
Abstract
There is growing evidence that air pollutants might affect human behavior. This study assesses the associations between air pollution concentrations and emergency department (ED) visits for abuse of psychoactive substances. 28,745 such ED visits were identified and retrieved from a health database containing diagnosed visits from five hospitals in Edmonton (Canada) over 10 years. The ED visits were analyzed as daily counts. Conditional Poisson regression models were used to estimate the associations between the number of ED visits and concentration levels of gaseous air pollutants (carbon monoxide (CO), nitrogen dioxide (NO2), sulphur dioxide (SO2), ozone (O3)) and particulate matters (PM2.5 and PM10, fine and coarse, respectively). Air pollutants and weather factors in the realized statistical models were lagged by the same number of days, from 0 to 5 days. The associations were estimated in the form of concentration-response functions. The results show relative risks and their 95% confidence intervals. Positive and statistically significant associations were obtained for CO for all patients (lags from 0 to 5), males (lags 1 and 3–5), and females (lag 4). For NO2, exposure lagged by 1 and 2 days has a positive statistically significant association for all and male patients. PM10 shows the same type of associations lagged by 2 and 3 days. PM2.5 (lag 2) is associated only in females. The results indicate that urban air pollution may have an impact on the abuse of psychoactive substances.
Similar content being viewed by others
Introduction
There is growing evidence supporting the associations between ambient air pollution and a wide range of health conditions. Air pollution may affect various tissues and organs, including skin and sense organs (eye and otitis media). Air pollution may also have systemic effects, and may impact a large spectrum of neurobehavioral disorders. The existing literature indicates correlations between ambient air pollution and a variety of disordered behaviors, including drug abuse, behavioral disorders, depression, and suicide (Bakian et al. 2015; Kim et al. 2010; Lundberg 1996; Szyszkowicz 2007; Szyszkowicz et al. 2010; Szyszkowicz et al. 2016; Szyszkowicz et al. 2018; Szyszkowicz 2019).
Sussman and collaborators (Sussman et al. 2015), in their commentary publication, explored the following question: “Could environmental exposures be a factor in increased susceptibility to addictive behaviors?” Based on the literature review, the authors suggested that environmental exposures to air pollutants can contribute to dysregulation of mesolimbic dopamine (DA) turnover, “resulting in an increased propensity for addictive behaviors to manifest themselves” (Sussman et al. 2015). In other studies on this topic, Miller (Miller 1999; Miller 2000) presented and discussed the implication of environmental pollutants on addiction, but did not present a neurobiological mechanisms in her theoretical approach. Miller introduced and applied the term “toxicant-induced loss of tolerance.” She supported her terminology by assuming that people exposed to air pollutants may become more susceptible to the effects of drugs. Thus, drug users may observe an impact of lower quantities of drugs and have greater difficulties with withdrawal because of environmental toxicants. As Sussman and colleagues (Sussman et al. 2015) wrote: “While not describing neurobiological mechanisms, her ideas may be consistent with the potential impact of toxicants on mesolimbic DA shrinkage or depletion.”
There is an established link between substance use disorder and mental health problems such as depression. Emergency department (ED) presentations for substance abuse may be affirmations of mental health conditions. “If ambient air pollutants do indeed affect the central nervous system and provoke psychiatric symptoms” (Amitai et al. 1998), one might expect a corresponding increase in hospital presentations and admissions for substance use disorder (Szyszkowicz et al. 2018). Several mental health disorders tend to be more prevalent in the urban populations and are correlated with ambient air pollution concentration levels. Apart from ambient air pollution, population density, traffic intensity, generated noise, sedentary lifestyle, drug use, urbanization, comorbidity, social economic position, or other factors might mediate there health effects. It is not known exactly which components of air pollution might contribute to the development of mental health problems, but there are a few potential mechanisms explaining causality. Air pollutants might affect the human brain via neuroinflammatory processes (Khan et al. 2019). Other mechanisms and processes might be triggered and developed by oxidative stress, epigenetic alterations, and dysfunction of the hypothalamic-pituitary-adrenal axis (Thomson 2019).
This paper does a re-analysis of previously published work (Szyszkowicz et al. 2018). In the presented work, we used health outcomes from the previous study and extended the project to include drug dependency data. Additionally, we proposed a new statistical methodology for the extended health data.
