
Opinion statement
The specialty of palliative care has evolved over time to provide symptom management, psychosocial support, and care planning for patients with cancer throughout the disease continuum and in multiple care settings. This review examines the delivery and impact of palliative care in the outpatient, inpatient, and community-based settings. The article will discuss how these 3 palliative care settings can work together to optimize patient outcomes under a unifying model of palliative care “anywhere, anytime” and how to prioritize palliative care services when resources are limited. Many patients with advanced cancer receive care from each of the 3 branches of palliative care—outpatient, inpatient, and community-based settings—at some point along their disease trajectory. Early on, outpatient clinics provide longitudinal supportive care concurrent with active disease-modifying treatments. Telemedicine appointments can serve patients remotely to minimize their need to travel. When patients experience functional decline, community-based palliative care services can provide support and monitoring for patients at home. When patients develop acute symptomatic complications requiring admission, inpatient care consultation teams are essential for symptom management and goals-of-care discussions. For patients in severe distress, receiving care in a palliative care unit that provides intensive symptom control and facilitates complex discharge planning is ideal. Under a unifying model of palliative care designed to offer care “anywhere, anytime,” the 3 branches of palliative care could work in unison to support each other, minimize gaps in care, and optimize patient outcomes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Palliative care has evolved over the past 6 decades as a specialty that focuses on delivering patient-centered, interdisciplinary care to alleviate suffering, improve patients’ quality of life, and enhance the quality of care. In the 1950s, Dame Cicely Saunders in the UK started the hospice movement to improve the care of dying patients in the community [1]. In the 1970s, Dr. Balfour Mount coined the term “palliative care” and established the first palliative care unit in Montreal, Canada [2]. This marked the expansion of palliative care from community-based settings to acute care facilities, in which specialist teams also provided consultations for hospitalized patients in acute distress. In 1990s, Dr. Eduardo Bruera initiated one of the first outpatient palliative care clinics in Edmonton, Canada, marking the beginning of palliative care for patients in the outpatient setting. In 2010, Dr. Jennifer Temel published her landmark randomized controlled trial on early palliative care [3]. Since then, the term “supportive care” has been adopted in a growing number of palliative care programs to signal their availability throughout a patient’s disease trajectory rather than only at the end-of-life [4, 5, 6•). In 2020, the COVID-19 pandemic catalyzed telemedicine visits as a care delivery model and enabled palliative care to reach more patients and caregivers [7]. This brief history of palliative care underscores how this specialty has expanded its scope to better serve a greater number of patients at different disease stages and in a variety of care settings.
As palliative care evolves, a growing body of literature supports the delivery of palliative care in various settings. Multiple randomized controlled trials have reported that adding specialist palliative care in the outpatient, inpatient, and community-based care settings to routine care can improve patient outcomes. In addition, several systematic reviews and meta-analyses have found that specialist palliative care has a positive impact on patients’ quality of life and symptom burden, patient satisfaction, and home death [8••, 9, 10]. However, many of these studies included a mix of care settings, making it difficult to know which form of palliative care is most effective. Accordingly, in this article, the delivery and impact of palliative care in the outpatient, inpatient, and community-based settings will be examined separately. The article will also consider how these 3 palliative care settings can work together to optimize patient outcomes under a unifying model of palliative care “anywhere, anytime.”
Outpatient palliative care
Outpatient palliative care clinics are the main settings in which patients receive timely access to specialized supportive care. In contrast to patients seen in inpatient and community-based palliative care settings, those seen in outpatient palliative care clinics often have better performance status and longer survival durations. By providing symptom management, psychological support, and care-planning services longitudinally, outpatient palliative care clinics alleviate distress throughout the disease trajectory, maximize patients’ readiness for disease-modifying treatments, and potentially prevent costly hospitalizations [11•].
In 2009, only 59% of National Cancer Institute (NCI)-designated cancer centers and 22% of non-NCI-designated cancer centers in the USA reported having outpatient palliative care clinics. These percentages increased to 95% and 40%, respectively, in 2018. The time from outpatient palliative care referral to death also increased from 3 to 6 months at NCI-designated cancer centers from 2009 to 2018 [6•].
