
Abstract
Background
Early adverse tissue reactions around metal-on-metal (MoM) hip replacements, especially pseudotumors, are a major concern. Because the causes and pathomechanisms of these pseudotumors remain largely unknown, clinical monitoring of patients with MoM bearings is challenging.
Questions/purposes
The purpose of this study was to compare the lymphocyte subpopulations in peripheral blood from patients with a failed MoM hip implant with and without a pseudotumor and patients with a well-functioning MoM hip implant without a pseudotumor. Potential differences in the systemic immune response are expected to reflect local differences in the periprosthetic tissues.
Methods
Consenting patients who underwent a revision of a failed MoM hip implant at The Ottawa Hospital (TOH) from 2011 to 2014, or presented with a well-functioning MoM hip implant for a postoperative clinical followup at TOH from 2012 to 2013, were recruited for this study, unless they met any of the exclusion criteria (including diagnosed conditions that can affect peripheral blood lymphocyte subpopulations). Patients with a failed implant were divided into two groups: those with a pseudotumor (two hip resurfacings and five total hip arthroplasties [THAs]) and those without a pseudotumor (10 hip resurfacings and two THAs). Patients with a well-functioning MoM hip implant (nine resurfacings and three THAs) at 5 or more years postimplantation and who did not have a pseudotumor as demonstrated sonographically served as the control group. Peripheral blood subpopulations of T cells (specifically T helper [Th] and cytotoxic T [Tc]), B cells, natural killer (NK) cells, memory T and B cells as well as type 1 (expressing interferon-γ) and type 2 (expressing interleukin-4) Th and Tc cells were analyzed by flow cytometry after immunostaining. Serum concentrations of cobalt and chromium were measured by inductively coupled plasma-mass spectrometry.
Results
The mean percentages of total memory T cells and, specifically, memory Th and memory Tc cells were lower in patients with a failed MoM hip implant with a pseudotumor than in both patients with a failed implant without a pseudotumor and patients with a well-functioning implant without a pseudotumor (memory Th cells: 29% ± 5% [means ± SD] versus 55% ± 17%, d = 1.8, 95% confidence interval [CI] [1.2, 2.5] and versus 48% ± 14%, d = 1.6, 95% CI [1.0, 2.2], respectively; memory Tc cells: 18% ± 5% versus 45% ± 14%, d = 2.3, 95% CI [1.5, 3.1] and versus 41% ± 12%, d = 2.3, 95% CI [1.5, 3.1], respectively; p < 0.001 in all cases). The mean percentage of memory B cells was also lower in patients with a failed MoM hip implant with a pseudotumor than in patients with a well-functioning implant without a pseudotumor (12% ± 8% versus 29% ± 16%, d = 1.3, 95% CI [0.7, 1.8], p = 0.025). In addition, patients with a failed MoM hip implant with a pseudotumor had overall lower percentages of type 1 Th cells than both patients with a failed implant without a pseudotumor and patients with a well-functioning implant without a pseudotumor (5.5% [4.9%–5.8%] [median with interquartile range] versus 8.7% [6.5%–10.2%], d = 1.4, 95% CI [0.8, 2.0] and versus 9.6% [6.4%–11.1%], d = 1.6, 95% CI [1.0, 2.2], respectively; p ≤ 0.010 in both cases). Finally, serum cobalt concentrations in patients with a failed MoM hip implant with a pseudotumor were overall higher than those in patients with a well-functioning implant without a pseudotumor (5.8 µg/L [2.9–17.0 µg/L] versus 0.9 µg/L [0.6–1.3 µg/L], d = 2.2, 95% CI [1.4, 2.9], p < 0.001).
Conclusions
Overall, results suggest the presence of a type IV hypersensitivity reaction, with a predominance of type 1 Th cells, in patients with a failed MoM hip implant with a pseudotumor.
Clinical Relevance
The lower percentages of memory T cells (specifically Th and Tc) as well as type 1 Th cells in peripheral blood of patients with a failed MoM hip implant with a pseudotumor could potentially become diagnostic biomarkers for the detection of pseudotumors. Although implant design (hip resurfacing or THA) did not seem to affect the results, as suggested by the scatter of the data with respect to this parameter, future studies with additional patients could include the analysis of implant design in addition to correlations with histological analyses of specific Th subsets in periprosthetic tissues.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
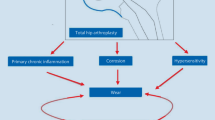
Since the mid-1980s, over one million metal-on-metal (MoM) hip implants have been implanted worldwide [24]. However, an increasing number of studies are reporting adverse tissue reactions to metal products (wear particles and ions), which can compromise clinical results and survivorship of these implants. These adverse tissue reactions include pseudotumors, defined as soft or cystic masses, often associated with pain and soft tissue destruction and frequently leading to revision surgery. Because of bone and soft tissue destruction, these revision procedures are often associated with a high risk of reoperation [1, 11]. In addition, several research groups have reported the presence of pseudotumors in as many as 61% of asymptomatic patients [2, 18, 25, 39].
Various risk factors have been identified for the formation of pseudotumors, including: gender, implant design, and head size as well as abnormal acetabular component positioning usually associated with higher wear, which, in turn, has been associated with pseudotumors [23]. However, pseudotumors have also been observed in the presence of low wear and a hypersensitivity reaction [3]. Therefore, wear alone may not explain pseudotumors around MoM hip implants [5]. Pseudotumor histology includes features consistent with a nonspecific inflammatory reaction to metal wear such as macrophages and particles, but also features consistent with a specific metal hypersensitivity reaction such as lymphocyte aggregates [3, 10]. Although the pathomechanisms of pseudotumors remain largely unknown, the presence of lymphocyte aggregates suggests the involvement of the adaptive immune response and a hypersensitivity reaction. Diagnostic methods of hypersensitivity reactions include dermal patch testing, peripheral blood lymphocyte migration inhibition assays, lymphocyte transformation tests, and enzyme-linked immunosorbent assays (ELISA) for migration inhibitory factor [13, 15]. However, all of these techniques present limitations, and there is currently no standardized testing method for the characterization of hypersensitivity to metallic joint replacement components.
