
Abstract
Purpose of the Review
Non-alcoholic fatty liver disease (NAFLD) and heart failure (HF) are two chronic diseases that have become important global public health problems. This narrative review provides a comprehensive overview of the association between NAFLD and increased risk of new-onset HF, briefly discusses the putative biological mechanisms linking these two conditions, and summarizes targeted pharmacotherapies for NAFLD that might also beneficially affect cardiac complications leading to new-onset HF.
Recent Findings
Recent observational cohort studies supported a significant association between NAFLD and the long-term risk of new-onset HF. Notably, this risk remained statistically significant even after adjustment for age, sex, ethnicity, adiposity measures, pre-existing type 2 diabetes and other common cardiometabolic risk factors. In addition, the risk of incident HF was further increased with more advanced liver disease, especially with higher severity of liver fibrosis. There are multiple potential pathophysiological mechanisms by which NAFLD (especially in its more advanced forms) may increase the risk of new-onset HF.
Summary
Because of the strong link existing between NAFLD and HF, more careful surveillance of these patients will be needed. However, further prospective and mechanistic studies are required to better decipher the existing but complex link between NAFLD and risk of new-onset HF.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Congestive heart failure (HF) and non-alcoholic fatty liver disease (NAFLD) are two growing major clinical and public health problems globally [1, 2].
Convincing evidence indicates that the clinical burden of NAFLD is not only restricted to its liver-related complications [such as non-alcoholic steatohepatitis (NASH), advanced fibrosis, cirrhosis or hepatocellular carcinoma] but also adversely affects multiple extrahepatic organs and systems, including the heart and vascular system [3,4,5]. In particular, NAFLD is not only associated with a substantially higher risk of developing major adverse cardiovascular events (that are the leading cause of mortality in people with NAFLD) [6, 7], but is also associated with a higher risk of cardiac arrhythmias (mainly atrial fibrillation) and myocardial remodeling, which may precede and/or promote the development of new-onset HF [8, 9•, 10]. So, because of the close link between NAFLD and HF, more careful surveillance of these patients is needed.
This narrative review article focuses on the most recent observational cohort studies supporting a significant association between NAFLD and the risk of developing new-onset HF. We also discuss the epidemiology and diagnosis of NAFLD, the putative biological mechanisms underpinning the association between NAFLD and risk of new-onset HF, and briefly summarize targeted pharmacotherapies for NAFLD or NASH that may also beneficially affect cardiac complications leading to new-onset HF over time.
Epidemiology and Diagnosis of NAFLD
NAFLD Epidemiology
NAFLD has become the most common cause of chronic liver disease worldwide, affecting up to nearly 30% of adults in the general population [11]. The prevalence of non-alcoholic steatohepatitis (NASH) in the general adult population is challenging to estimate precisely [12]. Based on the currently available data, the global prevalence of NASH is estimated between ~ 2% and 6% in the general adult population [11]. The global prevalence rates of NAFLD and NASH markedly increase in specific patient populations, such as patients who are obese or have type 2 diabetes mellitus (T2DM) [3]. For instance, in a 2019 systematic review and meta-analysis including 80 observational studies for a total of approximately 49,500 individuals with T2DM, Younossi et al. reported that the estimated global prevalence of NAFLD (as detected by liver ultrasonography or magnetic resonance spectroscopy) amongst patients with T2DM was 55.5% (95% CI 47–64%); studies from Europe reported the highest prevalence (68% [95% CI 62–73%]) [13]. In addition, the authors also found that the global prevalence rates for NASH and advanced fibrosis (stage ≥ F3 on liver histology) among T2DM patients were 37% and 17%, respectively [13]. In a 2023 meta-analysis including 151 observational studies for a total of 101,028 overweight and obese individuals, Quek et al. reported that in the overweight population the estimated global prevalence of NAFLD and NASH was approximately 70% and 33%, respectively [14]. Similarly, in the obese population the global prevalence of NAFLD and NASH was 75% and 34% [14]. Additionally, the estimated global prevalence of advanced fibrosis was around 7% among overweight and obese individuals [14]. Differences in terms of the prevalence of NAFLD may also exist in relation to sex and ethnicity. For example, the global prevalence of NAFLD is higher in men than in premenopausal women, but tends to be comparable between men and postmenopausal women of similar age [15]. Hispanic and Caucasian individuals are more likely to have NAFLD, while African Americans are at a lower risk for NAFLD [16].
Although detailed information about the incidence rates of NAFLD is currently lacking, a recent systematic review and meta-analysis of 63 observational studies (~ 1,200,000 participants) showed that the global incidence of NAFLD was about 46 cases per 1000 person-years, with higher incidence rates observed in males and overweight/obese individuals compared to females and those of normal body weight [17].
NAFLD Diagnosis
The NAFLD acronym includes a spectrum of progressive steatotic liver conditions, ranging from non-alcoholic fatty liver (NAFL) to NASH, advanced fibrosis and cirrhosis [12, 18•]. NAFL is defined histologically by the presence of macrovesicular steatosis in ≥ 5% of hepatocytes without evidence of hepatocyte injury (ballooning) in persons with no or little alcohol consumption [12, 18•]. NASH is defined histologically by the presence of ≥ 5% steatotic hepatocytes with coexisting inflammation and hepatocyte ballooning, independent of liver fibrosis [12, 18•]. Advanced fibrosis refers to histologic stages F3-F4 on the Kleiner’s classification that is the presence of either “bridging fibrosis” (F3 stage) or cirrhosis (F4 stage) [12, 18•, 19]. Currently, the diagnosis of NAFLD is always a diagnosis of exclusion that is mainly based on the following criteria: (a) presence of hepatic steatosis (detected by serum biomarkers/scores, imaging techniques or liver histology); (b) no significant alcohol consumption (conventionally defined as < 20 g/day for women and < 30 g/day for men); and (c) no other secondary causes of hepatic steatosis (e.g., virus, hemochromatosis, autoimmune hepatitis, alpha-1 anti-trypsin deficiency, Wilson’s disease or use of potentially hepatotoxic drugs) [12, 18•].
In 2020, international experts have proposed to change the terminology and definition of this common metabolic liver disease, switching from NAFLD to metabolic dysfunction-associated fatty liver disease (MAFLD) to overcome the intrinsic limitations of the NAFLD definition and to further highlight the pathogenic role of metabolic dysfunction in the development and progression of this liver disease [20, 21]. Based on this newly-proposed definition, the diagnosis of MAFLD is based on the coexistence of hepatic steatosis (detected by serum biomarkers/scores, imaging techniques or liver biopsy) and at least one of the following three metabolic risk abnormalities: (a) overweight or obesity, (b) T2DM, or (c) metabolic dysregulation (defined by the presence of at least two metabolic risk factors, typically featuring the metabolic syndrome, amongst increased waist circumference, high plasma triglycerides, low HDL cholesterol level, hypertension, prediabetes, insulin resistance [assessed by homeostasis model assessment of insulin resistance (HOMA-IR score) ≥ 2.5] or systemic low-grade inflammation [evaluated by a plasma high-sensitive C reactive protein level > 2 mg/L]) [20, 21]. Emerging data suggested that adopting the MAFLD definition (instead of NAFLD definition) more individuals with liver damage may be identified [22]. However, since there is not a global support for the newly proposed MAFLD definition yet, we have decided to use in this narrative review the term NAFLD instead of that of MAFLD.