Outpatient palliative care can be classified as stand-alone, embedded, or co-located. Care is typically provided in person. Telemedicine visits have become more common since the start of the COVID-19 pandemic. These visits allow patients in rural areas, those with limited mobility, and those with transportation challenges ease of access to specialized palliative care teams. Another potentially useful telemedicine strategy is telemonitoring, in which symptom scores, vital signs, and other parameters can be monitored remotely with predefined prompts for self-management and real-time triggers for interventions by the health care team [12]. However, regional regulations, reimbursement policies, and access to the Internet and devices for video conferencing may pose challenges to telemedicine delivery. Besides providing symptom management, psychological support, and care-planning services, outpatient palliative care clinics also offer point-of-contact service for questions and medication refills [13]. For selected patients with high symptom burden or poor performance status, proactive phone calls from the clinic after hospital discharge or in between clinic visits may reduce patients’ distress and emergency room visits. Some outpatient palliative care clinics also offer same-day consultations to provide urgent symptom management and rapidly triage patients’ supportive care needs.
Several systematic reviews have examined the impact of outpatient palliative care referrals on patient outcomes. Haun et al. conducted a Cochrane systematic review and meta-analysis in 2017 [14]. They included 7 randomized trials with 1615 participants. Compared to usual care, outpatient palliative care was associated with a significant improvement in quality of life (standardized mean difference [SMD], 0.27; 95% CI, 0.15–0.38) and symptoms (SMD, −0.23; 95% CI, −0.35 to −0.10); however, depressive symptoms did not differ among patients treated in the 2 settings.
A more recent systematic review that included 10 randomized trials involving patients with advanced cancer was conducted by Fulton et al. [15] in 2019. The authors concluded that, compared to usual care, specialist palliative care conferred a small but significant benefit on quality of life (SMD, 0.24; 95% CI, 0.13–0.35), but no significant benefits were seen for patients’ symptom burdens (SMD, −0.17; 95% CI, −0.45 to 0.11) or survival (hazard ratio, 0.84; 95% CI, 0.61–1.71).
Hoerger et al. also conducted a meta-analysis to examine survival and quality of life in patients with advanced cancer [16]. The authors reported that, compared to usual care, outpatient palliative care was associated with a survival benefit at 1 year (14.1%; 95% CI, 6.5–21.7%). However, there was no survival benefit at 3 months or at 24 months. Consistent with other meta-analyses, the study also reported an improvement in quality of life (SMD (Hedges’ g), 0.18; 95% CI, 0.09–0.28) with specialist palliative care.
In addition to these randomized trials and meta-analyses, several non-randomized cohort studies have also reported that the timely involvement of palliative care is associated with a reduction in emergency room visits, intensive care unit admissions, and hospital deaths in the last month of life [17,18,19,20]. Indeed, patients who were first referred to palliative care as outpatients had better outcomes than those first referred as inpatients [17]. The benefits of timely palliative care are discussed elsewhere [21].
Inpatient care
Inpatient palliative care has 2 major components: inpatient consultation teams, which offer expert recommendations for symptom control, support medical decision-making, and facilitate hospital discharges; and acute palliative care units, which provide intensive symptom management for patients in severe distress and comprehensive care planning for patients in the last weeks and days of life. Although most cancer centers in the USA have inpatient consultation teams, only 40% of NCI-designated cancer centers and 7% of non-NCI-designated cancer centers reported having acute palliative care units [6•). To date, studies examining the impact of inpatient palliative care services have focused on consultation teams only.
For patients who presented to an emergency room, the Palliative Care and Rapid Emergency Screening tool (P-CaRES) has been developed to facilitate early referral for inpatient specialist palliative care [22, 23]. Patients with a diagnosis of life-limiting illness (e.g., advanced cancer) and at least 2 of the following 5 criteria would benefit from a referral: ≥2 emergency room visits in 6 months, uncontrolled symptoms, functional decline, uncertainty regarding goals of care and/or caregiver burnout, and not surprised if patient would die in the next 12 months. Patients already seen by palliative care teams and presenting to an emergency room represent a unique population because they often have a poor functional status and may not desire aggressive life-prolonging measures. Paiva et al. developed a Palliative Care Triage System (PCTS) for use by emergency room nurses with 4 categories associated with hospital admission and survival [24].