Blood levels of cobalt (Co) and chromium (Cr) ions have been used as a monitoring tool because of their reported correlation with the risk of adverse tissue reactions [25]. However, the reliability of metal ion levels for clinical prognostic remains questionable [17] with no clear cutoff values [19] and interlaboratory variability in measurements [21]. In addition, not all patients with high metal ion levels and high wear develop an adverse tissue reaction [4, 6, 10]. Radiological investigation using sonography is currently recommended to confirm a pseudotumor diagnosis [8]. Unfortunately, imaging does not allow the differentiation between aggressive and benign lesions, and how to assess the severity and the progression of these lesions remains elusive. Therefore, identifying patients at risk of developing aggressive pseudotumors represents a major area of interest.
The purpose of this study was to compare the lymphocyte subpopulations in peripheral blood from three groups of patients with MoM hip implants: patients with a failed implant with and without a pseudotumor and patients with a well-functioning implant without a pseudotumor. Comparisons will reveal potential differences in the systemic immune response that are expected to reflect local differences in the periprosthetic tissues. The main functions of the lymphocytes analyzed in the present study are summarized (Table 1). Because metal implant-related hypersensitivity reactions were reported to be T cell-mediated (type IV) hypersensitivity reactions [9], a local increase in memory T cells would be expected if a type IV hypersensitivity reaction is prevalent in patients with a failed MoM hip implant with a pseudotumor. Furthermore, because type 1 T helper (Th1) cells (ie, Th cells expressing interferon-gamma [IFN-γ]) are involved in type IV hypersensitivity reactions, a local increase in Th cells expressing IFN-γ would also be expected.
Materials and Methods
Patient Groups
This study was approved by the Ottawa Health Science Network Research Ethics Board and written informed consent was obtained from all participants. The study exclusion criteria included active infection, previous revision of the hip implant, fracture, patient-requested removal of a well-functioning implant, bilateral hip implants (well-functioning group only), and diagnosed conditions that can affect peripheral blood lymphocyte subpopulations (rheumatoid arthritis, HIV infection, lupus, pregnancy, and thrombocytosis). All consenting patients who underwent a revision of a failed MoM hip implant at The Ottawa Hospital (TOH) from 2011 to 2014, or presented with a well-functioning MoM hip implant for a postoperative clinical followup at TOH from 2012 to 2013, were recruited for this study (Table 2) unless they met any of the exclusion criteria.
A total of 14 patients with a failed hip resurfacing and eight patients with a failed MoM THA were recruited. Only those for whom a complete data set was available were retained for the analysis (12 with a hip resurfacing and seven with a THA, representing 86% and 88% of the recruited patients with a failed hip resurfacing and THA, respectively). Patients with a failed MoM hip implant were divided into two groups: those with a pseudotumor (two hip resurfacings and five THAs) and those without a pseudotumor (10 hip resurfacings and two THAs). Pseudotumors were diagnosed or confirmed intraoperatively with the observation of a destructive solid or cystic mass in close proximity to the implant.
Patients with a well-functioning MoM hip implant (nine resurfacings and three THAs) at 5 or more years postimplantation who did not have a pseudotumor, as demonstrated sonographically [8], served as the control group. All ultrasounds were performed by a fellowship-trained musculoskeletal radiologist (RF). Patients with a well-functioning implant were assessed at the latest postoperative clinical followup (6 ± 1 years [mean ± SD]; range, 5–8 years) with the WOMAC and the UCLA activity scores. WOMAC scores were 100 (94–100) (median with interquartile range), 88 (75–88), 98 (95–100), and 94 (92–97) for pain, stiffness, function, and total score, respectively, and the UCLA score was 8 (6–8). Patients with a WOMAC score lower than 75 for stiffness and lower than 80 for pain, function, and total score, and/or a UCLA score lower than 6 (with 10 being the best score) were excluded from the study.
Phenotypic Analysis of Peripheral Blood Mononuclear Cells
Peripheral blood was collected, by venipuncture of the median cubital vein, into two 6-mL trace elements Na-heparin evacuated polyethylene terephthalate tubes (Greiner Bio-One, Frickenhausen, Germany). The blood was mixed immediately by gently inverting the tubes eight times. Mononuclear cells were isolated, under aseptic conditions, by neutral density gradient using Ficoll®-Paque PLUS (GE Healthcare Life Sciences, Piscataway, NJ, USA). The cells were washed twice in Roswell Park Memorial Institute (RPMI)-1640 medium (Wisent, St-Bruno, QC, Canada) and resuspended to a concentration of approximately 1.0 x 106 lymphocytes/mL in RPMI-1640 supplemented with heat-inactivated fetal bovine serum (HI-FBS; premium-grade; Wisent) to a final concentration of 10% (v/v). Cells were counted using an improved Neubauer hemocytometer (Hausser Scientific, Horsham, PA, USA).