In this work, ED visits for abuse of psychoactive substance, including alcohol dependence syndrome, drug dependence, and nondependent abuse of drugs, are investigated in relation to ambient air pollution concentrations. The hypothesis is that ambient air pollutants are associated with the number of ED visits for substance use disorder.
Methods
Health data
Health conditions, recorded as diagnosed ED visits data from five hospitals in Edmonton (Canada), were collected and organized as a health database. Data on ED visits were retrieved from the database for the period April 1, 1998, to March 31, 2002 (3,652 days). The health outcomes related to this study were identified by applying the International Classification of Diseases 9th Revision (ICD-9) codes. The following three health problems, considered as substance use disorder, were jointly investigated: alcohol dependence syndrome (ICD-9: 303), drug dependence (ICD-9: 304), and nondependent abuse of drugs (ICD-9: 305). The applied statistical methods used daily counts. Daily counts of ED visits were calculated as the sum of daily health events diagnosed in one of these three categories (ICD-9: 303–305). The time-series form of the analyzed data was used for the period of 3,652 days, i.e., daily counts, daily average of temperature and relative humidity, and average of daily concentration of air pollutants as an exposure.
Environmental data
In this work, six ambient air pollutants are considered and investigated: four gases (carbon monoxide (CO), nitrogen dioxide (NO2), sulphur dioxide (SO2), and ozone (O3)) and two particulate matters (PM2.5 (fine particulate matter no greater than 2.5 microns in diameter) and PM10 (coarse particulate matter no greater than 10 microns in diameter)). The daily concentration of these pollutants is represented as an average of 24 values of hourly measurements. The estimated values are the average of three monitor stations operating during this period. The maximum distance among the three stations used in the city of Edmonton was 11 km. The air pollutant measurement data came from Canada’s National Air Pollution Surveillance and the weather data came from Environment Canada’s weather archive. More details on these environmental data, air pollutants, and methods of their measurements are presented in another publication by Canadian authors (Zemek et al. 2010).
In the applied statistical models, the daily average ambient temperature and relative humidity are covariates. We represented the weather factors as natural splines with three degrees of freedom, which allows for the adjustment of weather factors in their non-linear form. In the constructed statistical models, ambient air pollutants and meteorological factors were lagged by the same number of days.
Statistical methods
This work is a short-term air pollution health effects study with day as a time unit. The presented study analyzes the potential associations of six ambient air pollution with the number of ED visits in Edmonton, Canada, using a case-crossover (CC) strategy (Maclure 1991). The CC design is very similar to a crossover study, where each subject serves as his or her own control, and is an attractive alternative to the classic case–control design. A CC study is used to study onset of acute events where the risk factors of interest vary by time. Exposures within cases at different times, considered as controls, are compared. In the standard and widely used CC approach, a time-stratified technique is used to define the control periods (Janes et al. 2005). Typically, the same days of week in 1 month are chosen and health risk is estimated by applying case and control period(s) exposures. In the standard CC method, conditional logistic regression is used to estimate the odds ratio (OR). In this paper, conditional Poisson models are applied as a flexible alternative technique to the case-crossover methodology, and as such, relative risks (RRs) are estimated (Szyszkowicz 2006; Armstrong et al. 2014; Szyszkowicz and Burr 2016; Szyszkowicz 2019; Szyszkowicz 2020). In order to do this, we created a strata hierarchy using the following calendar structure <year: month: day of week>. Thus, the study days are nested in the natural hierarchical structure of the constructed strata: days in days of week, days of week in months, and months in the corresponding years (Szyszkowicz 2006). The conditional Poisson models are then used with respect to the constructed strata. On each stratum, the regression is performed with respect to the air pollution concentration levels. The effect of time is controlled by the strata. One stratum has 4 or 5 days, depending on the length of the month (months with 28, 29, 30, or 31 days) and the day of week in a considered month.
To investigate the concentration-response associations, the values of the concentration levels were transformed. The following formula was applied to estimate the RR as the function of the variable z, RR(z) = exp(β(z)). Here the variable z represents the concentration of air pollutant (for example, z = NO2). The coefficient β(z) is a function of the concentration. The formula for β(z) has the following form:
where r is the range of the concentrations. The parameters μ (mu) and τ (tau) determine the logistic function. Usually, the function f(z) has a simple form as f(z) = z, f(z) = log(z), or others.