In 2020, Scott et al. conducted a systematic review to examine the impact of hospital-based palliative care teams on post-discharge care and outcomes [25]. The investigators identified 15 studies involving 53,659 patients. These studies included 1 randomized clinical trial, 5 prospective studies (2 with a control group), and 9 retrospective studies (6 with a control group). A meta-analysis was not possible because of the heterogeneous design of the review. The authors concluded that inpatient palliative care consultations were associated with higher rates of community discharge, greater provision of services after discharge, improved care coordination, and lower rates of readmission. However, another systematic review focusing on palliative care transitions from acute care to community-based settings identified 8 studies and reported more heterogeneous findings [26].
The studies above mostly included patients with advanced solid tumors. In patients with hematologic malignancies, inpatient palliative care consultation is also beneficial. El-Jawahri et al. conducted a randomized controlled trial to compare inpatient palliative care consultation to routine oncologic care in 160 patients with hematologic malignancies undergoing autologous or allogeneic stem cell transplant. The primary outcome was quality of life at 2 weeks, which decreased in both groups with treatment; however, patients in the palliative care group had significantly less reduction in quality of life than did the control group. Furthermore, the symptom burden and levels of depression and anxiety were all significantly better in the palliative care group at 2 weeks and 3 months [27]. In a second randomized trial, El-Jawahri assigned 160 hospitalized patients undergoing intensive chemotherapy for acute myeloid leukemia to receive inpatient palliative care consultation or usual care. Patients’ quality of life and symptoms of anxiety, depression, and post-traumatic stress disorder were all significantly better with palliative care compared to usual care over the 24-week follow-up period [28].
Community-based palliative care
Community-based palliative care traditionally involves care teams coming to patients’ homes to conduct symptom and needs assessments, provide recommendations for various non-pharmacologic and pharmacologic interventions, assist with daily activities, offer counseling and education for patients and caregivers, and support self-management of symptoms. However, the advent of telemedicine and remote monitoring services has shifted how community-based palliative care is delivered, blurring the line between outpatient care and community-based care. A randomized trial examining the addition of telemedicine services to community-based palliative care in the Netherlands found that symptom distress was higher with than without telemedicine services; however, the study had important methodologic limitations [29]. Further research is needed to assess telemedicine services in the setting of community-based palliative care.
Hospital-at-home programs, in which selected, acute hospital-level services such as blood collection and the delivery of intravenous medications are provided at home, are also available and offer more intensive home care than is provided through traditional community-based palliative care programs [30, 31]. Another form of community-based palliative care, hospice care, is delivered predominantly at home in the USA. However, hospice care is considered distinct from non-hospice, community-based palliative care services because of health system and reimbursement policy differences. In other countries such as the UK and Canada, hospice care is provided more typically in a community-based, free-standing facility. Several systematic reviews on community-based palliative care include hospice programs [32].
Community-based palliative care services are intended for patients who are typically home-bound and thus have a poorer performance status and shorter expected survival. These programs offer an alternative to hospitalization and provide reassurance and support for patients who might otherwise need acute care visits. However, patients with acute medical issues or severe symptoms often still require admission to a hospital.
In a 2013 systematic review and meta-analysis, Luckett et al. examined the impact of specialist community-based palliative care on home death [33]. Nine studies were included. A meta-analysis showed that specialist palliative care with home nursing was associated with home death (odds ratio, 4.45; 95% CI, 3.24–6.11). However, when only the 2 high-quality studies were considered, the effect became non-significant (odds ratio, 1.40; 95% CI, 0.97–2.02).