Liver biopsy remains the gold standard method for diagnosing and staging NAFLD, as it is the only diagnostic method, which is able to differentiate between NAFL and NASH and to quantify liver fibrosis [12, 18•, 23, 24]. However, liver biopsy is invasive, patient-unfriendly, and potentially risky [12, 18•, 23, 24]. For these reasons, liver biopsy assessment is not used routinely for the diagnosis of NAFLD, but it is used sparingly in clinical practice [12, 18•, 23, 24]. Conventional liver ultrasonography is the recommended first-line imaging technique for the diagnosis of NAFLD (hepatic steatosis) in clinical practice [12, 18•, 23, 24]. This imaging method is inexpensive, patient friendly, and largely spread in several clinical settings [12, 18•, 23, 24]. However, liver ultrasonography is operator-dependent [12, 18•, 23, 24] and lacks sufficient sensitivity for accurately quantifying or monitoring changes in hepatic fat content [25]. Controlled attenuation parameter (CAP), in combination with vibration-controlled transient elastography (Fibroscan®), is another non-invasive method that can be used for the diagnosis of hepatic steatosis [26]. However, at present, the specific CAP thresholds for detecting hepatic steatosis are not yet established [23]. Computed tomography offers a semi-quantitative imaging method for detecting hepatic steatosis, but it also lacks sufficient sensitivity for smaller amounts of liver fat and exposes the subject to high radiation levels [12, 18•, 23]. Magnetic resonance imaging–proton density fat fraction (MRI-PDFF) and proton magnetic resonance spectroscopy have emerged as the two most accurate and reproducible imaging methods for the non-invasive quantification of liver fat content [24, 27]. However, both imaging methods are expensive and used only in clinical research or tertiary care centers [12, 18•, 23, 24]. Vibration-controlled transient elastography (Fibroscan®) is the most widely used method for non-invasively staging hepatic fibrosis in clinical practice, since it is broadly validated, patient-friendly and also provides real-time results [12, 18•, 23, 24]. Fibroscan® has a good reproducibility and excellent performance in identifying advanced fibrosis or cirrhosis [12, 18•, 23, 24]. However, its diagnostic performance is reduced by presence of severe obesity [12, 18•, 23, 24].
NAFLD as Risk Factor for New-Onset HF
More than 10 years ago, the Framingham Heart Study and some other large community-based cohort studies from UK and Finland reported that higher serum gamma-glutamyltransferase concentrations within the "normal" range (as a surrogate marker of NAFLD) were associated with a higher risk of new-onset HF events, independently of daily alcohol consumption and a wide range of common risk factors for HF [28,29,30].
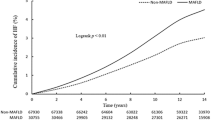
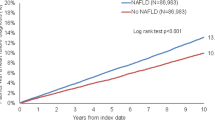
In 2021, using a nationwide health screening database of about 9 million middle-aged Korean individuals followed for a median of 10.1 years, Lee et al. reported that NAFLD (defined as fatty liver index [FLI] ≥ 30) was significantly associated with a higher risk of incident HF events (adjusted hazard ratio [HR] 1.61, 95% confidence interval [CI] 1.55–1.67). This association was independent of age, sex, household income, residential area, the Charlson’s comorbidity index, smoking history, physical activity, and estimated glomerular filtration rate [31]. Most interestingly, in a nationwide cohort study of 10,422 Swedish adult individuals with biopsy-confirmed NAFLD and nearly 50,000 matched control subjects who were followed for a median of 13.6 years, Simon et al. [32] examined the risk of incident major adverse cardiovascular events (including also the risk of new-onset HF), according to the presence and histological severity of NAFLD. These authors found that compared with matched population controls, patients with NAFLD had a significantly higher incidence of HF (adjusted HR 1.75, 95% CI 1.63–1.87) even after adjustment for common cardiometabolic risk factors. Rates of incident HF events increased progressively with worsening NAFLD severity, with the highest incidence rates observed with non-cirrhotic fibrosis (adjusted HR 2.04, 95% CI 1.66–2.51) and cirrhosis (adjusted HR 2.83, 95% CI 2.08–3.85) [32].
In 2023, we included the aforementioned longitudinal cohort studies in a comprehensive meta-analysis that incorporated a total of 11 observational cohort studies with more than 11 million middle-aged individuals from different countries and captured nearly 98,000 cases of new-onset HF over a median of 10-year follow-up [33•]. As shown in the forest plot of Fig. 1, our meta-analysis concluded that the presence of NAFLD (diagnosed by blood biomarkers/scores, International Classification of Diseases (ICD)-10 codes, imaging techniques, or liver histology) was significantly associated with a 1.5-fold higher risk of developing new-onset HF (pooled random-effects HR 1.50, 95% CI 1.34–1.67; p < 0.001). This risk remained significant even after adjustment for age, sex, ethnicity, adiposity measures, hypertension, T2DM and other cardiometabolic risk factors. In addition, the magnitude of this risk remained unchanged even when the comparison was stratified by study country, follow-up duration, modality of HF diagnosis or methods used for diagnosing NAFLD. Notably, the risk of incident HF appeared to increase further with greater severity of NAFLD, especially with higher fibrosis stage [33•]. These latter observations are also supported by recent longitudinal studies showing that increased fibrosis-4 (FIB-4) index or other non-invasive liver fibrosis scores were associated with a higher risk of hospitalization for HF (adjusted HR 2.09, 95% CI 1.86–2.35) in a large real-word cohort of patients with established NAFLD or NASH [34]. Similarly, these results are supported by data from cohorts of patients with chronic HF, especially in HF patients with preserved ejection fraction (HFpEF) [35, 36]. However, further studies are needed to prove whether the severity of liver disease in NAFLD further amplifies the risk of new-onset HF.

Forest plot and pooled estimates of the effect of NAFLD on the risk of new-onset heart failure in eleven eligible cohort studies, stratified by methodologies used for the diagnosis of NAFLD. Data are reproduced from Mantovani et al. [33•]
Interestingly, after the publication of our updated meta-analysis [33•], Simon et al. examined the association between NAFLD and risk of developing new-onset HF in a nationwide cohort study of 699 Swedish obese children and young adults ≤ 25 years old with histologically confirmed NAFLD and 3,353 control subjects matched for age, sex, calendar year and county [37]. Over a median follow-up of 16.6 years, these authors found that compared with matched population controls, young patients with NAFLD had significantly higher incidence rates of congestive HF (adjusted HR 3.89, 95% CI 1.20–12.6) that appeared to be further augmented with NASH. These findings suggest that research to better characterize cardiovascular risk also in obese children and young adults with NAFLD should be prioritized [37].