In the standard CC method, and using conditional logistic regression, OR is estimated as OR(z) = exp(β*z), where the coefficient β (slope) has a constant value. In this kind of statistical model, the concentration-response shape always has one form of the same exponential function, with varying β values. In the method presented here, the coefficient varies with concentration levels.
In this paper, three forms of the function f(z) are used: \(f\left(z\right)=z, f\left(z\right)=\sqrt{z}, f\left(z\right)={z}^{1.5}\), i.e., an identical, concave, and convex function, respectively. The constant Beta (slope) is determined by using the statistical regression models (Nasari et al. 2016). Here, the transformed concentration z, represented as the product of the function f(z) and the logistic function of z, is used in the conditional Poisson regression models.
For a given initial value of the parameters mu and tau, the coefficient β (Beta) is estimated using the conditional Poisson regression on the constructed strata. The values of β, mu, tau, and f(z) define the concentration-response shape function as the function β(z) is determined. The process to estimate the optimal values of the parameters mu and tau is completed as an iterative algorithm. A similar approach was used in (Szyszkowicz 2018), where a minimization routine was applied to fit the statistical model to produce the minimum AIC (Akaike information criterion) value. This minimization algorithm estimates the parameters and from those parameters, the concentration-response function.
In this study, we considered only two fixed values of the parameter tau, 0.1 and 0.2 (Nasari et al. 2016). As the value of the parameter mu, the successive percentiles of the air pollutant concentrations are used and submitted into the constructed models. The computer program then fits the model with the fixed triplets (mu, tau, f(z)) and returns the coefficient β. The proposed triplet also gives the minimum of the AIC value as an optimal solution. The result (β, mu, tau, f(z)) from the used model allows to calculate the coefficient β(z), which is a function of the air pollutant concentration and determines the shape. These flexible models allow the construction of all forms of concentration-response functions. A similar approach was used in longitudinal cohort study related to air pollution and mortality (Burnett et al. 2018). The Supplementary Materials provide the corresponding software code used for this methodology. We completed this project using R computer statistical software (Version 3.5.1; ©2018, The R Foundation for Statistical Computing).
Results
During the period of the study, from April 1, 1992, to March 31, 2002 (3,652 days), 28,745 ED visits were identified, retrieved, and used. Among these ED visits diagnosed for abuse of psychoactive substance, 5,921 were for alcohol dependence syndrome (male 4,207 (71%) cases, female 1,714 (29%) cases), 1,212 were for drug dependence (male 714 (59%) cases, female 498 (41%) cases), and 21,612 were for nondependent abuse of drugs (male 13,779 (64%) cases, female 7,833 (36%) cases).
Table 1 presents summary statistics on the environmental parameters and ED visits considered in the study. Data were missing for 61% of days for fine particulate matter and 23% of days for coarse particulate matter pollutants. We excluded days missing this data from the study.
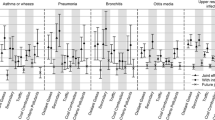
Figure 1 summarizes the results for the 6 air pollutants by 0 to 5 lags. The figure shows three qualitative categories, positive (red) and negative (green) statistically significant associations and also situations with no associations found (neutral, white). In this study, P-values less than 0.05 indicated statistical significance. Thus, the probability of obtaining the results seen in the study, if the null hypothesis (β = 0) is actually true, is less than 0.05. Figure 1 may be interpreted as a map of the associations between ED visits and lagged exposures.

A qualitative map of the associations: positive (1, red), negative (−1, green), and neutral (0, white).
Table 2 gives numerical estimations for the six considered air pollutants and their lags from 0 to 5 days. The associations between carbon monoxide and ED visits are positive and statistically significant for the exposure lagged by 0 to 5 days. The listed parameters allowed the construction of the corresponding Figures 2 and 3.

The concentration-response shapes for carbon monoxide exposure. ED visits, all patients, Edmonton, Canada, 1992–2002.

The concentration-response shapes for nitrogen dioxide exposure. ED visits, all patients, Edmonton, Canada, 1992–2002.