Gomes et al. conducted a Cochrane systematic review and meta-analysis in 2013. In their study of the impact of community-based palliative care on patients with advanced diseases [34], the investigators examined 23 studies (including 16 randomized trials) that involved 37,561 patients and 4042 caregivers and found that community-based palliative care was associated with more home deaths (odds ratio, 2.21; 95% CI, 1.31–3.71) and better symptom control than was the usual care. However, the evidence for other outcomes such as physical function, quality of life, the caregiver burden, satisfaction with care, and the cost of care was less conclusive.
Another systematic review conducted in 2016 focused on the impact of specialized home-based palliative care for patients with advanced cancer [35]. Two interventional before-and-after studies and 6 longitudinal observational studies were included; no randomized trials were identified. The investigators concluded that symptom control improved over time in patients who received specialized palliative care; however, there was insufficient evidence for other outcomes.
In 2021, Gonzalez-Jaramillo and colleagues completed a systematic review to assess the impact of community-based palliative care on hospital use and health care costs [32]. Nineteen studies, involving 92,000 participants, were included. The study found that, compared to usual care, community-based palliative care was associated with a reduction in hospitalizations (13 of 14 studies), a shorter length of hospital stays (9 of 9 studies), fewer emergency department visits (5 of 7 studies), more home deaths (6 of 6 studies), and lower costs of care (mean, 36.3% savings; interquartile range, 28.8–51.8%).
In a 2021 Cochrane meta-analysis, Shepperd et al. examined the benefits of hospital-at-home programs for patients with advanced diseases who were at the end of life [31]. Four randomized clinical trials were included. The investigators concluded that, based on 2 studies involving 539 participants, patients receiving community-based end-of-life care had a higher likelihood of dying at home (relative risk, 1.3; 95% CI, 1.12, 1.52) than did patients receiving usual care. There was also a small increase in patient satisfaction at 1 month among the patients receiving home-based end-of-life care. The impact on other outcomes such as symptom control and health service costs was less uncertain. Further research is ongoing [36].
Taken together, the literature supports an association between home palliative care and home death [37]. Other outcomes with less consistent findings include improved symptom control and reduced hospitalizations and care costs. The heterogeneous findings could be explained by substantial variations in the service delivery models (in-person, telemedicine, hospital-at-home, and home hospice visits), intensity of visits, care team composition, patient populations, study designs, and outcome assessments. More high-quality research is needed.
Personalizing the setting of palliative care delivery: “Care anywhere, anytime”
Bringing palliative care to where patients are matters. With so many settings and variations in which specialized palliative care can be delivered, one commonly asked question is which form of palliative care is most effective. The reality is that many patients with advanced cancer will require care from outpatient, inpatient, and community-based palliative care settings at some point along their disease journey. Early on, outpatient clinics provide longitudinal supportive care concurrent with active disease-modifying treatments. Telemedicine visits can serve patients remotely to minimize their need to travel. When patients experience functional decline, community-based palliative care services can provide support and monitoring for patients at home. When patients develop acute symptomatic complications requiring admission, inpatient care consultation teams are essential for symptom management and goals-of-care discussions. For patients in severe distress, receiving care in a palliative care unit that provides intensive symptom control and facilitates complex discharge planning is ideal.
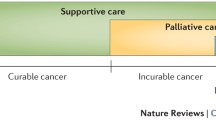
Teamwork matters. In an interdisciplinary palliative care team, each member contributes expertise and supports other team members. Similarly, in an integrated health care system, each branch of palliative care has a unique role to play in enhancing patient care and supporting the other branches (Fig. 1). For example, proper symptom management provided by the inpatient consultation team, thoughtful discharge planning, and telemedicine visits and/or community-based care after discharge may work together to prevent readmissions. Prognostic discussions in the outpatient setting to enhance patients’ understanding of their illnesses, coupled with goals-of-care discussions in inpatient visits, may reduce the use of chemotherapy and intensive care unit admissions in the last days of life [17, 38].

The 3 branches of comprehensive palliative care programs. The 3 major branches of comprehensive palliative care programs—inpatient, outpatient and community-based palliative care—are interdependent and work together to provide comprehensive supportive care to patients throughout the disease trajectory.