Based on the currently available data, there seems little doubt that NAFLD is associated with an increased incidence of HF, an association that has been consistently replicated across different countries, as well as across different methods used for NAFLD diagnosis. To date, little is known on the association between NAFLD and different HF phenotypes (i.e., HF with reduced left ventricular ejection fraction [HFrEF] vs. preserved left ventricular ejection fraction [HFpEF]) as most of the published cohort studies did not have any echocardiographic data to categorize LV ejection fraction. The only cohort study that examined this issue showed that the association of NAFLD with the risk of developing HF was stronger for HFpEF than for HFrEF [38]. This is also in line with previously published studies reporting a significant association of NAFLD with LV hypertrophy and subclinical LV diastolic dysfunction in the context of preserved ejection fraction [39, 40]. Notably, the association of NAFLD with impaired cardiac structure and function remained statistically significant even after adjusting for obesity and other common cardiometabolic risk factors, thus suggesting a possible direct pathophysiological link between NAFLD and the risk of HFpEF. Unlike HFrEF, HFpEF has distinct clinical phenotypes. Along with the obese-diabetic phenotype, which is the one often encountered in clinical practice, clinicians should be also aware of the potential coexistence of NAFLD or NASH in the context of HFpEF.
Collectively, therefore, the healthcare professionals should be aware that the risk of new-onset HF is moderately greater among patients with NAFLD, especially among those with fibrotic NASH. This further highlights the need for a multidisciplinary and holistic approach to manage both liver disease and cardiometabolic risk in patients with NAFLD [41]. However, as discussed in a later section, whether NAFLD is an independent risk factor for new-onset HF or it is simply a bystander that shares common cardiometabolic risk factors is still controversial.
Putative Mechanisms Linking NAFLD to Risk of New-Onset HF
Although the exact pathophysiological mechanisms by which NAFLD may increase the risk of new-onset HF are not fully understood, it is possible to speculate that several factors play a key role. A detailed description of the putative mechanisms linking NAFLD to increased risk of HF has been extensively discussed elsewhere [9•]. Briefly, multiple factors related with coexisting obesity, T2DM or directly linked to intestinal dysbiosis might modulate the association between NAFLD and the risk of new-onset HF [8, 9•, 42]. For instance, systemic low-grade inflammation that typically characterizes metabolic disorders, such as obesity, T2DM and NAFLD [42], may contribute to the development of accelerated coronary atherosclerosis, as well as to the development of myocardial remodeling and hypertrophy, thereby promoting the onset of HF [8, 9•]. Specifically, proinflammatory cytokines, such as interleukin (IL)-1, IL-6, tumor necrosis factor-alpha or transforming growth factor-beta, may promote myocardial remodeling, myolysis and fibrosis via several mechanisms [43,44,45,46]. In this regard, accumulating evidence indicates a potential beneficial effect of IL-1 blockade in terms of cardiac contractility, quality-of-life, and treadmill exercise time, as well as in terms of reduction in serum NT-proBNP concentrations in patients with established HF [47]. Dietary fatty acids may also promote systemic low-grade inflammation and even alter gut microbiota composition [48,49,50]. On this subject, a high-fat Western diet induces endotoxaemia, which, in turn, promotes low-grade inflammation and production of specific microbial metabolites, including trimethylamine (TMA) or TMA N-oxide (TMAO) [48]. Interestingly, higher circulating levels of TMA and TMAO are associated with the future risk of adverse cardiovascular outcomes [51].
Experimental and clinical studies also support the production of specific mediators from the steatotic/inflamed/fibrotic liver in patients with NAFLD (Fig. 2) [52, 53]. When NAFLD occurs, liver fat and inflammation progress (NASH) and advanced fibrosis develops. In this context, many alterations take place into the liver, resulting in increased production of atherogenic lipids, exacerbation of systemic and hepatic insulin resistance, activation of the renin-angiotensin-aldosterone system and release of several proinflammatory cytokines, pro-oxidant factors and thrombogenic molecules (e.g., IL-6, factor VII, plasminogen activator inhibitor-1, endotelin-1) [8, 9•, 52, 53]. According to the lipotoxicity theory [54], it is likely that there is a pathogenic “cross-talk” between NAFLD and the expanded and inflamed visceral adipose tissue. From this perspective, epicardial adipose tissue (EAT) thickness may represent a marker of the cumulative effects of NAFLD and insulin resistance in the setting of ectopic fat accumulation. It has been shown that the severity of NAFLD is significantly associated with increased EAT thickness, which is in turn associated with LV diastolic dysfunction [55, 56]. In patients with NAFLD, all these factors may also have an adverse effect on the long-term risk of cardiac complications, including the risk of new-onset HF, especially HFpEF [8, 9•].

Putative pathophysiological mechanisms underlying the association between NAFLD and risk of new-onset heart failure. In NAFLD, many alterations occur within the liver, resulting in an increased production of proinflammatory cytokines, worsening of insulin resistance, promotion of a more pronounced atherogenic lipid profile, exacerbation of oxidative stress, activation of the renin–angiotensin-aldosterone system (RAAS) and alteration of gut microbiota, accompanied by an increased production of bioactive microbial metabolites. All these factors, along with specific genetic polymorphisms, may lead microvascular dysfunction, myocardial remodeling and hypertrophy, as well as cardiac arrhythmias, thereby resulting in an increased long-term risk of new-onset heart failure
Finally, some genetic polymorphisms predisposing individuals to advanced forms of NAFLD, such as patatin-like phospholipase domain-containing protein-3 (PNPLA3) and trans-membrane 6 super family-2 (TM6SF2), may modulate the association between NAFLD and the risk of cardiovascular disease [8, 9•, 57]. For instance, the PNPLA3 rs738409 C > G and TM6SF2 rs58542926 C > T are two genotypes that increase the risk of developing advanced forms of NAFLD [57], but may also promote the reduction in plasma very-low-density lipoprotein (VLDL) concentrations, thereby reducing the risk of cardiovascular disease in patients with NAFLD [57]. However, at present, it is uncertain if the PNPLA3 rs738409 C > G or TM6SF2 rs58542926 C > T genetic variants might also modulate the association between NAFLD and the risk of new-onset HF [9•].
Pharmacological Treatments that Beneficially Affect NAFLD and HF
Lifestyle modifications, which include hypocaloric diet and physical activity to achieve weight loss, are the cornerstone of treatment for NAFLD [5, 12]. A weight loss of ≥ 10% is associated with resolution of NASH, and significant improvement of liver fibrosis. Moderate weight loss (ranging from ~ 5% to 10%) may also improve various histologic components of the NAFLD activity score [58]. For such reason, the European and American practice guidelines for the management of NAFLD recommend that in overweight or obese patients with NAFLD, a 5–10% weight loss is the goal of most lifestyle interventions [12, 18•]. Among the different therapeutic options to lose body weight, bariatric surgery is currently the most effective strategy [59]. In severely obese patients with NAFLD, bariatric surgery can improve all histological features of NASH, including also liver fibrosis [59]. In a systematic review and meta-analysis of 32 cohort studies including 3,093 liver biopsy specimens, Lee et al. reported that bariatric surgery procedures resulted in histologic resolution of hepatic steatosis in ~ 65% of patients, hepatocyte ballooning in ~ 75% of cases and liver fibrosis in ~ 40% of cases [60]. In a recent multicentre, open-label, randomised clinical trial enrolling 288 severely obese patients with biopsy-proven NASH, who were randomly assigned to lifestyle modification plus medical care, Roux-en-Y gastric bypass, or sleeve gastrectomy, Verrastro et al. reported that the percentage of patients who met the histological resolution of NASH without fibrosis worsening, at 1-year follow-up, was significantly greater in the Roux-en-Y gastric bypass group (56%) and the sleeve gastrectomy group (57%) when compared with the nonsurgical group (16%) [61]. Among patients with NASH and obesity, bariatric surgery, compared with nonsurgical management, was also associated with a significantly lower risk of major adverse cardiovascular and liver-related outcomes [62, 63]. Emerging evidence indicates that bariatric surgery might be also considered for treating severely obese patients with advanced HF [9•], as this surgical procedure is able to improve cardiac structure and function [64,65,66].