Figure 2 presents the concentration-response shapes for the association between ED visits and ambient carbon monoxide (z = CO) levels. The functions give values of the RR along the CO concentration levels. In addition, a 95% confidence interval (CI) is estimated and added to the graph. The figure illustrates the estimations obtained for the exposures, lagged from 0 to 5 days. For example, for the same day (lag 0) exposure for carbon monoxide, the obtained values are β = 0.7719, standard error = 0.3134, statistically significant (P-value = 0.0138). The mu (4.8) was in the 100th percentile of carbon monoxide concentration, tau = 0.1, and as the transformation function f(z) is used, the function is indexed by the number 2, i.e., here \(f\left(z\right)=\sqrt{z}\). This example shows how to interpret the values presented in the tables.
Figure 3 illustrates the function RR(z) related to the concentration-response shape for nitrogen dioxide (z = NO2). Supplementary Materials provide two tables which show the results for male and female patients using the same convention of interpretation. For illustrative purposes, sample code (in R) is provided in the Supplementary Materials. The code illustrates that the presented concentration-response functions were drawn for the optimal parameters.
Discussion
This study examined ED visits for drug dependence and nondependent abuse of psychoactive substances for patients in five EDs in Edmonton, Canada, over a period of 10 years. The main result of this work is the estimation of an association between exposure to specific ambient air pollutants and the numbers of ED visits for substance use problems. The considered visits may represent acute psychiatric symptomology and among various be classified as drug abuse. Some of the visits may have been related to a suicide attempt, though this information is not specifically indicated in the used database.
In this work, all, male, and female patients exposed to elevated air pollution concentrations were more likely to visit ED for psychoactive substances use disorder. As the results indicate, carbon monoxide and nitrogen dioxide were individually associated with increased ED presentations for substance abuse. The positive statistically significant associations are also seen for both types of particulate matter. Unfortunately, in this study, PM2.5 data were missing for 61% of the study period (available from April 1998 to April 2002) and PM10 for 23% (available from January 1994 to April 2002). This missing information undoubtedly largely affects the results for their associations with the number of ED visits. Figure 1 shows a few positive statistically significant associations for both PMs. It is a possible limitation of the study that such data are not available for the whole period.
This study is a re-analysis of the work presented in (Szyszkowicz et al. 2018) with two new elements. In this study, ED data were expanded by visits diagnosed as drug dependence (ICD-9: 304) cases. The applied statistical methodology is also augmented. In the previous work (Szyszkowicz et al. 2018), the standard CC method was used; here, an optimal concentration-response parametric function is fitted. In addition to estimating relative risk, the current study provides the shape of the concentration-response curve to illustrate the relationship between air pollution levels and health outcomes. The curve shapes demonstrate various non-linear forms.
The results on the risk estimates from the current study are consistent with the previous findings. Similar to previous studies, we observed positive, statistically significant associations for exposure to carbon monoxide, nitrogen dioxide, and particulate matter and the outcome of interest.
While few studies in the literature currently report on the impacts of air pollution on substance abuse, there is a growing body of evidence that exposure to air pollution affects the brain and can alter behavior. Several studies have reported associations between air pollutants and cognitive function (Calderón-Garcidueñas et al. 2008; Suglia et al. 2008; Chen and Schwartz 2009; Szyszkowicz 2019; Ranft et al. 2009; Power et al. 2011).
This study includes several limitations that are common in observational research, including the adequacy of the statistical models used, and potential impact of measurement error in the concentration of ambient air pollutants and outcome variables. The triangular configuration of the three monitors in the area of the study is well designed. The largest distance among the monitor stations is about 11 km. The health data were collected from five hospitals in Edmonton and they are not separated from each other by more than 10 km.
Common sources of carbon monoxide are motor vehicles, fireplaces, coal and wood stoves, kerosene space heaters, charcoal grills, gas appliances, and internal combustion engines. The largest source of carbon monoxide is natural in origin. As was mentioned in (Sussman et al. 2015), the measured values for carbon monoxide may not represent actual vertical distribution.
Carbon monoxide has almost the same density as air. Its molar mass is 28.0, where air has a molar mass of 28.8. By a consequence, human height level exposure concentrations may be higher than those recorded by monitoring stations. Usually, these stations are located a few meters above the ground.