The dose of supportive care offered to patients matters. In an understaffed palliative care team, a nurse, rather than a psychologist or social worker, may need to provide some counseling for emotional distress, which is less than ideal. Similarly, in an underfunded palliative care program, 1 branch may overextend to compensate for a missing branch. In contrast, having all branches of a comprehensive palliative care program available to provide services allows patients to receive optimal care according to their needs and with minimal interruptions. Such a program would allow the intensity of supportive care to be optimally tailored to patients’ needs, which would theoretically promote more efficient use of health care resources.
The 3 main branches of specialist palliative care—outpatient, inpatient, and community-based care—are interdependent and work together to improve patient care along the disease continuum by providing optimal supportive care “anywhere, anytime” (Fig. 1). Health systems missing one of the branches need to compensate with overextending the other branches (inefficiently), supplement patient care with outside services, or risk patient care being jeopardized. For example, health systems without outpatient palliative care services and/or community-based care access are more likely to have a greater demand for acute care services, which are not only costly but also are considered to provide poorer quality of care. Thus, a comprehensive palliative care program that can provide access to all 3 branches of specialist palliative care is desirable.
Although a comprehensive palliative care program is likely to provide better patient care and cost savings than an attenuated program, it requires a large team and a high level of startup resources and thus may not be possible for health systems with limited resources. In such circumstances, inpatient palliative care consultation teams remain the backbone of palliative care because they require limited infrastructure and can support patients in acute distress. In health systems with additional resources, outpatient clinics can provide timely palliative care and can also house telemedicine services. The outpatient staffing and scope of services can be increased over time. Community-based palliative care and acute palliative care units are more resource-intensive but provide important support for patients in the last phase of life and are thus most in need. For programs without community-based palliative care services, the engagement of community partners is helpful. For example, cancer centers without community-based palliative care programs may still refer patients to home health agencies or hospices. Ultimately, the palliative care program should be personalized not only to patients but also to health care systems.
Multiple studies have found that, in addition to improving the quality of life and quality of care, palliative care can provide cost savings for health care systems [39, 40]. Most of these studies have been conducted in the inpatient and community-based care settings. They have demonstrated that specialist palliative care reduces the cost of care predominantly by reducing intensive interventions at the end of life [32, 41,42,43,44].
Summary
The goal of palliative care is to relieve suffering, improve patients’ quality of life, and enhance the quality of care. Because suffering is a multi-dimensional construct that starts from the time of diagnosis and varies in intensity over time, palliative care needs to be interdisciplinary, provided in a timely fashion, and available in different settings to provide access “anywhere, anytime.” Importantly, these 3 branches of specialist palliative care—outpatient, inpatient, and community-based care—are interdependent and work together to enhance patient care along the disease continuum by providing optimal supportive care. Further research is needed to examine novel models of palliative care in different health care settings.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Saunders C. The evolution of palliative care. J R Soc Med. 2001;94:430–2.
Mount BM. The problem of caring for the dying in a general hospital; the palliative care unit as a possible solution. Can Med Assoc J. 1976;115:119–21.
Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. New England Journal of Medicine. 2010;363:733–42.
Dalal S, Palla S, Hui D, et al. Association between a name change from palliative to supportive care and the timing of patient referrals at a comprehensive cancer center. The Oncologist. 2011;16:105–11.
Hui D, Cherny N, Latino N, Strasser F. The ‘'critical mass’' survey of palliative care programme at ESMO designated centres of integrated oncology and palliative care. Ann Oncol. 2017;28:2057–66.
• Hui D, De La Rosa A, Chen J, et al. State of palliative care services at US cancer centers: an updated national survey. Cancer. 2020;126:2013–23 This national survey highlights the state of palliative care in US cancer centers.
Reddy A, Arthur J, Dalal S, et al. Rapid transition to virtual care during the COVID-19 epidemic: experience of a supportive care clinic at a tertiary care cancer center. J Palliat Med. 2021;24:1467–73.
•• Bajwah S, Oluyase AO, Yi D, et al. The effectiveness and cost-effectiveness of hospital-based specialist palliative care for adults with advanced illness and their caregivers. Cochrane Database Syst Rev. 2020;9:Cd012780 This recent Cochrane meta-analysis examines specialist palliative care in its different forms and its impact on health- related quality of life, symptom burden, patient satisfaction with care, and dying in preferred place of death.
