, m and TRAb on IU24h, T eff and 99mTcU20min. The significance level was p < 0.05.
The non-linear regression function was used to establish the correlation of the IU24h, 99mTcU20min and TRAb parameters, with the level of significance at p < 0.05.
Results
It can be noticed among the parameters measured in GD patients in the course of the eligibility study, the effective 131I half-life in the thyroid gland (T eff) has a very low standard deviation (±0.04) and that its mean value equals 5.5 days, while the serum level of thyroid hormones in all the patients before treatment remains within the normal limits, thanks to an effective therapy with thyrostatic medications (Table 1).
Comparison of the parameters measured in the patients during the eligibility screening period demonstrates that there exists a statistically significant (p < 0.05) correlation between the following pairs: TRAb and 131IU24h, TRAb and 99mTcU20min, 99mTcU20min and 131IU24h (Table 2).
The statistical analysis revealed that the highest correlation between 99mTc and 131I occurs when the TRAb titre is either <10 IU/ml or >10 IU/ml.
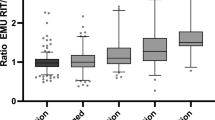
Using this information, further analysis involved the non-linear regression model in order to generate a mathematical formula that would describe the relationship between 131IU24h and 99mTcU20min for the two ranges of TRAb titres, assuming the significance at p < 0.05. It stems from the calculations (Figs. 1 and 2) that the regression model that predicts the dependence of IU24h on 99mTcU20min, if TRAb < 10 IU/ml, looks as follows:
whereas if TRAb > 10 IU/ml:

Scatter graph for variables 99mTcU20min and 131IU24h, with TRAb < 10 IU/ml, and regression equation illustrating their relationship

Scatter graph for variables 99mTcU20min and 131IU24h, with TRAb > 10 IU/ml, and regression equation illustrating their relationship
By substituting 131IU24h in the Marinelli formula with the above correlations, and T eff with the number 5.5 (the value of T eff in all the patients equalled approximately 5.5; see Table 1), we will obtain transformed formulas that can be used to calculate the therapeutic activity of 131I on the basis of thyroid 99mTcU20min uptake.
If TRAb < 10 IU/ml, the transformed Marinelli’s formula takes this form:
whereas if TRAb > 10 IU/ml, it looks as follows:
Discussion
The therapeutic effect of the ionising radiation of 131I applied in the course of hyperthyroidism treatment depends above all on the dose of radiation absorbed by the thyroid gland. This statement is one of the key points of the standards regarding radioiodine treatment for hyperthyroidism issued by the EANM. The EANM guidelines mention the ranges of absorbed doses of ionising radiation according to the type of hyperthyroidism. In patients with autonomous nodules, the recommended dose is 300–400 Gy. In patients with GD, the dose with the aim of restoring a euthyroid status is approximately 150 Gy, whereas the dose to achieve complete ablation is in the range 200–300 Gy. For calculating the therapeutic activity of radioiodine, the EANM guidelines recommend the Marinelli formula. Apart from the aforementioned absorbed dose, the formula requires the evaluation of maximum thyroidal iodine uptake and of the effective half-life of radioiodine in the thyroid [1]. In an accurately prepared GD patient, the effective half-life has—according to our calculations—a steady value of 5.5 days on average [7–10]. This is why we are convinced that Marinelli’s formula can be simplified by substituting T eff with 5.5 days.
In their attempts to streamline the calculation of the therapeutic activity of radioactive iodine using Marinelli’s formula, some authors resort to a variety of methods to determine the value of maximum thyroid iodine uptake. As a rule, the maximum uptake occurs after 24 h of the administration of radioactive iodine (131I) [10–12]. Morris and Hayes et al. propose algorithms for predicting 131I uptake through measuring it after 4 or 6 h, which considerably shortens the time of the procedure. In Morris’ study, the difference between the actual 24 h measurement and the estimated value after 4 h amounted to +10 %, and +5.9 % after 6 h. Hayes et al., meanwhile, proved that the correlation coefficient between the actual measurements and the 4- and 6-h estimates was high, reaching r = 0.94 [13, 14].