For extracellular immunostaining, the freshly isolated mononuclear cells were resuspended in cold (4 °C) staining buffer (phosphate-buffered saline [PBS] without Ca+ and Mg2+ [Wisent] containing 2% [v/v] HI-FBS and 0.01% [w/v] NaN3). Aliquots (100 µL) of the cell suspension, at a final nominal concentration of 1 x 106 lymphocytes/mL, were incubated 10 minutes in the dark with selected combinations of the following fluorescently labeled monoclonal antibodies to detect specific cell surface markers: phycoerythrin-Texas red-X (ECD)-labeled mouse antihuman CD3 (0.65 µg/mL; clone UCHT1; BD Biosciences, San Jose, CA, USA) for T cells; phycoerythrin-cyanine 5 (PC5)-labeled mouse antihuman CD4 (0.65 µg/mL; clone 13B8.2; Beckman Coulter, Indianapolis, IN, USA) for Th cells; phycoerythrin-cyanine 7 (PC7)-labeled mouse antihuman CD8 (2.5 µg/mL; clone SFCI21Thy2D3; Beckman Coulter) for cytotoxic T (Tc) cells; fluorescein isothiocyanate (FITC)-labeled mouse antihuman CD19 (10 µg/mL; clone HIB19; eBioscience, San Diego, CA, USA) for B cells; PE-labeled mouse antihuman CD56 (0.30 µg/mL; clone CMSSB; Beckman Coulter) for natural killer (NK) cells; FITC-labeled mouse antihuman CD45RO (2.5 µg/mL; clone UCHL1; eBioscience) for memory T cells; and of phycoerythrin (PE)-labeled mouse antihuman CD27 (0.65 µg/mL; clone 1A4CD27; Beckman Coulter) for memory B cells. The immunostained cells were diluted to 500 µL with staining buffer, transferred into 5-mL polystyrene tubes (Greiner Bio-One), and analyzed immediately by flow cytometry using a Cytomics FC 500 Series flow cytometer (Beckman Coulter).
For intracellular immunostaining, aliquots of freshly isolated mononuclear cells were incubated in a tissue culture-treated 24-well polystyrene plate (Greiner Bio-One) for 5.5 hours at 37 °C in a humidified atmosphere of 95% air and 5% CO2. Triplicate wells each contained 1 mL of cell suspension (1 × 106 lymphocytes) in RPMI-1640 medium containing 10% (v/v) HI-FBS in the presence of phorbol-12-myristate-13-acetate (15 ng/mL; PMA; EMD Millipore, Billerica, MA, USA), ionomycin from Steptomyces conglobatus (1 µM; EMD Millipore), and the protein-transport inhibitor brefeldin A (1:1000 dilution of Golgy Plug™; BD Biociences). Wells for controls contained cell suspension only, cell suspension with the protein-transport inhibitor only, and cell suspension with PMA only. After incubation, the nonadherent cells were collected and immunostained for CD3 and CD4. After washing with staining buffer, the cells were incubated in a 4% (v/v) paraformaldehyde fixation buffer (IC Fixation Buffer; eBioscience) for 15 minutes in the dark at room temperature, washed again, and incubated in 100 µL of a saponin-based permeabilization buffer (1× concentration; eBioscience) for 5 minutes in the dark at room temperature. The cells were then incubated an additional 15 minutes in the dark with the following fluorescently labeled monoclonal antibodies: PC7-labeled mouse antihuman IFN-γ (10 µg/mL; clone 4S.B3; eBioscience) for type 1 cells and PE-labeled mouse antihuman interleukin-4 (IL-4) (1.25 µg/mL; clone 8D4-8; eBioscience) for type 2 cells. Finally, the immunostained cells were washed with staining buffer, resuspended in 500 µL of phosphate-buffered paraformaldehyde (100 mM NaH2PO4, 100 mM Na2HPO4, 4% [w/v] paraformaldehyde, pH 7.2), and analyzed immediately by flow cytometry, as described previously in this article. All flow cytometry data were analyzed using CXP Analysis software Version 2.2 (Beckman Coulter, Brea, CA, USA). Results are expressed as percentages, as detailed in the individual figure legends.
Trace Metal Analysis of Serum
Peripheral blood was collected, as described previously in this article, into a 6-mL trace elements evacuated polyethylene terephthalate tube with a clot activator (BD Diagnostics, Franklin, NJ, USA). The blood was mixed immediately by gently inverting the tubes five times, allowed to clot 30 minutes at room temperature, and centrifuged 10 minutes at 1600 × g at 4 °C. The serum was transferred into an 8-mL polypropylene screw-cap tube (Sarstedt, Montreal, QC, Canada) using a polyethylene plastic transfer pipette (VWR Mississauga, ON, Canada) and frozen/stored at −20 °C. Concentrations of Co and Cr were measured by inductively coupled plasma-mass spectrometry (London Laboratory Services Group, London Health Sciences Centre, London, ON, Canada). Corrections for Co and Cr contamination originating from the container and transfer pipette were not required.
Statistical Analysis
Statistical analysis was implemented in R-3.1.0 [33]. The Shapiro-Wilk and Bartlett tests were used to assess if the data conformed to the assumptions of normality and homogeneity of variance, respectively. Assessment of normality was confirmed using Q-Q (quantile-quantile) plots. When data distributions were normal and variance was homogenous between groups, statistical analysis was performed using the analysis of variance (ANOVA) and Tukey-Kramer post hoc tests. When data distributions were normal but variance was inhomogeneous between groups, statistical analysis was performed using the Welch ANOVA and Games Howell tests. When data distributions were not normal, statistical analysis was performed using the Kruskal-Wallis and two-sided exact Mann-Whitney U-tests. A p value < 0.05 was considered significant. Data are presented as mean ± SD (parametric data) or median with interquartile range (nonparametric data). Cohen’s d effect sizes (ES) for parametric data, adjusted Cohen’s d ES for nonparametric data [7, 20] and confidence intervals (CIs) for Cohen’s d and adjusted Cohen’s d [20, 31] are also presented.
Results
Phenotypic Analysis of Peripheral Blood Mononuclear Cells
No significant differences were observed among the experimental groups for T, B, and NK cells (CD3+, CD19+, and CD56+, respectively) nor for the ratios of Th/Tc (CD3+ CD4+/ CD3+CD8+) cell percentages (p = 0.391, 0.507, 0.303, and 0.178, respectively) (Fig. 1A–D).