Gaertner J, Siemens W, Meerpohl JJ, et al. Effect of specialist palliative care services on quality of life in adults with advanced incurable illness in hospital, hospice, or community settings: systematic review and meta-analysis. BMJ. 2017;357:j2925.
Kavalieratos D, Corbelli J, Zhang D, et al. Association between palliative care and patient and caregiver outcomes: a systematic review and meta-analysis. JAMA. 2016;316:2104–14.
• Hui D, Hannon BL, Zimmermann C, Bruera E. Improving patient and caregiver outcomes in oncology: team-based, timely, and targeted palliative care. CA Cancer J Clin. 2018;68:356–76 This article highlights the evidence to support timely palliative care, the key components for a successful program, and evolving models of care in the outpatient setting.
Mir O, Ferrua M, Fourcade A, et al. Digital remote monitoring plus usual care versus usual care in patients treated with oral anticancer agents: the randomized phase 3 CAPRI trial. Nat Med. 2022;28:1224–31.
Pimentel LE, Yennurajalingam S, Chisholm G, et al. The frequency and factors associated with the use of a dedicated Supportive Care Center Telephone Triaging Program in patients with advanced cancer at a comprehensive cancer center. J Pain Symptom Manage. 2015;49:939–44.
Haun MW, Estel S, Rucker G, et al. Early palliative care for adults with advanced cancer. Cochrane Database Syst Rev. 2017;6:Cd011129.
Fulton JJ, LeBlanc TW, Cutson TM, et al. Integrated outpatient palliative care for patients with advanced cancer: a systematic review and meta-analysis. Palliat Med. 2019;33:123–34.
Hoerger M, Wayser GR, Schwing G, et al. Impact of interdisciplinary outpatient specialty palliative care on survival and quality of life in adults with advanced cancer: a meta-analysis of randomized controlled trials. Ann Behav Med. 2019;53:674–85.
Hui D, Kim SH, Roquemore J, et al. Impact of timing and setting of palliative care referral on quality of end-of-life care in cancer patients. Cancer. 2014;120:1743–9.
Jang RW, Krzyzanowska MK, Zimmermann C, et al. Palliative care and the aggressiveness of end-of-life care in patients with advanced pancreatic cancer. J Natl Cancer Inst. 2015;107.
de Oliveira Valentino TC, Paiva CE, Hui D, et al. Impact of palliative care on quality of end-of-life care among Brazilian patients with advanced cancers. J Pain Symptom Manage. 2020;59:39–48.
Ziegler LE, Craigs CL, West RM, et al. Is palliative care support associated with better quality end-of-life care indicators for patients with advanced cancer? A retrospective cohort study. BMJ Open. 2018;8:e018284.
Hui D, Heung Y, Bruera E. Timely palliative care: personalizing the process of referral. Cancers (Basel). 2022:14.
Bowman J, George N, Barrett N, et al. Acceptability and reliability of a novel palliative care screening tool among emergency department providers. Acad Emerg Med. 2016;23:694–702.
George N, Barrett N, McPeake L, et al. Content validation of a novel screening tool to identify emergency department patients with significant palliative care needs. Acad Emerg Med. 2015;22:823–37.
Paiva CE, Seriaco F, de Oliveira MA, et al. The palliative care triage system in advanced cancer emergency care: development and initial validation. BMJ Support Palliat Care. 2022.
Scott M, Shaver N, Lapenskie J, et al. Does inpatient palliative care consultation impact outcomes following hospital discharge? A narrative systematic review. Palliat Med. 2020;34:5–15.
Saunders S, Killackey T, Kurahashi A, et al. Palliative care transitions from acute care to community-based care-a systematic review. J Pain Symptom Manage. 2019;58:721–734.e721.
El-Jawahri A, LeBlanc T, VanDusen H, et al. Effect of inpatient palliative care on quality of life 2 weeks after hematopoietic stem cell transplantation: a randomized clinical trial. JAMA. 2016;316:2094–103.
