
Abstract
Purpose of Review
To explore the sexual outcomes following the novel minimally invasive surgical procedures for benign prostatic hyperplasia- (BPH-) related lower urinary tract symptoms (LUTS), with an emphasis on ejaculatory dysfunction (EjD).
Recent Findings
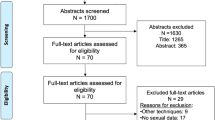
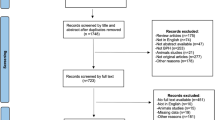
A database search with a 10-year time restriction was carried out until February 20, 2020 using MEDLINE through the PubMed Platform evaluating minimally invasive treatment modalities for BPH and their effect on EjD. After the article selection, we retrieved data for men randomized in 19 different studies with results in 40 separate published articles investigating minimally invasive BPH surgery and reporting EjD rates. To date, water vapor thermal therapy or Rezūm, prostatic urethral lift (PUL) or UroLift®, prostate artery embolization (PAE), and Aquablation showed acceptable rates (< 2%) of retrograde ejaculation by 1 year and had very low adverse events related to the procedure. Both PUL and Rezūm demonstrated lower rates when compared with PAE and Aquablation.
Summary
With comparable sexual side effect profiles postoperatively, clinicians may determine which therapeutic modality is optimal for patients based on efficacy and cost-benefit. Further randomized clinical trials are required to directly compare the effect of novel minimally invasive surgical procedures for BPH-related LUTS on ejaculation and sexual function.


Similar content being viewed by others

Data Availability
This is a literature review, all data is available through online peer reviewed articles.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Wei JT, Calhoun E, Jacobsen SJ. Urologic diseases in America project: benign prostatic hyperplasia. J Urol. 2005;173(4):1256–61.
Lim KB. Epidemiology of clinical benign prostatic hyperplasia. Asian J Urol. 2017;4(3):148–51.
Marra G, Sturch P, Oderda M, Tabatabaei S, Muir G, Gontero P. Systematic review of lower urinary tract symptoms/benign prostatic hyperplasia surgical treatments on men’s ejaculatory function: time for a bespoke approach? Int J Urol. 2016;23(1):22–35.
Briganti A, Naspro R, Gallina A, Salonia A, Vavassori I, Hurle R, et al. Impact on sexual function of holmium laser enucleation versus transurethral resection of the prostate: results of a prospective, 2-center, randomized trial. J Urol. 2006;175(5):1817–21.
Roehrborn CG, Rukstalis DB, Barkin J, Gange SN, Shore ND, Giddens JL, et al. Three year results of the prostatic urethral L.I.F.T. study. Can J Urol. 2015;22(3):7772–82.
Cantwell AL, Bogache WK, Richardson SF, Tutrone RF, Barkin J, Fagelson JE, et al. Multicentre prospective crossover study of the ‘prostatic urethral lift’ for the treatment of lower urinary tract symptoms secondary to benign prostatic hyperplasia. BJU Int. 2014;113(4):615–22.
McVary KT, Rogers T, Mahon J, Gupta NK. Is sexual function better preserved after water vapor thermal therapy or medical therapy for lower urinary tract symptoms due to benign prostatic hyperplasia? J Sex Med. 2018;15(12):1728–38.
Gratzke C, Barber N, Speakman MJ, Berges R, Wetterauer U, Greene D, et al. Prostatic urethral lift vs transurethral resection of the prostate: 2-year results of the BPH6 prospective, multicentre, randomized study. BJU Int. 2017;119(5):767–75.
McVary KT, Gange SN, Shore ND, Bolton DM, Cowan BE, Brown BT, et al. Treatment of LUTS secondary to BPH while preserving sexual function: randomized controlled study of prostatic urethral lift. J Sex Med. 2014;11(1):279–87.
Roehrborn CG. Prostatic urethral lift: a unique minimally invasive surgical treatment of male lower urinary tract symptoms secondary to benign prostatic hyperplasia. Urol Clin N Am. 2016;43(3):357–69.
Rukstalis D, Rashid P, Bogache WK, Tutrone RF, Barkin J, Chin PT, et al. 24-month durability after crossover to the prostatic urethral lift from randomised, blinded sham. BJU Int. 2016;118(Suppl 3):14–22.