This figure presents the subpopulations of peripheral blood lymphocytes. Data are presented as: (A) percentages of cells in the forward scatter/side scatter (FS/SS) lymphocyte gate that are CD3+ (T cells); (B) percentages of cells in the FS/SS lymphocyte gate that are CD19+ (B cells); (C) percentages of cells in the FS/SS lymphocyte gate that are CD56+ (NK cells); and (D) ratios of CD3+CD4+ (Th)/CD3+CD8+ (Tc) percentages. Vertical scatterplots show medians with interquartile ranges (A, C, D) and means ± SD (B). Circles (●) and squares (■) represent data from patients with a hip resurfacing and a THA, respectively. Lines with p values connect groups with significant differences. P = patients with a failed implant with a pseudotumor; NP = patients with a failed implant without a pseudotumor; W-F = patients with a well-functioning implant. Cells were analyzed by flow cytometry after immunostaining.
In contrast, a difference was observed among the experimental groups for total memory T (CD3+CD45RO+), memory Th (CD3+CD4+CD45RO+), and memory Tc (CD3+CD8+CD45RO+) cells (p < 0.001 in all cases). The mean percentages of total memory T cells and, specifically, memory Th cells and memory Tc cells were lower in patients with a failed MoM hip implant with a pseudotumor than in both patients with a failed implant without a pseudotumor and patients with a well-functioning implant without a pseudotumor (total memory T cells: 26% ± 4% versus 48% ± 10%, d = 2.7, 95% CI [1.8, 3.6] and versus 44% ± 12%, d = 1.8, 95% CI [1.1, 2.4], respectively; memory Th cells: 29% ± 5% versus 55% ± 17%, d = 1.8, 95% CI [1.2, 2.5] and versus 48% ± 14%, d = 1.6, 95% CI [1.0, 2.2], respectively; memory Tc cells: 18% ± 5% versus 45% ± 14%, d = 2.3, 95% CI [1.5, 3.1] and versus 41% ± 12%, d = 2.3, 95% CI [1.5, 3.1], respectively; p < 0.001 in all cases) (Fig. 2A–C). A difference was also observed among the three experimental groups for memory B (CD19+CD27+) cells (p = 0.032). Specifically, the mean percentage of memory B cells was lower in patients with a failed MoM hip implant with a pseudotumor than in patients with a well-functioning implant without a pseudotumor (12% ± 8% versus 29% ± 16%, d = 1.3, 95% CI [0.7, 1.8], p = 0.025) (Fig. 2D). There was, however, no significant difference in the mean percentages of memory B cells between patients with a failed MoM hip implant with and without a pseudotumor (12% ± 8% versus 22% ± 12%, d = 1.0, 95% CI [0.5, 1.5], p = 0.208).

This figure presents the subpopulations of peripheral blood memory lymphocytes. Data are presented as percentages of: (A) T cells (CD3+) that are CD45RO+ (memory T cells); (B) Th cells (CD3+CD4+) that are CD45RO+ (memory Th cells); (C) Tc cells (CD3+CD8+) that are CD45RO+ (memory Tc cells); and (D) B cells (CD19+) that are CD27+ (memory B cells), respectively. Vertical scatterplots show means ± SD. Circles (●) and squares (■) represent data from patients with a hip resurfacing and a THA, respectively. Lines with p values connect groups with significant differences. P = patients with a failed implant with a pseudotumor; NP = patients with a failed implant without a pseudotumor; W-F = patients with a well-functioning implant. Cells were analyzed by flow cytometry after immunostaining.
The analysis of intracellular cytokine expression revealed a difference among the three experimental groups for total T cells expressing IFN-γ (p = 0.009). Specifically, patients with a failed MoM hip implant with a pseudotumor had overall lower percentages than both patients with a failed implant without a pseudotumor and patients with a well-functioning implant without a pseudotumor (7% [6%–9%] versus 15% [12%–21%], d = 1.5, 95% CI [0.9, 2.1] and versus 14% [12%–22%], d = 1.8, 95% CI [1.1, 2.4], respectively; p < 0.008 in both cases) (Fig. 3A). For Th cells expressing IFN-γ (type 1 Th cells), a difference was observed among the three experimental groups (p = 0.014). Specifically, patients with a failed MoM hip implant with a pseudotumor had overall lower percentages than both patients with a failed implant without a pseudotumor and patients with a well-functioning implant without a pseudotumor (5.5% [4.9%–5.8%] versus 8.7% [6.5%–10.2%], d = 1.4, 95% CI [0.8, 2.0] and versus 9.6% [6.4%–11.1%], d = 1.6, 95% CI [1.0, 2.2], respectively; p ≤ 0.010 in both cases) (Fig. 3B). There was no significant difference among the three experimental groups for CD3+CD4– cells expressing IFN-γ (considered to be primarily Tc cells expressing IFN-γ, ie, type 1 Tc cells) probably because of the large spread of the data and overlap between the three groups (p = 0.124) (Fig. 3C).

This figure presents the subpopulations of peripheral blood type 1 T lymphocytes. Data are presented as percentages of: (A) T cells (CD3+) that are IFN-γ+ (type 1 T cells); (B) Th cells (CD3+CD4+) that are IFN-γ+ (type 1 Th cells); (C) Tc cells (ie, CD3+CD4– which are considered to be primarily Tc cells) that are IFN-γ+ (type 1 Tc cells). Vertical scatterplots show medians with interquartile ranges. Circles (●) and squares (■) represent data from patients with a hip resurfacing and a THA, respectively. Lines with p values connect groups with significant differences. P = patients with a failed implant with a pseudotumor; NP = patients with a failed implant without a pseudotumor; W-F = patients with a well-functioning implant. Cells were analyzed by flow cytometry after immunostaining.