El-Jawahri A, LeBlanc TW, Kavanaugh A, et al. Effectiveness of integrated palliative and oncology care for patients with acute myeloid leukemia: a randomized clinical trial. JAMA Oncol. 2021;7:238–45.
Hoek PD, Schers HJ, Bronkhorst EM, et al. The effect of weekly specialist palliative care teleconsultations in patients with advanced cancer -a randomized clinical trial. BMC Med. 2017;15:119.
Grande GE, Todd CJ, Barclay SI, Farquhar MC. Does hospital at home for palliative care facilitate death at home? Randomised controlled trial. Bmj. 1999;319:1472–5.
Shepperd S, Gonçalves-Bradley DC, Straus SE, Wee B. Hospital at home: home-based end-of-life care. Cochrane Database Syst Rev. 2021;3:Cd009231.
Gonzalez-Jaramillo V, Fuhrer V, Gonzalez-Jaramillo N, et al. Impact of home-based palliative care on health care costs and hospital use: a systematic review. Palliat Support Care. 2021;19:474–87.
Luckett T, Davidson PM, Lam L, et al. Do community specialist palliative care services that provide home nursing increase rates of home death for people with life-limiting illnesses? A systematic review and meta-analysis of comparative studies. J Pain Symptom Manage. 2013;45:279–97.
Gomes B, Calanzani N, Curiale V, et al. Effectiveness and cost-effectiveness of home palliative care services for adults with advanced illness and their caregivers. Cochrane Database Syst Rev 2013; Cd007760.
Nordly M, Vadstrup ES, Sjøgren P, Kurita GP. Home-based specialized palliative care in patients with advanced cancer: a systematic review. Palliat Support Care. 2016;14:713–24.
Nipp RD, Shulman E, Smith M, et al. Supportive oncology care at home interventions: protocols for clinical trials to shift the paradigm of care for patients with cancer. BMC Cancer. 2022;22:383.
Gomes B, Calanzani N, Higginson IJ. Benefits and costs of home palliative care compared with usual care for patients with advanced illness and their family caregivers. Jama. 2014;311:1060–1.
Hui D, Nortje N, George M, et al. Impact of an interdisciplinary goals-of-care program among medical inpatients at a comprehensive cancer center during the COVID-19 pandemic: a propensity score analysis. J Clin Oncol. 2022;Jco2200849.
Mathew C, Hsu AT, Prentice M, et al. Economic evaluations of palliative care models: a systematic review. Palliat Med. 2020;34:69–82.
May P, Normand C, Morrison RS. Economics of palliative care for cancer: interpreting current evidence, mapping future priorities for research. J Clin Oncol. 2020;38:980–6.
Yadav S, Heller IW, Schaefer N, et al. The health care cost of palliative care for cancer patients: a systematic review. Support Care Cancer. 2020;28:4561–73.
May P, Normand C, Cassel JB, et al. Economics of palliative care for hospitalized adults with serious illness: a meta-analysis. JAMA Internal Medicine 2018; 178:820-9.
Morrison RS, Penrod JD, Cassel JB, et al. Cost savings associated with US hospital palliative care consultation programs. Archives of Internal Medicine. 2008;168:1783–90.
May P, Garrido MM, Cassel JB, et al. Prospective cohort study of hospital palliative care teams for inpatients with advanced cancer: earlier consultation is associated with larger cost-saving effect. J Clin Oncol. 2015;33:2745–52.
Acknowledgements
We thank Laura L. Russell, scientific editor, Research Medical Library, the University of Texas MD Anderson Cancer Center, for editing this article.
Funding
D.H. is supported in part by grants from the National Cancer Institute (R01CA214960; R01CA225701; R01CA231471).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Palliative and Supportive Care
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Hui, D., Paiva, B.S.R. & Paiva, C.E. Personalizing the Setting of Palliative Care Delivery for Patients with Advanced Cancer: “Care Anywhere, Anytime”. Curr. Treat. Options in Oncol. 24, 1–11 (2023). https://doi.org/10.1007/s11864-022-01044-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11864-022-01044-1