Sønksen J, Barber NJ, Speakman MJ, Berges R, Wetterauer U, Greene D, et al. Prospective, randomized, multinational study of prostatic urethral lift versus transurethral resection of the prostate: 12-month results from the BPH6 study. Eur Urol. 2015;68(4):643–52.
•• Roehrborn CG, Barkin J, Gange SN, et al. Five year results of the prospective randomized controlled prostatic urethral L.I.F.T. study. Can J Urol. 2017;24(3):8802–13 The L.I.F.T. trial is the largest prospective, randomized trial we encountered for Prostatic urethral lift. Through 5 years of patient follow-up, we saw sexual function data in terms of MSHQ-EjD bother score and IIEF score.
Dixon C, Cedano ER, Pacik D, Vit V, Varga G, Wagrell L, et al. Efficacy and safety of Rezūm system water vapor treatment for lower urinary tract symptoms secondary to benign prostatic hyperplasia. Urology. 2015;86(5):1042–7.
McVary KT, Gange SN, Gittelman MC, et al. Erectile and ejaculatory function preserved with convective water vapor energy treatment of lower urinary tract symptoms secondary to benign prostatic hyperplasia: randomized controlled study. J Sex Med. 2016;13(6):924–33.
McVary KT, Gange SN, Gittelman MC, et al. Minimally invasive prostate convective water vapor energy ablation: a multicenter, randomized, controlled study for the treatment of lower urinary tract symptoms secondary to benign prostatic hyperplasia. J Urol. 2016;195(5):1529–38.
McVary KT, Roehrborn CG. Three-year outcomes of the prospective, randomized controlled Rezūm system study: convective radiofrequency thermal therapy for treatment of lower urinary tract symptoms due to benign prostatic hyperplasia. Urology. 2018;111:1–9, 1.
•• McVary KT, Rogers T, Roehrborn CG. Rezūm water wapor thermal therapy for lower urinary tract symptoms associated with benign prostatic hyperplasia: 4-year results from randomized controlled study. Urology. 2019;126:171–9 Paper extensively talked about Rezūm transurethral water vapor thermal therapy, its background and comparison to invasive BPH therapy such as TURP. It provided a large 4 year trial of Rezūm outcomes including IPSS score and sexual function outcomes.
Bhojani N, Bidair M, Zorn KC, Trainer A, Arther A, Kramolowsky E, et al. Aquablation for benign prostatic hyperplasia in large prostates (80-150 cc): 1-year results. Urology. 2019;129:1–7.
Bhojani N, Nguyen DD, Kaufman RP Jr, Elterman D, Zorn KC. Comparison of < 100 cc prostates and > 100 cc prostates undergoing aquablation for benign prostatic hyperplasia. World J Urol. 2019;37(7):1361–8.
• Desai M, Bidair M, Bhojani N, et al. WATER II (80-150 mL) procedural outcomes. BJU Int. 2019;123(1):106–12 The WATER II trial is discussed in this source, a prospective, multicenter study in which 101 men with prostates 80-150cc underwent Aquablation for BPH. This study is very open about benefits as well as complications from this procedure and provided insight into this treatment for the review.
Desai MM, Singh A, Abhishek S, Laddha A, Pandya H, Ashrafi AN, et al. Aquablation therapy for symptomatic benign prostatic hyperplasia: a single-centre experience in 47 patients. BJU Int. 2018;121(6):945–51.
Gilling P, Anderson P, Tan A. Aquablation of the prostate for symptomatic benign prostatic hyperplasia: 1-year results. J Urol. 2017;197(6):1565–72.
Gilling P, Barber N, Bidair M, Anderson P, Sutton M, Aho T, et al. WATER: a double-blind, randomized, controlled trial of Aquablation(®) vs transurethral resection of the prostate in benign prostatic hyperplasia. J Urol. 2018;199(5):1252–61.
Gilling P, Reuther R, Kahokehr A, Fraundorfer M. Aquablation - image-guided robot-assisted waterjet ablation of the prostate: initial clinical experience. BJU Int. 2016;117(6):923–9.