Finally, there was no significant difference among the three experimental groups for total T cells expressing IL-4 (p = 0.269). Also, the percentages of both CD3+CD4+ and CD3+CD4– cells expressing IL-4 (Th2 and Tc2, respectively) remained low, and the three groups were not significantly different (data not shown).
Trace Metal Analysis of Serum
A difference was observed among the three experimental groups for serum Co concentrations (p = 0.004). Specifically, patients with a failed MoM hip implant with a pseudotumor had overall higher serum Co concentrations than patients with a well-functioning implant without a pseudotumor (5.8 µg/L [2.9–17.0 µg/L] versus 0.9 µg/L [0.6–1.3 µg/L], d = 2.2, 95% CI [1.4, 2.9], p < 0.001) (Fig. 4A). There was, however, no significant difference in serum Co concentrations between patients with a failed MoM hip implant with and without a pseudotumor with the available number of patients (5.8 µg/L [2.9–17.0 µg/L] versus 2.1 µg/L [0.8–3.6 µg/L], d = 1.0, 95% CI [0.4, 1.5]; p = 0.057), possibly because of a patient with a high Co concentration (outlier) in the group of failed MoM hip implants without a pseudotumor. There was also no significant difference among the three experimental groups in serum Cr concentrations (p = 0.108) (Fig. 4B). However, Co and Cr results should be interpreted with care because of differences in the proportions of patients with bilateral hip implants among the three experimental groups (Table 2).

This figure presents the serum Co and Cr concentrations. (A) Co concentrations; (B) Cr concentrations. Vertical scatterplots show medians with interquartile ranges. Circles (●) and squares (■) represent data from patients with a hip resurfacing and a THA, respectively. Lines with p values connect groups with significant differences. P = patients with a failed implant with a pseudotumor; NP = patients with a failed implant without a pseudotumor; W-F = patients with a well-functioning implant. Concentrations of Co and Cr were measured by inductively coupled plasma-mass spectrometry.
Discussion
Adverse tissue reactions associated with joint replacement surgery remain a major complication that can lead to considerable soft tissue destruction impacting implant function and survivorship [30, 32, 36]. Although relatively uncommon, pseudotumors, a type of adverse tissue reaction, are a concern, especially because of the high percentages of asymptomatic lesions [2, 18, 39]. In addition, current investigative tools are limited to metal ion measurements and diagnostic imaging, although both lack sufficient prognostic power and provide limited insight into the risk factors and pathomechanisms leading to these adverse tissue reactions. The present study showed overall lower percentages of memory T cells (specifically Th and Tc) as well as type 1 Th cells (expressing IFN-γ) in peripheral blood of patients with a failed MoM hip implant with a pseudotumor compared with both patients with a failed implant without a pseudotumor and patients with a well-functioning implant without a pseudotumor. These results are consistent with the presence of a type IV hypersensitivity reaction with a predominance of type 1 Th cells in patients with a failed MoM hip implant with a pseudotumor. Results also showed that patients with a failed MoM hip implant with a pseudotumor had overall lower percentages of memory B cells than patients with a well-functioning implant without a pseudotumor. To the best of our knowledge, this is the first study to analyze the different lymphocyte subpopulations in peripheral blood of patients with a failed implant with a pseudotumor, specifically the different T cell subsets (Th1 and Th2), and compare these subpopulations with those in patients with a failed implant without a pseudotumor and patients with a well-functioning implant.
Because the purpose of the study was to analyze potential differences in the lymphocyte subpopulations resulting from the presence of a pseudotumor, patients were grouped exclusively based on the presence or absence of this adverse tissue reaction, regardless of their implant design (hip resurfacing or THA). Nevertheless, it is possible that the levels of Co and Cr ions were affected by the implant design and/or the indication for implant revision. The latter included pain, aseptic cup or femoral loosening, fibrosis ingrowth (one case), and metallosis (one case) in patients without a pseudotumor (Table 2). However, because of the limited number of patients in the study (especially in the group with a pseudotumor), patients with a hip resurfacing and those with a THA could not be analyzed separately. Interestingly, most patients without a pseudotumor had a failed hip resurfacing (only two of 12 had a failed THA) and most patients with a pseudotumor had a failed THA (two of seven had a failed hip resurfacing). Therefore, future studies with additional patients could include the analysis of the potential influence of implant design and indication of revision, although the scatter of the data with respect to implant design (identified on each figure through the use of different symbols) suggests that this parameter did not influence the results. Interestingly, the scatter of the lymphocyte data with respect to unilateral or bilateral implant suggests that this parameter also did not influence the results (data not shown). Nevertheless, increasing the number of patients would allow further subgrouping based on other potential confounding factors such as patient gender and age. Interestingly, significant differences in lymphocyte subpopulations were observed despite the relatively low number of patients, especially in the group with failed MoM implants with a pseudotumor, and statistical analysis (p values) suggests that increasing the number of patients is not likely to create additional differences in the lymphocyte subpopulations.