Currently, there are no approved pharmacotherapies for NAFLD and its more advanced forms. The current scientific guidelines for the NAFLD management recommend the use of pioglitazone in patients with biopsy-proven NASH and/or advanced fibrosis, regardless of the presence or absence of T2DM [5, 12, 18•]. However, safety concerns due to moderate weight gain, fluid retention and peripheral oedema limit the use of pioglitazone in clinical practice that should be avoided in patients at high risk of HF. Indeed, current HF guidelines do not recommend the use of pioglitazone in patients with symptomatic HF or in those at high risk of HF [1].
Growing clinical evidence indicate that glucagon-like peptide-1 receptor agonists (GLP-1RAs) and sodium-glucose cotransporter-2 (SGLT-2) inhibitors have hepatoprotective effects [67,68,69, 70•], as well as beneficial effects on the long-term risk of adverse cardiovascular and kidney outcomes, regardless of T2DM status [71, 72]. GLP-1RAs are approved for the treatment of T2DM. These glucose-lowering agents improve insulin resistance and promote body weight loss. For such reason, GLP-1RAs have been extensively studied in patients with NAFLD or NASH. A recent meta-analysis of 11 placebo-controlled or active-controlled phase-2 randomized controlled trials (RCTs) (involving a total of 936 middle-aged individuals) showed that compared with placebo or reference therapy, treatment with GLP-1RAs for a median of 26 weeks was associated with a significant reduction in the absolute percentage of liver fat content assessed by magnetic resonance-based techniques (pooled weighted mean difference: -3.92%, 95% CI -6.27% to -1.56%) (Fig. 3, panel A) and serum liver enzyme levels, as well as with greater histological resolution of NASH without worsening of fibrosis (pooled random-effects odds ratio 4.06, 95% CI 2.52–6.55; for subcutaneous liraglutide and semaglutide only) [68]. In this meta-analysis, GLP-1RA treatment was not associated with an improvement in liver fibrosis on histology [68]. GLP-1RAs have also beneficial effects on all-cause mortality and cardiovascular and kidney outcomes. For instance, a 2019 meta-analysis of seven RCTs for a total of nearly 56,000 individuals with T2DM showed a significant reduction of the risk of major adverse cardiovascular events (defined as cardiovascular mortality, nonfatal stroke or myocardial infarction), all-cause mortality, hospital admission for HF and worsening of kidney function [71]. Specifically, GLP-1RAs significantly reduced hospital admission for HF by nearly 10% (HR 0.91; 95% CI 0.83–0.99) [71]. However, it should be noted that a recent network meta-analysis aimed at evaluating GLP-1RAs and SGLT-2 inhibitors in patients with T2DM at varying cardiovascular risk reported that GLP-1RAs had a little or even no effect on hospital admission for HF (odds ratio 0.94, 95% confidence interval 0.85–1.03) compared with SGLT-2 inhibitors [72]. GLP-1RAs are usually well tolerated in clinical practice, although these drugs may induce nausea, constipation, abdominal pain or diarrhea, especially in the first weeks of use. Thad said, GLP-1RAs appear to be a valuable option for the treatment of NAFLD patients with or without coexisting HF (Table 1). However, given that there are no data from large RCTs with liver histological endpoints, the practice guidelines released from the European and American hepatology societies for management of NAFLD did not yet recommend the use of GLP-1RAs to specifically treat NAFLD or NASH [18•, 73•].

(A) Forest plot and pooled estimates of the effect of GLP-1RAs on the absolute percentage of liver fat content as assessed by magnetic resonance-based techniques (n = 7 randomized controlled trials) when compared with placebo or reference therapy. Data are reproduced from Mantovani et al. [68]. (B) Forest plot and pooled estimates of the effect of SGLT-2 inhibitors on the absolute percentage of liver fat content as assessed by magnetic resonance-based techniques (n = 7 randomized controlled trials) when compared with placebo or reference therapy. Data are reproduced from Mantovani et al. [69].
SGLT2 inhibitors are a relatively newer class of glucose-lowering drugs that act mainly by inhibiting SGLT2 receptors in the proximal convoluted tubule of the glomeruli, thus preventing sodium and glucose reabsorption and promoting their excretion in urine [74]. SGLT2 inhibitors are responsible for critical paradigm shifts in the management of patients with or at high risk for HF [75]. In this regard, a recent meta-analysis of 8 RCTs showed that SGLT-2 inhibitors significantly reduced all-cause mortality, cardiovascular mortality and hospitalization for HF [76]. Specifically, in that meta-analysis, treatment with SGLT-2 inhibitors reduced the risk of hospitalization for HF by nearly 30% (HR 0.69; 95% CI 0.64–0.74) [76]. A post-hoc analysis of the DECLARE-TIMI 58 trial also reported that dapagliflozin reduced the risk of first and total non-elective hospitalizations for any cause in patients with T2DM (irrespective of the presence of atherosclerotic cardiovascular disease), including hospitalizations not directly attributed to cardiac, kidney, or metabolic causes [77]. Other observational studies and some meta-analyses have even reported that SGLT2 inhibitors are able to reduce the risk of hospitalizations for HF in a broad range of patients with HF, regardless of T2DM status, LVEF and care setting [78,79,80]. Interestingly, experimental data also reported several favorable effects of SGLT-2 inhibitors on hepatic steatosis, necroinflammation and fibrosis, because of the combination of negative energy balance and substrate switching towards lipids as source of energy. Interestingly, a 2021 meta-analysis of 12 RCTs (involving a total of 850 overweight or obese adults with NAFLD, most of whom had T2DM) examining the efficacy of SGLT-2 inhibitors to specifically treat NAFLD reported that compared to placebo or reference therapy, the treatment with SGLT-2 inhibitors for a median of 24 weeks was associated with a significant improvement in serum liver enzyme levels and in the absolute percentage of liver fat content on magnetic resonance-based techniques (pooled weighted mean difference: -2.05%, 95% CI -2.61 to -1.48%) (as shown in Fig. 3, panel B) [69]. SGLT-2 inhibitors are usually well tolerated in clinical practice, although these agents may induce fungal urinary tract infections, especially in postmenopausal women. However, given that RCTs with histological liver endpoints are not available to date, it is still premature to recommend the use of SGLT-2 inhibitors for the treatment of NAFLD or NASH [18•, 73•]. That said, these findings suggest that SGLT-2 inhibitors might be an attractive therapeutic option in NAFLD patients with or at high risk for HF (Table 1).