•• Gilling PJ, Barber N, Bidair M, et al. Randomized controlled trial of Aquablation versus transurethral resection of the prostate in benign prostatic hyperplasia: one-year outcomes. Urology. 2019;125:169–73 This study compared Aquablation to TURP with randomized control trial, double-blinding patients to receive either treatment and comparing results. This was important in assessing Aquablation's efficacy and safety. Overall, the study determined that this minimally invasive BPH therapy gave similar results with similar complication rate as TURP.
Plante M, Gilling P, Barber N, Bidair M, Anderson P, Sutton M, et al. Symptom relief and anejaculation after Aquablation or transurethral resection of the prostate: subgroup analysis from a blinded randomized trial. BJU Int. 2019;123(4):651–60.
Yafi FA, Tallman CT, Seard ML, Jordan ML. Aquablation outcomes for the U.S. cohort of men with LUTS due to BPH in large prostates (80-150 cc). Int J Impot Res. 2018;30(5):209–14.
Abt D, Hechelhammer L, Müllhaupt G, et al. Comparison of prostatic artery embolisation (PAE) versus transurethral resection of the prostate (TURP) for benign prostatic hyperplasia: randomised, open label, non-inferiority trial. Bmj. 2018;361:k2338.
Bagla S, Martin CP, van Breda A, Sheridan MJ, Sterling KM, Papadouris D, et al. Early results from a United States trial of prostatic artery embolization in the treatment of benign prostatic hyperplasia. J Vasc Interv Radiol. 2014;25(1):47–52.
Carnevale FC, da Motta-Leal-Filho JM, Antunes AA, Baroni RH, Marcelino ASZ, Cerri LMO, et al. Quality of life and clinical symptom improvement support prostatic artery embolization for patients with acute urinary retention caused by benign prostatic hyperplasia. J Vasc Interv Radiol. 2013;24(4):535–42.
Carnevale FC, Iscaife A, Yoshinaga EM, Moreira AM, Antunes AA, Srougi M. Transurethral resection of the prostate (TURP) versus original and PErFecTED prostate artery embolization (PAE) due to benign prostatic hyperplasia (BPH): preliminary results of a single center, prospective, Urodynamic-Controlled Analysis. Cardiovasc Intervent Radiol. 2016;39(1):44–52.
Carnevale FC, Moreira AM, Harward SH, Bhatia S, de Assis AM, Srougi M, et al. Recurrence of lower urinary tract symptoms following prostate artery embolization for benign hyperplasia: single center experience comparing two techniques. Cardiovasc Intervent Radiol. 2017;40(3):366–74.
de Assis AM, Moreira AM, de Paula Rodrigues VC, Yoshinaga EM, Antunes AA, Harward SH, et al. Prostatic artery embolization for treatment of benign prostatic hyperplasia in patients with prostates > 90 g: a prospective single-center study. J Vasc Interv Radiol. 2015;26(1):87–93.
Hechelhammer L, Müllhaupt G, Mordasini L, Markart S, Güsewell S, Betschart P, et al. Predictability and inducibility of detachment of prostatic central gland tissue after prostatic artery embolization: post hoc analysis of a randomized controlled trial. J Vasc Interv Radiol. 2019;30(2):217–24.
Isaacson AJ, Raynor MC, Yu H, Burke CT. Prostatic artery embolization using embosphere microspheres for prostates measuring 80-150 cm(3): early results from a US trial. J Vasc Interv Radiol. 2016;27(5):709–14.
Pisco J, Campos Pinheiro L, Bilhim T, Duarte M, Rio Tinto H, Fernandes L, et al. Prostatic arterial embolization for benign prostatic hyperplasia: short- and intermediate-term results. Radiology. 2013;266(2):668–77.
• Pisco JM, Bilhim T, Costa NV, et al. Randomised clinical trial of prostatic artery embolisation versus a sham procedure for benign prostatic hyperplasia. Eur Urol. 2020;77(3):354–62 Source discussed prostatic artery embolization (PAE), one of the minimally invasive BPH procedures discussed in the review, compared PAE to sham, illustrating its efficacy in improving LUTS in men vs placebo.
Salem R, Hairston J, Hohlastos E, Riaz A, Kallini J, Gabr A, et al. Prostate artery embolization for lower urinary tract symptoms secondary to benign prostatic hyperplasia: results from a prospective FDA-approved investigational device exemption study. Urology. 2018;120:205–10.