Although previous research has characterized T (specifically Th and Tc cells), B, and NK cell subpopulations in the peripheral blood of patients with a failed hip implant, there has been little attention to the state of lymphocyte differentiation (ie, naïve versus memory cells) as well as to the cytokine profile of T cells to determine the different subsets. A study by Granchi et al. evaluating lymphocyte subpopulations in the peripheral blood of patients with loosened hip implants containing CoCrMo alloy reported lymphopenia and more specifically a reduction in CD4+ (Th) and CD8+ (Tc) cells [12]. The authors interpreted these results as either the consequence of a toxic effect of the wear products released from the implant or a lymphocyte sequestration at the site of loosening attributable to a cell-mediated hypersensitivity reaction. In the present study, results showed overall lower percentages of memory T cells (specifically Th and Tc) as well as type 1 Th cells in patients with a failed MoM hip implant with a pseudotumor (memory cells in the type 1 Th cell subpopulation were not analyzed because of the limited number of channels available for cell markers on the flow cytometer). These results, like those of Granchi et al. [12], suggest either a toxic effect of the wear products or a sequestration of these cells at the implant site. Absolute cell counts in peripheral blood and histological analysis of periprosthetic tissues would help the interpretation of these results. However, the absence of differences in other cell subpopulations (T, B, and NK cells) further suggests a sequestration of the cells at the implant site rather than a toxic effect of the wear products. A local increase in the number of memory T cells and type 1 Th cells in the tissues would be consistent with a type IV hypersensitivity reaction. Interestingly, results of the present study also showed overall lower percentages of memory B cells in patients with a failed MoM hip implant with a pseudotumor than in patients with a well-functioning implant without a pseudotumor. These results may reflect the sequestration of memory B cells, possibly in secondary lymphoid organs or in periprosthetic tissues where lymphoid aggregates resembling tertiary lymphoid organs have been described in some patients with a MoM hip implant [29]. Interestingly, plasma cells have been found in periprosthetic tissues from failed MoM hip implants with a hypersensitivity reaction [38] and more specifically with a pseudotumor [32]. Although not characteristic of a type IV (delayed-type) hypersensitivity reaction, which is primarily T-cell mediated, the presence of plasma B cells (possibly originating from memory B cell differentiation) in periprosthetic tissues may reflect a role of these cells in the T cell-mediated reaction. Indeed, B cells have been reported to be involved in the regulation of immune responses via, for example, antigen presentation, cytokine production and the regulation of T cell differentiation [37]. Alternatively, the differences observed in the percentages of memory B cells may reflect the presence of a more complex combination of immune responses involving both T and B cells.
Although the absence of an additional marker such as CCR7 or CD62L (as a result of the limited number of channels available on the flow cytometer in the present study) did not allow the distinction of naïve and effector T cells nor did it allow the distinction between central memory and effector memory T cells, the group differences observed in the type 1 Th subpopulation suggest that T cells had previously undergone differentiation into the effector and effector memory phenotypes. Interestingly, results showed overall higher serum Co concentrations in patients with a failed MoM hip implant with a pseudotumor than in patients with a well-functioning implant without a pseudotumor. The comparison with patients with a failed hip implant without a pseudotumor was not statistically significant, but this was likely attributable to one patient (outlier) with a high Co concentration in the latter group. Overall, these results suggest a correlation between Co concentrations and the lymphocyte subpopulations. Although not sensitizers on their own, metal ions can form complexes with proteins [16, 26, 28, 40] and become antigenic to elicit metal hypersensitivity reactions. The pathomechanisms by which metals function as antigenic determinants remain poorly understood, but it is hypothesized that metal hapten-specific T lymphocytes recognize hapten-modified major histocompatibility (MHC)-peptide complexes [34]. So far, most studies have focused on the effects of nickel (Ni) ions on the adaptive immune response in the context of allergic contact dermatitis, and some studies have shown that Ni-specific T cell clones derived from peripheral blood showed a type 1 Th cytokine secretion pattern [22, 35]. Similarly, results of the present study suggest a correlation between a type 1 Th cell response and elevated Co ions in patients with a failed MoM hip implant with a pseudotumor, which would be consistent with a hypersensitivity reaction to elevated Co ions in these patients (the origin of these ions, however, remains unknown [eg, implant corrosion or degradation of local wear particles]). Surprisingly, although Kwon et al. [25] reported significantly higher Co and Cr serum levels in patients with a pseudotumor, there was no significant difference among the three experimental groups for Cr concentrations in the present study with the available number of patients. It should, however, be noted that serum measurements may be misleading because Cr is stored in red blood cells [27]. Furthermore, it is possible that increasing the number of patients may lead to additional differences, especially for Co concentrations between patients with a failed MoM hip implant with and without a pseudotumor, as per the statistical analysis.
Histological studies of tissues surrounding failed MoM hip implants with a pseudotumor have been reported [3, 10, 32]. For example, the study of Pandit et al. revealed extensive necrosis of dense connective tissue, a focally heavy macrophage and lymphocyte infiltration as well as the presence of plasma cells and eosinophils in some cases [32]. The observed reaction was somewhat similar to the aseptic lymphocyte-dominated vasculitis-associated lesion (ALVAL) reaction reported earlier by Willert et al. in tissues around MoM hip implants, but differences included a more diffuse lymphocyte infiltrate and the presence of extensive connective tissue necrosis [38]. A study by Campbell et al. of pseudotumor-like tissues reported low wear and high ALVAL scores in some patients with a suspected hypersensitivity reaction [3]. More recently, Grammatopoulos et al. showed heavy macrophage infiltrates and high ALVAL scores in tissues from patients with a pseudotumor [10]. All these studies revealed the presence of a hypersensitivity reaction, which is consistent with the findings of the present study. Nevertheless, none of the previous studies analyzed the specific Th subsets (Th1, Th2), thereby limiting the understanding of the underlying mechanisms. In an in vitro study, Hallab et al. demonstrated that metals increased the proliferation of lymphocytes from patients undergoing hip arthroplasty as well as the lymphocyte production of IFN-γ, indicating that a Th1 (as opposed to Th2) type response was likely associated with metal-induced reactivity [14]. These results are in agreement with the results of the present study showing overall lower percentages of circulating Th1 cells, which is consistent with a type IV hypersensitivity reaction. Although the present study focused on patients with a MoM hip implant, the findings may also apply to patients who have developed a pseudotumor with a non-MoM hip implant, especially in cases of trunnionosis, which are typically associated with elevated metal wear products.