Other drugs that are widely used in patients with HF [81], such as angiotensin converting enzyme inhibitors (ACE-inhibitors), angiotensin II receptor blockers (ARBs) and mineralocorticoid receptor antagonists, might exert some hepatoprotective effects in patients with NAFLD. Experimental and clinical studies, although not all, have reported that treatment with ACE inhibitors or ARBs may exert some anti-fibrotic effects on the liver [82,83,84,85,86,87]. More recently, in a post-hoc analysis of the PARADIGM-HF trial that included 8,232 HF patients with reduced LVEF who had available measures of liver function, treatment with sacubitril/valsartan has shown to significantly improve serum liver enzyme concentrations compared to enalapril after randomization [88]. However, these results should be primarily interpreted as consequence of the beneficial hemodynamic effects of sacubitril/valsartan on increased hepatic congestion, mainly due to elevated central venous pressure occurring in HF patients with reduced LVEF, instead of a drug-induced beneficial effect on hepatic steatosis. Although these classes of anti-hypertensive drugs are not specifically approved for the treatment of NAFLD or NASH, they can be safely prescribed for conventional indications.
Conclusions
This review further reinforces the notion that NAFLD is a “multisystem disease” mainly affecting the heart and vascular system and interacting with the regulation of several metabolic pathways [41]. Convincing evidence indicates that NAFLD is a risk factor for atherosclerotic cardiovascular disease, which is the leading cause of mortality in people with NAFLD [6, 7]. In the last years, there is a growing body of evidence also supporting a significant association between NAFLD and higher risk of developing new-onset HF.
Although there are multiple potential pathophysiological mechanisms by which NAFLD may adversely affect cardiac function and structure and increase the long-term risk of new-onset HF, no studies to date have proven a cause-and-effect relationship, and further research is certainly needed to better decipher the existing but complex link between NAFLD and risk of new-onset HF.
In the meantime, we believe that the major clinical implications of these findings are that a diagnosis of NAFLD can identify a subset of individuals, who are most exposed to a greater risk of developing both cardiovascular events and new-onset HF. Therefore, individuals with NAFLD might benefit from more intensive surveillance and early pharmacological interventions to decrease the risk of developing these adverse cardiovascular outcomes. As regards to this, future high-quality intervention studies are required to evaluate whether improvement or resolution of NAFLD achieved by treatment with GLP-1RAs and SGLT-2 inhibitors (alone or in combination) may also reduce the long-term risk of new-onset HF.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Bohm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–726. https://doi.org/10.1093/eurheartj/ehab368.
Younossi ZM, Golabi P, Paik JM, Henry A, Van Dongen C, Henry L. The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH): a systematic review. Hepatology. 2023;77(4):1335–47. https://doi.org/10.1097/HEP.0000000000000004.
Mantovani A, Scorletti E, Mosca A, Alisi A, Byrne CD, Targher G. Complications, morbidity and mortality of nonalcoholic fatty liver disease. Metabolism. 2020;111S:154170. https://doi.org/10.1016/j.metabol.2020.154170.
Karlsen TH, Sheron N, Zelber-Sagi S, Carrieri P, Dusheiko G, Bugianesi E, et al. The EASL-lancet liver commission: protecting the next generation of Europeans against liver disease complications and premature mortality. Lancet. 2022;399(10319):61–116. https://doi.org/10.1016/S0140-6736(21)01701-3.
AISF, SID, SIO. Non-alcoholic fatty liver disease in adults 2021: A clinical practice guideline of the Italian Association for the Study of the Liver (AISF), the Italian Society of Diabetology (SID) and the Italian Society of Obesity (SIO). Nutr Metab Cardiovasc Dis. 2022;32(1):1–16. https://doi.org/10.1016/j.numecd.2021.04.028
Mantovani A, Csermely A, Petracca G, Beatrice G, Corey KE, Simon TG, et al. Non-alcoholic fatty liver disease and risk of fatal and non-fatal cardiovascular events: an updated systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2021;6(11):903–13. https://doi.org/10.1016/S2468-1253(21)00308-3.
Duell PB, Welty FK, Miller M, Chait A, Hammond G, Ahmad Z, et al. Nonalcoholic fatty liver disease and cardiovascular risk: a scientific statement from the American heart association. Arterioscler Thromb Vasc Biol. 2022;42(6):e168–85. https://doi.org/10.1161/ATV.0000000000000153.
Anstee QM, Mantovani A, Tilg H, Targher G. Risk of cardiomyopathy and cardiac arrhythmias in patients with nonalcoholic fatty liver disease. Nat Rev Gastroenterol Hepatol. 2018;15(7):425–39. https://doi.org/10.1038/s41575-018-0010-0.
• Mantovani A, Byrne CD, Benfari G, Bonapace S, Simon TG, Targher G. Risk of heart failure in patients with nonalcoholic fatty liver disease: JACC review topic of the week. J Am Coll Cardiol. 2022;79(2):180–91. https://doi.org/10.1016/j.jacc.2021.11.007. This review provides an overview of the association between NAFLD and increased risk of HF, discuss the underlying pathophysiological mechanisms that link these diseases, and summarize targeted pharmacological treatments for NAFLD that might also reduce the risk of HF.
Alon L, Corica B, Raparelli V, Cangemi R, Basili S, Proietti M, et al. Risk of cardiovascular events in patients with non-alcoholic fatty liver disease: a systematic review and meta-analysis. Eur J Prev Cardiol. 2022;29(6):938–46. https://doi.org/10.1093/eurjpc/zwab212.
Henry L, Paik J, Younossi ZM. Review article: the epidemiologic burden of non-alcoholic fatty liver disease across the world. Aliment Pharmacol Ther. 2022;56(6):942–56. https://doi.org/10.1111/apt.17158.
Rinella ME, Neuschwander-Tetri BA, Siddiqui MS, Abdelmalek MF, Caldwell S, Barb D, et al. AASLD practice guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology. 2023. https://doi.org/10.1097/HEP.0000000000000323.
Younossi ZM, Golabi P, de Avila L, Paik JM, Srishord M, Fukui N, et al. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: a systematic review and meta-analysis. J Hepatol. 2019;71(4):793–801. https://doi.org/10.1016/j.jhep.2019.06.021.
Quek J, Chan KE, Wong ZY, Tan C, Tan B, Lim WH, et al. Global prevalence of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in the overweight and obese population: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2023;8(1):20–30. https://doi.org/10.1016/S2468-1253(22)00317-X.
Lonardo A, Nascimbeni F, Ballestri S, Fairweather D, Win S, Than TA, et al. Sex differences in nonalcoholic fatty liver disease: state of the art and identification of research gaps. Hepatology. 2019;70(4):1457–69. https://doi.org/10.1002/hep.30626.
Younossi ZM, Corey KE, Alkhouri N, Noureddin M, Jacobson I, Lam B, et al. Clinical assessment for high-risk patients with non-alcoholic fatty liver disease in primary care and diabetology practices. Aliment Pharmacol Ther. 2020;52(3):513–26. https://doi.org/10.1111/apt.15830.
Riazi K, Azhari H, Charette JH, Underwood FE, King JA, Afshar EE, et al. The prevalence and incidence of NAFLD worldwide: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2022;7(9):851–61. https://doi.org/10.1016/S2468-1253(22)00165-0.