Still another approach to the problem can be found in the research results published by authors such as Shapiro or Yaqub. In both studies the maximum thyroid uptake in GD patients was calculated—as it usually is—after 24 h, but it was done by means of 123I instead of 131I. 123I possesses better physical parameters for isotope diagnostics (123I, in contrast to 131I, is a pure emitter of gamma radiation, characterised by a lower energy level and shorter half-life) [15, 16]. Osaki et al. combined the above two approaches to calculating IUmax based on Marinelli’s formula by assuming that it represented by the value of 24 h thyroidal iodine uptake and can be predicted using the 123I uptake after 3 h. They claim in their publication that the algorithm they propose for determining the correlation between the 3- and the 24-h thyroidal iodine uptake is statistically significant (p < 0.001) and can be used in clinical practice [8]. It has to be noted, however, that as for practical application, this method has the distinct disadvantage of being expensive, especially in Poland. The costs of producing the cyclotron-based iodine isotope 123I far outweighs those of acquiring the widely used reactor-produced isotope of iodine, 131I.
Smith et al. present yet another strategy for assessing IUmax in the thyroid, although their research was conducted on patients with non-toxic goitre, not with GD as in the case of the previously mentioned authors. Departing from an analysis of the measurements of thyroid 99mTc and 131I uptake in each of their 44 patients, Smith et al. created an algorithm estimating the 24-h thyroid radioactive iodine uptake based on the level of 99mTc uptake at 5 min of administering the radiomarker. They also emphasise that assessing iodine uptake on the basis of technetium scintigraphy allows for the greatest reduction of the patients’ exposure to ionising radiation. The thyroid absorbed dose of radiation emitted by technetium is 10 times as low as it is when 123I is used, and 10,000 lower than in the case of treatment with 131I. Also the effective dose of ionising radiation received by the entire organism is markedly lower when technetium is used for testing instead of 123I or 131I iodine [17]. The exposition from the diagnostic activity of radioiodine is unimportant considering the dose received from the following radioiodine therapy. Our study uses similar assumption as regards the prediction of thyroidal iodine uptake on the basis of technetium uptake, the only difference being that our sample consisted of patients with GD. The choice of study sample was determined by the fact that in GD the thyroid tissue is usually homogeneous and there are no problems associated with the occurrence of nodules that take up 99mTc and 131I in different ways, as it is sometimes the case in a nodular goitre. These discrepancies result from the lack of 99mTc organification by thyrocytes, which occurs when 131I is used [18]. Had we additionally taken into consideration the measurements of uptake values for the nodular goitre, the study sample would have become overly heterogeneous, making the calculations imprecise.
According to our investigations, the algorithm that depicts the correlation between the uptakes of 131I and 99mTc is determined by the level of TRAb antibodies. The level of TRAb that significantly changes the algorithm equals 10 IU/ml. In clinical practice, this means that when thyroidal iodine uptake is estimated in GD patients on the basis of 99mTc uptake, the level of TRAb antibodies should be taken into account so as to apply the correct algorithm.
In conclusion, predicting the thyroidal uptake of 131IU24h in GD on the basis of measuring 99mTcU20min uptake is possible, thanks to the equation created in the course of our research. The application of this algorithm considerably shortens the time necessary for pre-therapy diagnostic procedures and makes it possible to calculate the therapeutic activity of radioactive iodine with the use of Marinelli’s formula, as recommended by the EANM.
