
Abstract
Background and objective
This study aimed to evaluate the sleep patterns of students and employees working onsite versus those working from home during the COVID-19 pandemic using actigraphy.
Methods
A total of 75 students/employees (onsite: N = 40, home-office: N = 35; age range: 19–56 years; 32% male; 42.7% students, 49.3% employees) were studied between December 2020 and January 2022 using actigraphy, a sleep diary, and an online questionnaire assessing sociodemographics and morningness–eveningness. Independent-sample t-tests, paired-sample tests, and a multivariate general linear model adjusting for age (fixed factors: sex and work environment) were applied.
Results
Overall, onsite workers had significantly earlier rise times (7:05 [SD: 1:11] versus 7:44 [1:08] hours) and midpoints of sleep (2:57 [0:58] versus 3:33 [0:58] hours) on weekdays compared to home-office workers. Sleep efficiency, sleep duration, variability of sleep timing, and social jetlag did not differ between the groups.
Discussion
Home-office workers showed a delay in sleep timing that did not affect any other sleep parameters such as sleep efficiency or nighttime sleep duration. The work environment had only marginal impact on sleep patterns and thus sleep health in this sample. Sleep timing variability did not differ between groups.
Zusammenfassung
Hintergrund und Ziel
In dieser Studie wurde das Schlafverhalten von Studierenden und Angestellten, die während der COVID-19-Pandemie vor Ort oder von zu Hause aus arbeiteten, aktigraphisch untersucht.
Methoden
Untersucht wurden 75 Studierende/Angestellte (vor Ort: N = 40, Home-Office: N = 35, Alter: 19–56 Jahre, 32 % männlich, 42,7 % Studierende, 49,3 % Angestellte) zwischen Dezember 2020 und Januar 2022 mittels Aktigraphie, Schlaftagebuch und Online-Fragebogen zur Erfassung von soziodemographischen Daten und Morningness-Eveningness. Verwendet wurden t‑Tests für unabhängige Stichproben, Tests für gepaarte Stichproben sowie ein altersbereinigtes multivariates allgemeines lineares Modell (feste Faktoren: Geschlecht und Arbeitsumgebung).
Ergebnisse
Insgesamt standen die Vor-Ort-Arbeitenden an Wochentagen signifikant früher auf (7:05 [SD 1:11] vs. 7:44 [1:08] Stunden) und hatten einen signifikant früheren Schlafmittelpunkt (2:57 [0:58] vs. 3:33 [0:58] Stunden) als die im Home-Office-Arbeitenden. Schlafeffizienz, Schlafdauer, Schlafvariabilität und sozialer Jetlag unterschieden sich nicht zwischen den Gruppen.
Diskussion
Im Home-Office arbeitende Teilnehmende zeigten eine Verzögerung des Schlafzeitpunkts, die sich nicht auf andere Schlafparameter, wie Schlafeffizienz oder nächtliche Schlafdauer, auswirkte. Die Arbeitsumgebung hatte in dieser Stichprobe nur einen geringen Einfluss auf das Schlafverhalten und damit auf die Schlafgesundheit. Die Variabilität der Schlafzeiten unterschied sich nicht zwischen den Gruppen.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Sleep is critical for regular functioning of physical and mental health in humans [1]. It is important for maintaining long-term health through physical/cerebral functioning (sleep deprivation causes, e.g., an increased prevalence of noncommunicable diseases such as obesity [2] or cardiovascular problems [3]), and short term health by, e.g., minimizing the risk of traffic accidents related to drowsiness [4, 5].
With the onset of the coronavirus disease 2019 (COVID-19) pandemic, mental stress increased enormously due to fears about the future, about relatives, or about one’s own health. Since stress and anxiety have a strong negative impact on sleep, some research groups have reported a deterioration in sleep health (see [6] for a review). In addition, increased workloads in some professions (e.g., medical staff) have also taken their toll, leading to more sleep problems and poorer sleep health [6].
The pandemic changed the professional situation of students and employees. Remote working (hereinafter also referred to as the situation of students studying at home) as well as the closure of many business sectors (e.g., body-related services) affected everyday life, including sleep. It was shown that the shift to remote working and the associated later work start allowed participants to adjust their sleep times to their own circadian rhythm. As a result, students and employees were able to synchronize their biological and social clocks, thereby improving sleep health (e.g., [7,8,9,10,11,12,13,14,15]). In addition to the positive effects of synchronizing social and biological timing, on-demand teaching has been shown to lead to a loss of sleep timing regularity [14], which, in turn, can have negative effects on sleep and overall health (e.g., [16, 17]). In contrast, Ramírez-Contreras and colleagues [18] reported that the hybrid system of virtual and face-to-face activity was beneficial for students in terms of sleep regularity and eating habits, resulting in longer sleep duration on weekdays and reductions in sleep deprivation. Furthermore, increased screen time due to remote working may also have disrupted and delayed sleep onset due to more blue light exposure (e.g., [19, 20]) and less outdoor light exposure [21]. However, increased time spent outdoors in home-office workers has also been reported [22]. So far, there are few data on the effect of the working environment on sleep patterns during the COVID-19 pandemic in Germany.