Conclusion
This paper presented the results from short-term exposure to ambient air pollutants. Six ambient air pollutants, four gaseous and two particulate matters, were considered in relation to ED visits for substance use disorder. In the constructed models, daily counts of ED visits were analyzed. In the statistical models, the daily weather factors, temperature and relative humidity, were represented in the form of natural splines. The daily concentration levels of air pollutants were transformed to obtain the parametric non-linear response shapes. The positive statistically significant associations were assessed for carbon monoxide exposure lagged from 0 to 5 days. It is main conclusion of this study: carbon monoxide concentration levels may be associated with substance use disorders. The results are also positive for some other urban air pollutants. The estimated functions allow the identification of concentrations with various intensities of impact on health. In some cases, these functions indicate a potential threshold concentration.
In this study, urban ambient air pollution is associated with an increase in the number of ED visits for psychoactive substance disorders in Edmonton, Canada.
Data availability
The health data (ED visits) that support the findings of this study are available from Health Canada but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the Alberta Health Services (https://www.albertahealthservices.ca/default.aspx). The daily averages of the used environmental data (air pollution concentrations and weather factors) are available from the author on reasonable request. The original (hourly measurements) environmental data are available from the National Air Pollution Surveillance (NAPS) Program (http://maps-cartes.ec.gc.ca/rnspa-naps/data.aspx), which is the main source of ambient air quality data in Canada.
References
Amitai Y, Zlotogorski Z, Golan-Katzaw V, Wexler A, Gross D (1998) Neuropsychological impairment from acute low-level exposure to carbon monoxide. Arch Neurol 55:845–848
Armstrong BG, Gasparrini A, Tobias A (2014) Conditional Poisson models: a flexible alternative to conditional logistic case cross-over analysis. BMC Med Res Methodol 14:122. https://doi.org/10.1186/1471-2288-14-122
Bakian AV, Huber RS, Coon H, Gray D, Wilson Ph, McMahon W (2015) Acute air pollution exposure and risk of suicide completion. Am J Epidemiol 181(5):295–303. https://doi.org/10.1093/aje/kwu341
Burnett R, Chen H, Szyszkowicz M, Fann N, Hubbell B, Pope CA et al (2018) Global estimates of mortality associated with long-term exposure to outdoor fine particulate matter. Proc Natl Acad Sci USA 115(38):9592–9597. https://doi.org/10.1073/pnas.1803222115
Calderón-Garcidueñas L, Mora-Tiscareño A, Ontiveros E, Gómez-Garza G, Barragán-Mejía G, Broadway J et al (2008) Air pollution, cognitive deficits and brain abnormalities: a pilot study with children and dogs. Brain Cogn 68(2):117–27. https://doi.org/10.1016/j.bandc.2008.04.008
Chen JC, Schwartz J (2009) Neurobehavioral effects of ambient air pollution on cognitive performance in US adults. Neurotoxicology 30:231–239. https://doi.org/10.1016/j.neuroscience.2008.12.011
Janes H, Sheppard L, Lumley T (2005) Case-crossover analyses of air pollution exposure data: referent selection strategies and their implications for bias. Epidemiology 16:717–726
Khan A, Plana-Ripoll O, Antonsen S, Brandt J, Geels C, Landecker H, Sullivan PF, Pedersen CB, Rzhetsky A (2019) Environmental pollution is associated with increased risk of psychiatric disorders in the US and Denmark. PLoS Biol 17(8):e3353. https://doi.org/10.1371/journal.pbio.3000353
Kim C, Jung SH, Kang DR, Kim HC, Moon KT, Hur NW, Shin DC, Suh J (2010) Ambient particulate matter as a risk factor for suicide. Am J Psychiatry 167(9):1100–1107. https://doi.org/10.1176/appi.ajp.2010.09050706
Lundberg A (1996) Psychiatric aspects of air pollution. Otolaryngol Head Neck Surg 114:227–231. https://doi.org/10.1016/S0194-59989670172-9
Maclure M (1991) The case-crossover design: a method for studying transient effects on the risk of acute events. Am J Epidemiol 133(2):144–153
Miller CS (1999) Are we on the threshold of a new theory of disease? Toxicant induced loss of tolerance and its relationship to addiction and abdiction. Toxicology and Industrial Health 15:284–294