Torres D, Costa NV, Pisco J, Pinheiro LC, Oliveira AG, Bilhim T. Prostatic artery embolization for benign prostatic hyperplasia: prospective randomized trial of 100-300 μm versus 300-500 μm versus 100- to 300-μm + 300- to 500-μm embospheres. J Vasc Interv Radiol. 2019;30(5):638–44.
Wang MQ, Guo LP, Zhang GD, Yuan K, Li K, Duan F, et al. Prostatic arterial embolization for the treatment of lower urinary tract symptoms due to large (>80 mL) benign prostatic hyperplasia: results of midterm follow-up from Chinese population. BMC Urol. 2015;15:33–3.
Wang MQ, Zhang JL, Xin HN, Yuan K, Yan J, Wang Y, et al. Comparison of clinical outcomes of prostatic artery embolization with 50-μm plus 100-μm polyvinyl alcohol (PVA) particles versus 100-μm PVA particles alone: a prospective randomized trial. J Vasc Interv Radiol. 2018;29(12):1694–702.
Westwood J, Geraghty R, Jones P, Rai BP, Somani BK. Rezum: a new transurethral water vapour therapy for benign prostatic hyperplasia. Ther Adv Urol. 2018;10(11):327–33.
Lokeshwar SD, Harper BT, Webb E, Jordan A, Dykes TA, Neal Jr DE, et al. Epidemiology and treatment modalities for the management of benign prostatic hyperplasia. Transl Androl Urol. 2019;8(5):529–39.
Garcia C, Chin P, Rashid P, Woo HH. Prostatic urethral lift: a minimally invasive treatment for benign prostatic hyperplasia. Prostate Int. 2015;3(1):1–5.
Wang R. UroLift: a new surgical treatment for BPH without sexual side effect. Transl Androl Urol 2014;3(S1):AB02. https://doi.org/10.3978/j.issn.2223-4683.2014.s002
Jones P, Rai BP, Aboumarzouk O, Somani BK. UroLift: a new minimally-invasive treatment for benign prostatic hyperplasia. Ther Adv Urol. 2016;8(6):372–6.
JP MW, Bilhim TA, Carnevale FC, et al. Society of Interventional Radiology Multisociety consensus position statement on prostatic artery embolization for treatment of lower urinary tract symptoms attributed to benign prostatic hyperplasia: from the Society of Interventional Radiology, the Cardiovascular and Interventional Radiological Society of Europe, Société Française de Radiologie, and the British Society of Interventional Radiology: Endorsed by the Asia Pacific Society of Cardiovascular and Interventional Radiology, Canadian Association for Interventional Radiology, Chinese College of Interventionalists, Interventional Radiology Society of Australasia, Japanese Society of Interventional Radiology, and Korean Society of Interventional Radiology. J Vasc Interv Radiol. 2019;30(5):627–37 e621.
Challacombe B, Sabharwal T. Prostate artery embolisation for benign prostatic hyperplasia. BMJ. 2018;361:k2537.
Carnevale FC, Moreira AM, Antunes AA. The “PErFecTED technique”: proximal embolization first, then embolize distal for benign prostatic hyperplasia. Cardiovasc Intervent Radiol. 2014;37(6):1602–5.
Sturch P, Woo HH, McNicholas T, Muir G. Ejaculatory dysfunction after treatment for lower urinary tract symptoms: retrograde ejaculation or retrograde thinking? BJU Int. 2015;115(2):186–7.
Code Availability
None used
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
No conflicts of interest or disclosures
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Benign Prostatic Hyperplasia
Electronic Supplementary Material
ESM 1
(DOC 63 kb)
Rights and permissions
About this article

Cite this article
Lokeshwar, S.D., Valancy, D., Lima, T.F.N. et al. A Systematic Review of Reported Ejaculatory Dysfunction in Clinical Trials Evaluating Minimally Invasive Treatment Modalities for BPH. Curr Urol Rep 21, 54 (2020). https://doi.org/10.1007/s11934-020-01012-y
Accepted:
Published:
DOI: https://doi.org/10.1007/s11934-020-01012-y