The present study builds on the preliminary data and literature available and compares the sleep patterns of participants in two different working environments. We hypothesized later/more irregular sleep timing and midpoints of sleep, longer nighttime sleep duration, worse sleep efficiency, and less social jetlag (SJL) in home-office compared to onsite-working students/employees.
Methods
Setting
This study was approved by the Eberhard Karls University’s ethics committee (Faculty of Economics and Social Sciences: no. A.Z.: A2.5.4-157_ns).
Data collection
Data were collected from December 14, 2020, to January 18, 2022. Participants were recruited through university mailing lists and social media postings (Facebook, Instagram, WhatsApp). The study included a questionnaire that was available online on the SoSciSurvey platform (https://www.soscisurvey.de/). This hosting platform complies with European Union data protection regulations. Potential study participants were informed about the voluntary nature of participation, the possibility to stop data collection at any time without consequences, and the study compensation of 25 € in cash. Informed consent was obtained before data collection began. Exclusion criteria were shiftwork, participants who planned to travel across time zones during data collection, and participants who were not fluent in German.
Variables and instruments
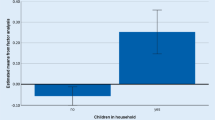
Participants reported information on their demographics (such as the work environment (“working onsite,” hereafter: “onsite group”; and “working from home,” hereafter: “home-office group”), age, sex, number of children in their household, occupation), details of their sleep behavior, and a morningness–eveningness questionnaire (the Morningness–Eveningness Stability Scale improved [MESSi]).
MESSi
The MESSi consists of three subscales: morning affect (MA), eveningness (EV), and distinctness (DI). MA is designed to measure the affective component of morning orientation, while EV measures the affective component of evening orientation. In comparison to the diurnal changes measured by the MA and EV subscales, the DI subscale measures fluctuating changes in the expression of MA and EV [23].
Actigraphy
Participants were asked to wear an ActiGraph (GT3X+, ActiGraph, Pensacola, FL, USA) for 7 consecutive days in order to measure sleep–wake patterns. The device is worn on the nondominant wrist similar to a wristwatch. At the end of the measurement week, participants returned their ActiGraphs and the data were downloaded using the accompanying software (ActiLife). Activity counts were collected in 1‑min epochs over a continuous period of 1 week (7 × 24 h). Any recordings that did not meet the minimum requirements of a) at least 10 h of valid signal during waking hours and b) a total of at least 4 valid days were excluded. Sleep–wake patterns were scored manually using the ActiLife software as described by Mitchell and colleagues [24]. Briefly, sleep onset and offset times were identified by diary report and observation of a sharp decrease/increase in activity. If there were discrepancies of more than 30 min between the sleep diary report and the decrease/increase in activity counts measured by the ActiGraph, sleep phases were determined visually based on the activity changes. We used the Cole–Kripke algorithm to estimate sleep and wake periods [25]. Non-wearing times were determined using the Troiano algorithm and compared with the sleep diary [26].
Sleep diary
Participants completed a sleep diary during the week of actigraphic monitoring. Participants were asked to note bedtimes, naps during the day, awakenings during the night (duration and frequency), and times when the ActiGraph was taken off (e.g., to take a shower).
Midpoint of sleep as a measure of chronotype
As a second measure of chronotype the corrected midpoint of sleep (MSFsc) as proposed by Roenneberg and colleagues was used [27]. This chronotype measure is based on clock time but adjusts for average individual sleep need [28]. It was shown to be a stable measure of chronotype during the COVID-19 pandemic in a similar German sample from Baden-Württemberg [13]. Throughout this manuscript the abbreviation “MPOS” represents “midpoint of sleep,” while in the following formula, “SDu” stands for “average sleep duration”:
Social jetlag
SJL is a parameter to describe the discrepancy between a person’s social and biological clocks due to circadian preferences [29]. Weekend sleep patterns are thought to reflect the internal biological clock, whereas weekday sleep patterns reflect the social clock. SJL is calculated by subtracting the midpoint of sleep on workdays from the midpoint of sleep on days off:
Sleep efficiency
Sleep efficiency is calculated by dividing the amount of time spent asleep (in minutes) by the total amount of time in bed (in minutes).
Sleep time variability
The variability in sleep times was compared between the groups. This was done by calculating the standard deviation of sleep times for each participant and using this to calculate a group mean. The result shows the average standard deviation of sleep times and is considered the variability of sleep timing in the group.