• European Association for the Study of the L, European Association for the Study of D, European Association for the Study of O. EASL-EASD-EASO clinical practice guidelines for the management of non-alcoholic fatty liver disease. J Hepatol. 2016;64(6):1388–402. https://doi.org/10.1016/j.jhep.2015.11.004. European guidelines regarding the diagnosis and management of NAFLD and its advanced forms.
Kleiner DE, Brunt EM, Van Natta M, Behling C, Contos MJ, Cummings OW, et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology. 2005;41(6):1313–21. https://doi.org/10.1002/hep.20701.
Eslam M, Newsome PN, Sarin SK, Anstee QM, Targher G, Romero-Gomez M, et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J Hepatol. 2020;73(1):202–9. https://doi.org/10.1016/j.jhep.2020.03.039.
Eslam M, Sanyal AJ, George J, International Consensus P. MAFLD: A consensus-driven proposed nomenclature for metabolic associated fatty liver disease. Gastroenterology. 2020;158(7):1999–2014 e1. https://doi.org/10.1053/j.gastro.2019.11.312
Ayada I, van Kleef LA, Alferink LJM, Li P, de Knegt RJ, Pan Q. Systematically comparing epidemiological and clinical features of MAFLD and NAFLD by meta-analysis: focusing on the non-overlap groups. Liver Int. 2022;42(2):277–87. https://doi.org/10.1111/liv.15139.
Byrne CD, Patel J, Scorletti E, Targher G. Tests for diagnosing and monitoring non-alcoholic fatty liver disease in adults. BMJ. 2018;362:k2734. https://doi.org/10.1136/bmj.k2734.
Wong VW, Adams LA, de Ledinghen V, Wong GL, Sookoian S. Noninvasive biomarkers in NAFLD and NASH - current progress and future promise. Nat Rev Gastroenterol Hepatol. 2018;15(8):461–78. https://doi.org/10.1038/s41575-018-0014-9.
Hernaez R, Lazo M, Bonekamp S, Kamel I, Brancati FL, Guallar E, et al. Diagnostic accuracy and reliability of ultrasonography for the detection of fatty liver: a meta-analysis. Hepatology. 2011;54(3):1082–90. https://doi.org/10.1002/hep.24452.
Castera L, Friedrich-Rust M, Loomba R. Noninvasive assessment of liver disease in patients with nonalcoholic fatty liver disease. Gastroenterology. 2019;156(5):1264-81.e4. https://doi.org/10.1053/j.gastro.2018.12.036.
Selvaraj EA, Mozes FE, Jayaswal ANA, Zafarmand MH, Vali Y, Lee JA, et al. Diagnostic accuracy of elastography and magnetic resonance imaging in patients with NAFLD: a systematic review and meta-analysis. J Hepatol. 2021;75(4):770–85. https://doi.org/10.1016/j.jhep.2021.04.044.
Dhingra R, Gona P, Wang TJ, Fox CS, D’Agostino RB Sr, Vasan RS. Serum gamma-glutamyl transferase and risk of heart failure in the community. Arterioscler Thromb Vasc Biol. 2010;30(9):1855–60. https://doi.org/10.1161/ATVBAHA.110.207340.
Wannamethee SG, Whincup PH, Shaper AG, Lennon L, Sattar N. Gamma-glutamyltransferase, hepatic enzymes, and risk of incident heart failure in older men. Arterioscler Thromb Vasc Biol. 2012;32(3):830–5. https://doi.org/10.1161/ATVBAHA.111.240457.
Wang Y, Tuomilehto J, Jousilahti P, Salomaa V, Li B, Antikainen R, et al. Serum gamma-glutamyltransferase and the risk of heart failure in men and women in Finland. Heart. 2013;99(3):163–7. https://doi.org/10.1136/heartjnl-2012-302972.
Lee H, Lee YH, Kim SU, Kim HC. Metabolic dysfunction-associated fatty liver disease and incident cardiovascular disease risk: a nationwide cohort study. Clin Gastroenterol Hepatol. 2021;19(10):2138-47.e10. https://doi.org/10.1016/j.cgh.2020.12.022.
Simon TG, Roelstraete B, Hagstrom H, Sundstrom J, Ludvigsson JF. Non-alcoholic fatty liver disease and incident major adverse cardiovascular events: results from a nationwide histology cohort. Gut. 2022;71(9):1867–75. https://doi.org/10.1136/gutjnl-2021-325724.
• Mantovani A, Petracca G, Csermely A, Beatrice G, Bonapace S, Rossi A, et al. Non-alcoholic fatty liver disease and risk of new-onset heart failure: an updated meta-analysis of about 11 million individuals. Gut. 2022. https://doi.org/10.1136/gutjnl-2022-327672. Updated systematic review and meta-analysis showing that NAFLD is associated with a 1.5-fold higher long-term risk of new-onset HF, independent of the presence of diabetes, hypertension and other common cardiometabolic risk factors.
Vieira Barbosa J, Milligan S, Frick A, Broestl J, Younossi Z, Afdhal N, et al. Fibrosis-4 index can independently predict major adverse cardiovascular events in nonalcoholic fatty liver disease. Am J Gastroenterol. 2022;117(3):453–61. https://doi.org/10.14309/ajg.0000000000001606.
Peters AE, Pandey A, Ayers C, Wegermann K, McGarrah RW, Grodin JL, et al. Association of liver fibrosis risk scores with clinical outcomes in patients with heart failure with preserved ejection fraction: findings from TOPCAT. ESC Heart Fail. 2021;8(2):842–8. https://doi.org/10.1002/ehf2.13250.
Yoshihisa A, Sato Y, Yokokawa T, Sato T, Suzuki S, Oikawa M, et al. Liver fibrosis score predicts mortality in heart failure patients with preserved ejection fraction. ESC Heart Fail. 2018;5(2):262–70. https://doi.org/10.1002/ehf2.12222.
Simon TG, Roelstraete B, Alkhouri N, Hagstrom H, Sundstrom J, Ludvigsson JF. Cardiovascular disease risk in paediatric and young adult non-alcoholic fatty liver disease. Gut. 2023;72(3):573–80. https://doi.org/10.1136/gutjnl-2022-328105.
Fudim M, Zhong L, Patel KV, Khera R, Abdelmalek MF, Diehl AM, et al. Nonalcoholic fatty liver disease and risk of heart failure among medicare beneficiaries. J Am Heart Assoc. 2021;10(22):e021654. https://doi.org/10.1161/JAHA.121.021654.
VanWagner LB, Wilcox JE, Colangelo LA, Lloyd-Jones DM, Carr JJ, Lima JA, et al. Association of nonalcoholic fatty liver disease with subclinical myocardial remodeling and dysfunction: a population-based study. Hepatology. 2015;62(3):773–83. https://doi.org/10.1002/hep.27869.
Mantovani A, Pernigo M, Bergamini C, Bonapace S, Lipari P, Pichiri I, et al. Nonalcoholic fatty liver disease is independently associated with early left ventricular diastolic dysfunction in patients with type 2 diabetes. PLoS One. 2015;10(8):e0135329. https://doi.org/10.1371/journal.pone.0135329.
Targher G, Tilg H, Byrne CD. Non-alcoholic fatty liver disease: a multisystem disease requiring a multidisciplinary and holistic approach. Lancet Gastroenterol Hepatol. 2021;6(7):578–88. https://doi.org/10.1016/S2468-1253(21)00020-0.