In conclusion, results suggest the presence of a type IV hypersensitivity reaction, with a predominance of type 1 Th cells, in patients with a failed MoM hip implant with a pseudotumor. The lower percentages of memory T cells (specifically Th and Tc) as well as type 1 Th cells in peripheral blood of these patients could potentially become diagnostic biomarkers for the detection of pseudotumors. Finally, although implant design (hip resurfacing or THA) did not seem to affect the results, as suggested by the scatter of the data with respect to this parameter, future studies with additional patients could include the analysis of implant design in addition to correlations with histological analyses of specific Th subsets in periprosthetic tissues.
References
Almousa SA, Greidanus NV, Masri BA, Duncan CP, Garbuz DS. The natural history of inflammatory pseudotumors in asymptomatic patients after metal-on-metal hip arthroplasty. Clin Orthop Relat Res. 2013;471:3814–3821.
Bisschop R, Boomsma MF, Van Raay JJ, Tiebosch AT, Maas M, Gerritsma CL. High prevalence of pseudotumors in patients with a Birmingham Hip Resurfacing prosthesis: a prospective cohort study of one hundred and twenty-nine patients. J Bone Joint Surg Am. 2013;95:1554–1560.
Campbell P, Ebramzadeh E, Nelson S, Takamura K, De Smet K, Amstutz HC. Histological features of pseudotumor-like tissues from metal-on-metal hips. Clin Orthop Relat Res. 2010;468:2321–2327.
Chang EY, McAnally JL, Van Horne JR, Van Horne JG, Wolfson T, Gamst A, Chung CB. Relationship of plasma metal ions and clinical and imaging findings in patients with ASR XL metal-on-metal total hip replacements. J Bone Joint Surg Am. 2013;95:2015–2020.
Ebramzadeh E, Campbell P, Tan TL, Nelson SD, Sangiorgio SN. Can wear explain the histological variation around metal-on-metal total hips? Clin Orthop Relat Res. 2015;473:487–494.
Ebramzadeh E, Campbell PA, Takamura KM, Lu Z, Sangiorgio SN, Kalma JJ, De Smet KA, Amstutz HC. Failure modes of 433 metal-on-metal hip implants: how, why, and wear. Orthop Clin North Am. 2011;42:241–250, ix.
Fritz CO, Morris PE. Effect size estimates: current use, calculations, and interpretation. J Exp Psychol Gen. 2012;141:2–18.
Garbuz DS, Hargreaves BA, Duncan CP, Masri BA, Wilson DR, Forster BB. The John Charnley Award: Diagnostic accuracy of MRI versus ultrasound for detecting pseudotumors in asymptomatic metal-on-metal THA. Clin Orthop Relat Res. 2014;472:417–423.
Goodman SB. Wear particles, periprosthetic osteolysis and the immune system. Biomaterials. 2007;28:5044–5048.
Grammatopoulos G, Pandit H, Kamali A, Maggiani F, Glyn-Jones S, Gill HS, Murray DW, Athanasou N. The correlation of wear with histological features after failed hip resurfacing arthroplasty. J Bone Joint Surg Am. 2013;95:e81.
Grammatopolous G, Pandit H, Kwon YM, Gundle R, McLardy-Smith P, Beard DJ, Murray DW, Gill HS. Hip resurfacings revised for inflammatory pseudotumour have a poor outcome. J Bone Joint Surg Br. 2009;91:1019–1024.
Granchi D, Ciapetti G, Stea S, Cavedagna D, Bettini N, Bianco T, Fontanesi G, Pizzoferrato A. Evaluation of several immunological parameters in patients with aseptic loosening of hip arthroplasty. Chir Organi Mov. 1995;80:399–408.
Hallab NJ, Anderson S, Stafford T, Glant T, Jacobs JJ. Lymphocyte responses in patients with total hip arthroplasty. J Orthop Res. 2005;23:384–391.
Hallab NJ, Caicedo M, Finnegan A, Jacobs JJ. Th1 type lymphocyte reactivity to metals in patients with total hip arthroplasty. J Orthop Surg Res. 2008;3:6–17.
Hallab NJ, Mikecz K, Jacobs JJ. A triple assay technique for the evaluation of metal-induced, delayed-type hypersensitivity responses in patients with or receiving total joint arthroplasty. J Biomed Mater Res (Appl Biomater). 2000;53:480–489.
Hallab NJ, Mikecz K, Vermes C, Skipor A, Jacobs JJ. Differential lymphocyte reactivity to serum-derived metal-protein complexes produced from cobalt-based and titanium-based implant alloy degradation. J Biomed Mater Res. 2001;56:427–436.
Hart AJ, Sabah SA, Bandi AS, Maggiore P, Tarassoli P, Sampson B, Skinner AJ. Sensitivity and specificity of blood cobalt and chromium metal ions for predicting failure of metal-on-metal hip replacement. J Bone Joint Surg Br. 2011;93:1308–1313.
Hart AJ, Satchithananda K, Liddle AD, Sabah SA, McRobbie D, Henckel J, Cobb JP, Skinner JA, Mitchell AW. Pseudotumors in association with well-functioning metal-on-metal hip prostheses: a case-control study using three-dimensional computed tomography and magnetic resonance imaging. J Bone Joint Surg Am. 2012;94:317–325.
Hartmann A, Hanneman F, Lutzner J, Seidler A, Drexler H, Gunther KP, Schmitt J. Metal ion concentrations in body fluids after implantation of hip replacements with metal-on-metal bearing–systematic review of clinical and epidemiological studies. PLoS ONE. 2013;8:e70359.
Ivarsson A, Andersen MB, Johnson U, Lindwall M. To adjust or not adjust: nonparametric effect sizes, confidence intervals, and real-world meaning. Phsycol Sport Exerc. 2013;14:97–102.
Jacobs JJ, Skipor JJ, Campbell PA, Hallab NJ, Urban RM, Amstutz HC. Can metal levels be used to monitor metal-on-metal hip arthroplasties? J Arthroplasty. 2004;19(Suppl 3):59–65.
