
Abstract
Aims
Management of patients with a single CHA2DS2-VASc score risk factor is controversial. We attempt to identify the “truly low risk” AF patients who will not benefit from oral anticoagulation (OAC) treatment.
Methods
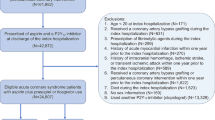
Retrospective cohort analysis, all incident non-valvular AF (NVAF) cases between 2004 and 2015, and age 21 and older, with up to one thromboembolic risk factor besides sex (CHA2DS2-VASc score of up to 1 for men and up to 2 for women). A “low risk” score was created for these patients using a logistic regression model on the incidence of stroke within 30–2500 days following the NVAF diagnosis.
Results
We identified 15,621 patients. Average age was 53.7 ± 12.3 years, 56.6% male. Mean follow-up was 5.5 years. Significant predictors of ischemic stroke were age 65–74 and diabetes (2 points each), hypertension, vascular disease, and chronic kidney disease stage 2–3 (1 point each). Stroke incidence ranged from 0.8% for score 0 and up to 3.4% for scores ≤ 2. Odds ratio for stroke among patient group with a score ≤ 2 was 4.3 (2.9–6.6) compared with score 0. Our risk score’s area-under-the-curve (AUC) for prediction of stroke was 0.68 (0.65–0.71), compared with 0.60 (0.57–0.62) for the CHAD2S2-VASc score, within this low-risk group.
Conclusion
Patients considered at low or intermediate risk using traditional risk stratification schemes, with ≥ 2 points using this proposed low-risk index (65–74 years old, diabetics or a combination of chronic renal failure and an additional risk factor), had an overall stroke risk that may justify anticoagulation therapy.


Similar content being viewed by others


Abbreviations
- AF:
-
Atrial fibrillation
- CHA2DS2-VASc:
-
Congestive heart failure, hypertension, age ≥ 75, diabetes, prior stroke, vascular disease, age 65–74, and female sex category
- CHF:
-
Congestive heart failure
- CHS:
-
Clalit Health Services
- CI:
-
Confidence interval
- OR:
-
Odds ratio
- INR:
-
International normalized ratio
- NVAF:
-
Non-valvular atrial fibrillation
References
Chugh SS, Havmoeller R, Narayanan K et al (2014) Worldwide epidemiology of atrial fibrillation: a Global Burden of Disease 2010 Study. Circulation 129:837–847
Hindricks G, Potpara T, Dagres N et al (2021) 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 42:373–498
January CT, Wann LS, Calkins H et al (2019) 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines and the heart rhythm society in collaboration with the society of thoracic surgeons. Circulation 140:e125–e151
January CT, Wann LS, Alpert JS et al (2014) 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the American College of Cardiology/American Heart Association task force on practice guidelines and the heart rhythm society. Circulation
Friberg L, Skeppholm M, Terent A (2015) Benefit of anticoagulation unlikely in patients with atrial fibrillation and a CHA2DS2-VASc score of 1. J Am Coll Cardiol 65:225–232
Lip GY, Skjoth F, Rasmussen LH, Larsen TB (2015) Oral anticoagulation, aspirin, or no therapy in patients with nonvalvular AF with 0 or 1 stroke risk factor based on the CHA2DS2-VASc score. J Am Coll Cardiol 65:1385–1394
Chao TF, Liu CJ, Wang KL et al (2015) Should atrial fibrillation patients with 1 additional risk factor of the CHA2DS2-VASc score (beyond sex) receive oral anticoagulation? J Am Coll Cardiol 65:635–642
Olesen JB, Torp-Pedersen C (2015) Stroke risk in atrial fibrillation: do we anticoagulate CHADS2 or CHA2DS2-VASc >/=1, or higher? Thromb Haemost 113:1165–1169
Levey AS, Stevens LA, Schmid CH et al (2009) A new equation to estimate glomerular filtration rate. Ann Intern Med 150:604–612
Lip GYH, Collet JP, Caterina R et al (2017) Antithrombotic therapy in atrial fibrillation associated with valvular heart disease: a joint consensus document from the European Heart Rhythm Association (EHRA) and European Society of Cardiology Working Group on Thrombosis, endorsed by the ESC Working Group on Valvular Heart Disease, Cardiac Arrhythmia Society of Southern Africa (CASSA), Heart Rhythm Society (HRS), Asia Pacific Heart Rhythm Society (APHRS), South African Heart (SA Heart) Association and Sociedad Latinoamericana de Estimulacion Cardiaca y Electrofisiologia (SOLEACE). Europace 19:1757–1758
Lip GY, Nieuwlaat R, Pisters R et al (2010) Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest 137:263–272
Olesen JB, Lip GY, Hansen ML et al (2011) Validation of risk stratification schemes for predicting stroke and thromboembolism in patients with atrial fibrillation: nationwide cohort study. BMJ 342:d124
Friberg L, Rosenqvist M, Lip GY (2012) Net clinical benefit of warfarin in patients with atrial fibrillation: a report from the Swedish atrial fibrillation cohort study. Circulation 125:2298–2307
Singer DE, Chang Y, Fang MC et al (2009) The net clinical benefit of warfarin anticoagulation in atrial fibrillation. Ann Intern Med 151:297–305
Friberg L, Rosenqvist M, Lip GY (2012) Evaluation of risk stratification schemes for ischaemic stroke and bleeding in 182 678 patients with atrial fibrillation: the Swedish Atrial Fibrillation cohort study. Eur Heart J 33:1500–1510
Funding
The authors are employees of Clalit Health Services and Clalit Health Services Research Institute which received funding from Pfizer Inc. to conduct this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
The study has been approved by the Clalit health service IRB committee.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Highlights
• Preventive treatment for atrial fibrillation patients with high thromboembolic risk is based on chronic oral anticoagulation treatment.
• The treatment of patients with atrial fibrillation and low to medium thromboembolic risk (CHADS-VASc score of 1) is controversial.
• Within low-risk patients, patients 65–74 years of age and diabetics as a single risk factor are at higher risk for stroke.
• The combination of chronic kidney disease and hypertension or vascular disease increases stroke risk as well.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Arnson, Y., Senderey, A.B., Hoshen, M. et al. Identifying patients with atrial fibrillation with a single CHA2DS2-VASC risk factor who are at higher risk of stroke. Ir J Med Sci 191, 705–711 (2022). https://doi.org/10.1007/s11845-021-02618-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11845-021-02618-y