Tilg H, Moschen AR, Roden M. NAFLD and diabetes mellitus. Nat Rev Gastroenterol Hepatol. 2017;14(1):32–42. https://doi.org/10.1038/nrgastro.2016.147.
Kacimi R, Long CS, Karliner JS. Chronic hypoxia modulates the interleukin-1beta-stimulated inducible nitric oxide synthase pathway in cardiac myocytes. Circulation. 1997;96(6):1937–43. https://doi.org/10.1161/01.cir.96.6.1937.
Li H, Chen C, Wang DW. Inflammatory cytokines, immune cells, and organ interactions in heart failure. Front Physiol. 2021;12:695047. https://doi.org/10.3389/fphys.2021.695047.
Tatsumi T, Matoba S, Kawahara A, Keira N, Shiraishi J, Akashi K, et al. Cytokine-induced nitric oxide production inhibits mitochondrial energy production and impairs contractile function in rat cardiac myocytes. J Am Coll Cardiol. 2000;35(5):1338–46. https://doi.org/10.1016/s0735-1097(00)00526-x.
Testa M, Yeh M, Lee P, Fanelli R, Loperfido F, Berman JW, et al. Circulating levels of cytokines and their endogenous modulators in patients with mild to severe congestive heart failure due to coronary artery disease or hypertension. J Am Coll Cardiol. 1996;28(4):964–71. https://doi.org/10.1016/s0735-1097(96)00268-9.
Buckley LF, Abbate A. Interleukin-1 blockade in cardiovascular diseases: a clinical update. Eur Heart J. 2018;39(22):2063–9. https://doi.org/10.1093/eurheartj/ehy128.
Malesza IJ, Malesza M, Walkowiak J, Mussin N, Walkowiak D, Aringazina R, et al. High-fat, western-style diet, systemic inflammation, and gut microbiota: a narrative review. Cells. 2021;10(11). https://doi.org/10.3390/cells10113164
Beam A, Clinger E, Hao L. Effect of diet and dietary components on the composition of the gut microbiota. Nutrients. 2021;13(8). https://doi.org/10.3390/nu13082795
Do MH, Lee E, Oh MJ, Kim Y, Park HY. High-glucose or -fructose diet cause changes of the gut microbiota and metabolic disorders in mice without body weight change. Nutrients. 2018;10(6). https://doi.org/10.3390/nu10060761
Chu H, Duan Y, Yang L, Schnabl B. Small metabolites, possible big changes: a microbiota-centered view of non-alcoholic fatty liver disease. Gut. 2019;68(2):359–70. https://doi.org/10.1136/gutjnl-2018-316307.
Stefan N, Schick F, Birkenfeld AL, Haring HU, White MF. The role of hepatokines in NAFLD. Cell Metab. 2023;35(2):236–52. https://doi.org/10.1016/j.cmet.2023.01.006.
Meex RCR, Watt MJ. Hepatokines: linking nonalcoholic fatty liver disease and insulin resistance. Nat Rev Endocrinol. 2017;13(9):509–20. https://doi.org/10.1038/nrendo.2017.56.
Lim S, Meigs JB. Ectopic fat and cardiometabolic and vascular risk. Int J Cardiol. 2013;169(3):166–76. https://doi.org/10.1016/j.ijcard.2013.08.077.
Petta S, Argano C, Colomba D, Camma C, Di Marco V, Cabibi D, et al. Epicardial fat, cardiac geometry and cardiac function in patients with non-alcoholic fatty liver disease: association with the severity of liver disease. J Hepatol. 2015;62(4):928–33. https://doi.org/10.1016/j.jhep.2014.11.030.
Inciardi RM, Chandra A. Epicardial adipose tissue in heart failure: risk factor or mediator? Eur J Heart Fail. 2022;24(8):1357–8. https://doi.org/10.1002/ejhf.2577.
Eslam M, Valenti L, Romeo S. Genetics and epigenetics of NAFLD and NASH: clinical impact. J Hepatol. 2018;68(2):268–79. https://doi.org/10.1016/j.jhep.2017.09.003.
Romero-Gomez M, Zelber-Sagi S, Trenell M. Treatment of NAFLD with diet, physical activity and exercise. J Hepatol. 2017;67(4):829–46. https://doi.org/10.1016/j.jhep.2017.05.016.
Nguyen NT, Varela JE. Bariatric surgery for obesity and metabolic disorders: state of the art. Nat Rev Gastroenterol Hepatol. 2017;14(3):160–9. https://doi.org/10.1038/nrgastro.2016.170.
Lee Y, Doumouras AG, Yu J, Brar K, Banfield L, Gmora S, et al. Complete resolution of nonalcoholic fatty liver disease after bariatric surgery: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2019;17(6):1040-60.e11. https://doi.org/10.1016/j.cgh.2018.10.017.
Verrastro O, Panunzi S, Castagneto-Gissey L, De Gaetano A, Lembo E, Capristo E, et al. Bariatric-metabolic surgery versus lifestyle intervention plus best medical care in non-alcoholic steatohepatitis (BRAVES): a multicentre, open-label, randomised trial. Lancet. 2023;401(10390):1786–97. https://doi.org/10.1016/S0140-6736(23)00634-7.
Aminian A, Al-Kurd A, Wilson R, Bena J, Fayazzadeh H, Singh T, et al. Association of bariatric surgery with major adverse liver and cardiovascular outcomes in patients with biopsy-proven nonalcoholic steatohepatitis. JAMA. 2021;326(20):2031–42. https://doi.org/10.1001/jama.2021.19569.
Krishnan A, Hadi Y, Alqahtani SA, Woreta TA, Fang W, Abunnaja S, et al. Cardiovascular outcomes and mortality after bariatric surgery in patients with nonalcoholic fatty liver disease and obesity. JAMA Netw Open. 2023;6(4):e237188. https://doi.org/10.1001/jamanetworkopen.2023.7188
Graziani F, Leone AM, Cialdella P, Basile E, Pennestri F, Della Bona R, et al. Effects of bariatric surgery on cardiac remodeling: clinical and pathophysiologic implications. Int J Cardiol. 2013;168(4):4277–9. https://doi.org/10.1016/j.ijcard.2013.04.202.
Kindel TL, Strande JL. Bariatric surgery as a treatment for heart failure: review of the literature and potential mechanisms. Surg Obes Relat Dis. 2018;14(1):117–22. https://doi.org/10.1016/j.soard.2017.09.534.
Datta T, Lee AJ, Cain R, McCarey M, Whellan DJ. Weighing in on heart failure: the potential impact of bariatric surgery. Heart Fail Rev. 2022;27(3):755–66. https://doi.org/10.1007/s10741-021-10078-w.
Targher G, Mantovani A, Byrne CD. Mechanisms and possible hepatoprotective effects of glucagon-like peptide-1 receptor agonists and other incretin receptor agonists in non-alcoholic fatty liver disease. Lancet Gastroenterol Hepatol. 2023;8(2):179–91. https://doi.org/10.1016/S2468-1253(22)00338-7.
Mantovani A, Petracca G, Beatrice G, Csermely A, Lonardo A, Targher G. Glucagon-Like Peptide-1 receptor agonists for treatment of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis: an updated meta-analysis of randomized controlled trials. Metabolites. 2021;11(2). https://doi.org/10.3390/metabo11020073.