Miller CS (2000) Toxicant-induced loss of tolerance. Addiction 96:115–139
Nasari MM, Szyszkowicz M, Chen H, Crouse D, Turner MC, Jerrett M et al (2016) A class of non-linear exposure-response models suitable for health impact assessment applicable to large cohort studies of ambient air pollution. Air Qual Atmos Health 9(8):961–972
Power MC, Weisskopf MG, Alexeeff SE, Coull BA, Spiro A, Schwartz J (2011) Traffic-related air pollution and cognitive function in a cohort of older men. Environ Health Perspect 119:682–687. https://doi.org/10.1289/ehp.1002767
Ranft U, Schikowski T, Sugiri D, Krutmann J, KraÈmer U (2009) Long-term exposure to traffic-related particulate matter impairs cognitive function in the elderly. Environ Res 109:1004–1011. https://doi.org/10.1016/j.envres.2009.08.003
Suglia SF, Gryparis A, Wright RO, Schwartz J, Wright RJ (2008) Association of black carbon with cognition among children in a prospective birth cohort study. Am J Epidemiol 167:280–286. https://doi.org/10.1093/aje/kwm308
Sussman S, Ames SL, Avol E (2015) Could environmental exposures facilitate the incidence of addictive behaviors? Eval Health Prof 38(1):53–8. https://doi.org/10.1177/0163278713501692
Szyszkowicz M (2006) Use of generalized linear mixed models to examine the association between air pollution and health outcomes. Int J Occup Med Environ Health 19:224–227
Szyszkowicz M (2007) Air pollution and emergency department visits for depression in Edmonton, Canada. Int J Occup Med Environ Health 20(3):241–5
Szyszkowicz M (2019) Urban ambient air pollution and behavioural disorders. Int Arch Subst Abuse Rehabil 1:005. https://doi.org/10.23937/iasar-2017/1710005
Szyszkowicz M (2019) Urban ambient air pollution and behavioural disorders. International Archives of Substance Abuse and Rehabilitation. https://doi.org/10.23937/iasar-2017/1710005
Szyszkowicz M (2020) Use of two-point models in “Model choice in time-series studies of air pollution and mortality.” Air Qual Atmos Health. https://doi.org/10.1007/s11869-019-00787-5
Szyszkowicz M, Willey JB, Grafstein E, Rowe BH, Colman I (2010) Air pollution and emergency department visits for suicide attempts in Vancouver, Canada. Environ Health Insights 4:79–86. https://doi.org/10.4137/EHI.S5662
Szyszkowicz M, Kousha T, Kingsbury M, Colman I (2016) Air pollution and emergency department visits for depression: a multicity case-crossover study. Environmental Health Insights 10:155–161. https://doi.org/10.4137/EHI.S40493
Szyszkowicz M, Thomson EM, Colman I, Rowe BH (2018) Ambient air pollution exposure and emergency department visits for substance abuse. PLoS One 13(6):e0199826. https://doi.org/10.1371/journal.pone.0199826
Szyszkowicz M (2018) Concentration–response functions for short-term exposure and air pollution health effects. Environmental Epidemiology 2(2) - p e011. https://doi.org/10.1097/EE9.0000000000000011.
Szyszkowicz M (2019) Case-crossover method with a short time-window. Int J Environ Res Public Health 17(1). doi: https://doi.org/10.3390/ijerph17010202.
Szyszkowicz M, Burr WS (2016) The use of chained two-point clusters for the examination of associations of air pollution with health conditions. Int J Occup Med Environ Health 29:613–622. https://doi.org/10.13075/ijomeh.1896.00379.
Thomson EM (2019) Air pollution, stress, and allostatic load: linking systemic and central nervous system impacts. J Alzheimer’s Dis. https://doi.org/10.3233/JAD-190015
Zemek R, Szyszkowicz M, Rowe BH (2010) Air pollution and emergency department visits for otitis media: a case-crossover study in Edmonton. Canada. Environ. Health Perspect 118(11):1631–1636. https://doi.org/10.1289/ehp.0901675
Funding
Open access funding provided by Health Canada.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Health Canada Research Ethic Board determined that the study is IRB exempt, given that patient data were pre-existing and de-identified.
Consent for publication
The publisher has the author’s permission to publish research findings.
Competing interests
The author declares no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Szyszkowicz, M. Urban ambient air pollution and substance use disorder. Air Qual Atmos Health 15, 1111–1120 (2022). https://doi.org/10.1007/s11869-022-01182-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11869-022-01182-3