Kapsenberg ML, Wierenga EA, Stiekema FE, Tiggelman AM, Bos JD. Th1 lymphokine production profiles of nickel-specific CD4+T-lymphocyte clones from nickel contact allergic and non-allergic individuals. J Invest Dermatol. 1992;98:59–63.
Kwon YM, Glyn-Jones S, Simpson DJ, Kamali A, McLardy-Smith P, Gill HS, Murray DW. Analysis of wear of retrieved metal-on-metal hip resurfacing implants revised due to pseudotumours. J Bone Joint Surg Br. 2010;92:356–361.
Kwon YM, Lombardi AV, Jacobs JJ, Fehring TK, Lewis CG, Cabanela ME. Risk stratification algorithm for management of patients with metal-on-metal hip arthroplasty: consensus statement of the American Association of Hip and Knee Surgeons, the American Academy of Orthopaedic Surgeons, and the Hip Society. J Bone Joint Surg Am. 2014;96:e4.
Kwon YM, Ostlere SJ, McLardy-Smith P, Athanasou NA, Gill HS, Murray DW. “Asymptomatic” pseudotumors after metal-on-metal hip resurfacing arthroplasty: prevalence and metal ion study. J Arthroplasty. 2011;26:511–518.
Merritt K, Brown SA. Metal sensitivity reactions to orthopedic implants. Int J Dermatol. 1981;20:89–94.
Merritt K, Brown SA. Distribution of cobalt chromium wear and corrosion products and biologic reactions. Clin Orthop Relat Res. 1996;329(Suppl):S233–S243.
Merritt K, Rodrigo JJ. Immune response to synthetic materials. Sensitization of patients receiving orthopaedic implants. Clin Orthop Relat Res. 1996;326:71–79.
Mittal S, Revell M, Barone F, Hardie DL, Matharu GS, Davenport AJ, Martin RA, Grant M, Mosselmans F, Pynsent P, Sumathi VP, Addison O, Revell PA, Buckley CD. Lymphoid aggregates that resemble tertiary lymphoid organs define a specific pathological subset in metal-on-metal hip replacements. PLoS ONE. 2013;8:e63470.
Munro JT, Masri BA, Duncan CP, Garbuz DS. High complication rate after revision of large-head metal-on-metal total hip arthroplasty. Clin Orthop Relat Res. 2014;472:523–528.
Nakagawa S, Cuthill IC. Effect size, confidence interval and statistical significance: a practical guide for biologists. Biol Rev. 2007;82:591–605.
Pandit H, Glyn-Jones S, McLardy-Smith P, Gundle R, Whitwell D, Gibbons CL, Ostlere S, Athanasou N, Gill HS, Murray DW. Pseudotumours associated with metal-on-metal hip resurfacings. J Bone Joint Surg Br. 2008;90:847–851.
R Core Team. R: a language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing; 2014. Available at: http://www.R-project.org/. Accessed June 21, 2014.
Sinigaglia F. The molecular basis of metal recognition by T cells. J Invest Dermatol. 1994;102:398–401.
Sinigaglia F, Scheidegger D, Garotta G, Scheper R, Pletscher M, Lanzavecchia A. Isolation and characterization of Ni-specific T cell clones from patients with Ni-contact dermatitis. J Immunol. 1985;135:3929–3932.
Svensson O, Mathiesen EB, Reinholt FP, Blomgren G. Formation of a fulminant soft-tissue pseudotumor after uncemented hip arthroplasty. A case report. J Bone Joint Surg Am. 1988;70:1238–1242.
Watanabe R, Fujimoto M, Ishiura N, Kuwano Y, Nakashima H, Yazawa N, Okochi H, Sato S, Tedder TF, Tamaki K. CD19 expression in B cells is important for suppression of contact hypersensitivity. Am J Pathol. 2007;171:560–570.
Willert HG, Buchhorn GH, Fayyazi A, Flury R, Windler M, Köster G, Lohmann CH. Metal-on-metal bearings and hypersensitivity in patients with artificial hip joints. A clinical and histomorphological study. J Bone Joint Surg Am. 2005;87:28–36.
Williams DH, Greidanus NV, Masri BA, Duncan CP, Garbuz DS. Prevalence of pseudotumor in asymptomatic patients after metal-on-metal hip arthroplasty. J Bone Joint Surg Am. 2011;93:2164–2171.
Yang J, Merritt K. Production of monoclonal antibodies to study corrosion products of CO-CR biomaterials. J Biomed Mater Res. 1996;31:71–80.
Acknowledgments
We thank the Division of Orthopaedic Surgery at The Ottawa Hospital for assistance in obtaining the clinical samples; Elise Guira, Charles Guo, Béatrice V. Lavergne, Matthieu Lemay, and Xiao Xiang for their contribution to flow cytometry data acquisition; Dr Lionel Filion for technical expertise; and Dr Javier M Di Noia for constructive discussions on immunology.
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was supported by the Canada Research Chairs Program (IC). Two of the authors (IH, SJB) were recipients of a H. K. Uhthoff graduate fellowship.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
Clinical Orthopaedics and Related Research ® neither advocates nor endorses the use of any treatment, drug, or device. Readers are encouraged to always seek additional information, including FDA-approval status, of any drug or device prior to clinical use.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
This work was performed at the University of Ottawa, Ottawa, Ontario, Canada.
About this article

Cite this article
Catelas, I., Lehoux, E.A., Hurda, I. et al. Do Patients With a Failed Metal-on-metal Hip Implant With a Pseudotumor Present Differences in Their Peripheral Blood Lymphocyte Subpopulations?. Clin Orthop Relat Res 473, 3903–3914 (2015). https://doi.org/10.1007/s11999-015-4466-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-015-4466-8