Mantovani A, Petracca G, Csermely A, Beatrice G, Targher G. Sodium-glucose cotransporter-2 inhibitors for treatment of nonalcoholic fatty liver disease: a meta-analysis of randomized controlled trials. Metabolites. 2020;11(1). https://doi.org/10.3390/metabo11010022.
• Mantovani A, Byrne CD, Targher G. Efficacy of peroxisome proliferator-activated receptor agonists, glucagon-like peptide-1 receptor agonists, or sodium-glucose cotransporter-2 inhibitors for treatment of non-alcoholic fatty liver disease: a systematic review. Lancet Gastroenterol Hepatol. 2022;7(4):367–78. https://doi.org/10.1016/S2468-1253(21)00261-2. Recent systematic review showing the efficacy and safety of peroxisome proliferator-activated receptor agonists, glucagon-like peptide-1 receptor agonists, and sodium-glucose cotransporter-2 inhibitors for the treatment of NAFLD.
Kristensen SL, Rorth R, Jhund PS, Docherty KF, Sattar N, Preiss D, et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet Diabetes Endocrinol. 2019;7(10):776–85. https://doi.org/10.1016/S2213-8587(19)30249-9.
Palmer SC, Tendal B, Mustafa RA, Vandvik PO, Li S, Hao Q, et al. Sodium-glucose cotransporter protein-2 (SGLT-2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists for type 2 diabetes: systematic review and network meta-analysis of randomised controlled trials. BMJ. 2021;372:m4573. https://doi.org/10.1136/bmj.m4573.
• Chalasani N, Younossi Z, Lavine JE, Charlton M, Cusi K, Rinella M, et al. The diagnosis and management of nonalcoholic fatty liver disease: practice guidance from the American association for the study of liver diseases. Hepatology. 2018;67(1):328–57. https://doi.org/10.1002/hep.29367. American guidelines regarding the diagnosis and management of NAFLD and its advanced forms.
Zelniker TA, Braunwald E. Mechanisms of cardiorenal effects of sodium-glucose cotransporter 2 inhibitors: JACC state-of-the-art review. J Am Coll Cardiol. 2020;75(4):422–34. https://doi.org/10.1016/j.jacc.2019.11.031.
Braunwald E. Gliflozins in the management of cardiovascular disease. N Engl J Med. 2022;386(21):2024–34. https://doi.org/10.1056/NEJMra2115011.
Salah HM, Al’Aref SJ, Khan MS, Al-Hawwas M, Vallurupalli S, Mehta JL, et al. Effect of sodium-glucose cotransporter 2 inhibitors on cardiovascular and kidney outcomes-Systematic review and meta-analysis of randomized placebo-controlled trials. Am Heart J. 2021;232:10–22. https://doi.org/10.1016/j.ahj.2020.10.064.
Schechter M, Wiviott SD, Raz I, Goodrich EL, Rozenberg A, Yanuv I, et al. Effects of dapagliflozin on hospitalisations in people with type 2 diabetes: post-hoc analyses of the DECLARE-TIMI 58 trial. Lancet Diabetes Endocrinol. 2023;11(4):233–41. https://doi.org/10.1016/S2213-8587(23)00009-8.
Vaduganathan M, Docherty KF, Claggett BL, Jhund PS, de Boer RA, Hernandez AF, et al. SGLT-2 inhibitors in patients with heart failure: a comprehensive meta-analysis of five randomised controlled trials. Lancet. 2022;400(10354):757–67. https://doi.org/10.1016/S0140-6736(22)01429-5.
Packer M, Anker SD, Butler J, Filippatos G, Pocock SJ, Carson P, et al. Cardiovascular and renal outcomes with empagliflozin in heart failure. N Engl J Med. 2020;383(15):1413–24. https://doi.org/10.1056/NEJMoa2022190.
McMurray JJV, Solomon SD, Inzucchi SE, Kober L, Kosiborod MN, Martinez FA, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381(21):1995–2008. https://doi.org/10.1056/NEJMoa1911303.
Vaduganathan M, Claggett BL, Inciardi RM, Fonarow GC, McMurray JJV, Solomon SD. Estimating the benefits of combination medical therapy in heart failure with mildly reduced and preserved ejection fraction. Circulation. 2022;145(23):1741–3. https://doi.org/10.1161/CIRCULATIONAHA.121.058929.
Jonsson JR, Clouston AD, Ando Y, Kelemen LI, Horn MJ, Adamson MD, et al. Angiotensin-converting enzyme inhibition attenuates the progression of rat hepatic fibrosis. Gastroenterology. 2001;121(1):148–55. https://doi.org/10.1053/gast.2001.25480.
Moreno M, Gonzalo T, Kok RJ, Sancho-Bru P, van Beuge M, Swart J, et al. Reduction of advanced liver fibrosis by short-term targeted delivery of an angiotensin receptor blocker to hepatic stellate cells in rats. Hepatology. 2010;51(3):942–52. https://doi.org/10.1002/hep.23419.
Hirose A, Ono M, Saibara T, Nozaki Y, Masuda K, Yoshioka A, et al. Angiotensin II type 1 receptor blocker inhibits fibrosis in rat nonalcoholic steatohepatitis. Hepatology. 2007;45(6):1375–81. https://doi.org/10.1002/hep.21638.
Park JG, Mok JS, Han YI, Park TS, Kang KW, Choi CS, et al. Connectivity mapping of angiotensin-PPAR interactions involved in the amelioration of non-alcoholic steatohepatitis by Telmisartan. Sci Rep. 2019;9(1):4003. https://doi.org/10.1038/s41598-019-40322-1.
Torres DM, Jones FJ, Shaw JC, Williams CD, Ward JA, Harrison SA. Rosiglitazone versus rosiglitazone and metformin versus rosiglitazone and losartan in the treatment of nonalcoholic steatohepatitis in humans: a 12-month randomized, prospective, open- label trial. Hepatology. 2011;54(5):1631–9. https://doi.org/10.1002/hep.24558.
McPherson S, Wilkinson N, Tiniakos D, Wilkinson J, Burt AD, McColl E, et al. A randomised controlled trial of losartan as an anti-fibrotic agent in non-alcoholic steatohepatitis. PLoS One. 2017;12(4):e0175717. https://doi.org/10.1371/journal.pone.0175717.
Suzuki K, Claggett B, Minamisawa M, Packer M, Zile MR, Rouleau J, et al. Liver function and prognosis, and influence of sacubitril/valsartan in patients with heart failure with reduced ejection fraction. Eur J Heart Fail. 2020;22(9):1662–71. https://doi.org/10.1002/ejhf.1853.
Funding
Open access funding provided by Università degli Studi di Verona within the CRUI-CARE Agreement. GT is supported in part by grants from the University School of Medicine of Verona, Verona, Italy.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Human and Animal Rights
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Inciardi, R.M., Mantovani, A. & Targher, G. Non-Alcoholic Fatty Liver Disease as an Emerging Risk Factor for Heart Failure. Curr Heart Fail Rep 20, 308–319 (2023). https://doi.org/10.1007/s11897-023-00613-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11897-023-00613-1