References
M.P. Stokkel, D. Handkiewicz Junak, M. Lassmann, M. Dietlein, M. Luster, EANM procedure guidelines for therapy of benign thyroid disease. Eur. J. Nucl. Med. Mol. Imaging 37, 2218–2228 (2010)
U.S. Vemulakonda, F.B. Atkins, H.A. Ziessman, Therapy dose calculation in Graves’ disease using early I-123 uptake measurements. Clin. Nucl. Med. 21, 102–105 (1996)
J.V. Hennessey, L.A. Berg, M.A. Ibrahim, R.J. Markert, Evaluation of early (5 to 6 hours) iodine 123 uptake for diagnosis and treatment planning in Graves’ disease. Arch. Intern. Med. 155, 621–624 (1995)
L. Giovanella, L. Ceriani, A. Ghelfo, Second-generation thyrotropin receptor antibodies assay and quantitative thyroid scintigraphy in autoimmune hyperthyroidism. Horm. Metab. Res. 40, 484–486 (2008)
S. Tepmongkol, Enhancement of radioiodine uptake in hyperthyroidism with hydrochlorothiazide: a prospective randomised control study. Eur. J. Nucl. Med. Mol. Imaging 29, 1307–1310 (2002)
L.D. Marinelli, E.H. Quimby, G.J. Hine, Dosage determination with radioactive isotopes; practical considerations in therapy and protection. Am. J. Roentgenol. Radium Ther. 59, 260–281 (1948)
C. Kobe, W. Eschner, M. Wild, I. Rahlff, F. Sudbrock, M. Schmidt, M. Dietlein, H. Schicha, Radioiodine therapy of benign thyroid disorders: what are the effective thyroidal half-life and uptake of 131I?. Nucl. Med. Commun. 31, 201–205 (2010)
Y. Osaki, K. Sakurai, Z. Arihara, M. Hata, H. Fukazawa, Prediction of late (24-hour) radioactive iodine uptake using early (3-hour) uptake values in Japanese patients with Graves’ disease. Endocr. J. 59, 173–177 (2012)
H. Hautzel, E. Pisar, N. Yazdan-Doust, M. Schott, M. Beu, H.W. Műller, Qualitative and quantitative impact of protective glucocorticoid therapy on the effective 131I half-life in radioiodine therapy for Graves’ disease. J. Nucl. Med. 51, 1917–1922 (2010)
A.C. Traino, F. Di Martino, M. Lazzeri, M.G. Stabin, Study of the correlation between administered activity and radiation committed dose to the thyroid in 131I therapy of Graves’ disease. Radiat. Prot. Dosimetry 95, 117–124 (2001)
C.H. Read, M.J. Tansey, Y. Menda, A 36-year retrospective analysis of the efficacy and safety of radioactive iodine in treating young Graves’ patients. J. Clin. Endocrinol. Metab. 89, 4229–4233 (2004)
M. Schiavo, M.C. Bagnara, L. Camerieri, E. Pomposeli, M. Giusti, G. Pesce, C. Reitano, M. Caputo, M. Bagnasco, Clinical efficacy of radioiodine therapy in multinodular toxic goiter, applying an implemented dose calculation algorithm. Endocrine 48, 902–908 (2015)
L.F. Morris, A.D. Waxman, G.D. Braunstein, Accuracy considerations when using early (four- or six-hour) radioactive iodine uptake to predict twenty-four-hour values for radioactive iodine dosage in the treatment of Graves’ disease. Thyroid 10, 779–787 (2000)
A.A. Hayes, C.M. Akre, C.A. Gorman, Iodine-131 treatment of Graves’ disease using modified early iodine-131 uptake measurements in therapy dose calculations. J. Nucl. Med. 31, 519–522 (1990)
A. Yaqub, M.I. Choudhry, J. Wheaton, T. Gress, Post-ablative hypothyroidism. W. V. Med. J. 107, 37–40 (2011)
B. Shapiro, D.E. Zanin, R. Schipper, Reference-free thyroid uptake measurement. Nucl. Med. Commun. 35, 382–390 (2014)
J.J. Smith, B.Y. Croft, V.A. Brookeman, C.D. Teates, Estimation of 24-hour thyroid uptake of I-131 sodium iodide using a 5-minute uptake of technetium-99m pertechnetate. Clin. Nucl. Med. 15, 80–83 (1990)
Z. Kusić, D.V. Becker, E.L. Saenger, P. Paras, P. Gartside, T. Wessler, S. Spaventi, Comparison of technetium-99m and iodine-123 imaging of thyroid nodules: correlation with pathologic findings. J. Nucl. Med. 31, 393–399 (1990)
Acknowledgments
We are grateful to all of the staff for helping with the data collection and for the technical assistance. This paper was financed from statutory activity funds of the Medical University of Białystok.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Ethical approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Rights and permissions
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Szumowski, P., Mojsak, M., Abdelrazek, S. et al. Calculation of therapeutic activity of radioiodine in Graves’ disease by means of Marinelli’s formula, using technetium (99mTc) scintigraphy. Endocrine 54, 751–756 (2016). https://doi.org/10.1007/s12020-016-1074-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12020-016-1074-7