Statistical analyses
We further analyzed the actigraphy data using pyActigraphy [30], an open-source Python actigraphy analysis and visualization framework. In addition, averages of various sleep parameters were calculated for each subject using the Python data analysis library Pandas [31]. To calculate time averages after midnight, e.g., sleep onset time and midpoint of sleep, we added 24 h to times below an appropriate pivot element before calculating the mean, and then subtracted 24 h afterwards, if necessary. The software and a detailed description are available as open source at https://github.com/spuetz/actigraphy.git. Statistical analysis of the actigraphy and questionnaire data was performed using SPSS 29.0 software (IBM Corp., Armonk, NY, USA). Independent-sample t-tests and paired-sample tests were calculated to compare inter-and intra-individual differences. Furthermore, a multivariate general model was calculated with sex and work environment as fixed factors and age as a covariate to control the reliability of the t-tests. Kolmogorov–Smirnov and Shapiro–Wilk tests were used to test the normal distribution of the MSFsc variable. Levine tests indicated that equal variances could be assumed. Pearson’s chi-squared test was used for descriptive group comparisons.
Results
Descriptive group statistics are presented in Table 1. Exploratory data analysis was performed to identify outliers in the age variable, as this variable has a strong influence on other variables. Outlier limits were defined as ±3 standard deviations from the mean value. Two cases were excluded in each group. This reduced the original sample size from N = 79 to N = 75. Overall, the home-office group was significantly younger than the onsite group. Significantly more participants were students in the home-office group compared to the onsite group. We did not see any difference between groups regarding children in the household or chronotype. The sleep timing variability did not differ between the groups. In terms of intra-individual differences in the variability of sleep times, the onsite group had the lowest standard deviation of 0.17 h for bedtimes and also the highest of 2.32 h. For rise times, the minimum and maximum were 0.2 h and 2.07 h (Table 1). In the home-office group, the minimum for bedtime was 0.2 h and the maximum was 1.9 h, while the rise times were 0.25 h and 2.1 h respectively (see Table 1).
Comparisons of sleep patterns are shown in Table 2. No differences were seen in total time in bed, sleep efficiency, and total sleep time on weekdays, weekends, and all days. The home-office group went to bed, reached the midpoint of sleep, and got up significantly later than the onsite group on weekdays. Interestingly, sleep parameters did not differ between groups at weekends. Also, the variability of sleep timing (standard deviations of sleep timing, Table 1) did not differ between the groups. Both groups showed a SJL of about 1 h, which was not significantly different. In addition, there was no difference in chronotype measured by the MESSi scales MA/EV/DI (Table 1) or MSFsc (Table 2) between the two groups. For both the onsite and home-office groups, the Kolmogorov–Smirnov test and the Shapiro–Wilk test indicated a normal distribution of the MSFsc.
As age differed significantly between the onsite and home-office groups (30.3 versus 25.8 years, p = 0.01), a multivariate general linear model adjusting for age was applied (fixed factors: sex and work environment) (Table 3).
In comparison with the independent-sample test (Table 2), the general linear model confirmed the significant findings. The only exception was the variable “average rise time workdays,” which was no longer significant in the general linear model.
Sleep parameters on weekdays were also compared with weekend days to investigate intra-individual differences within each group using paired-sample t-tests (Table 4). Intra-individual differences were found in both the onsite and home-office groups. The sleep parameters of the onsite group differed significantly between weekdays and weekend days with regard to sleep efficiency, bedtime, total sleep time, rise time, and midpoint of sleep. The home-office group differed in the same sleep parameters except for total sleep time.
Onsite workers had a higher sleep efficiency on weekdays compared to weekends, while home-office workers had a higher sleep efficiency on weekends compared to weekdays. Average bedtime and midpoint of sleep were significantly later at weekends compared to weekdays for both groups.
Discussion
In summary, it was found that onsite workers had significantly earlier sleep timing and midpoints of sleep on weekdays compared to home-office workers, whereas there were no clinically meaningful differences regarding sleep efficiency, sleep duration, and variability in sleep timing. Importantly, also SJL did not differ between the groups. The results of the group comparison showed that the onsite group was significantly older than the home-office group. The group means differed by 4.5 years. This age difference is particularly important when considering the present results. Chronotype, as an individual difference trait, is subject to changes in expression over the course of a person’s life [32]. While young children tend to be morning types, this tendency changes strongly during adolescence [32]. Adolescents show a distinct delay in chronotype, peaking at the age of 20 years [27]. With the end of adolescence, the daytime preference shifts again and begins to advance. Roenneberg and colleagues [27] showed a continuous advancement of chronotype from the age of 20 until about 65 years. There is also a steeper regression line between the ages of 20 and 45 years than between 45 and 65 years. Most adults do not belong to an extreme chronotype and are therefore described as neither type [32]. In the sample of Randler and colleagues [32], a distribution of 21.1% evening, 71.7% neither, and 7.2% morning type was reported for the 26-year-old subjects. Among the 30-year-old subjects, 11.9% were classified as evening type, 74.8% as neither, and 13.3% as morning type. This means that the 30-year-old subjects were 9.2% less likely to be classified as evening type than the 26-year-old subjects. As the average age of the present sample groups differed by about 4.5 years (mean 25.8 years in home-office, mean 30.3 years in onsite), it could be assumed that also the chronotypes differ significantly from each other. Participants in the home-office group may therefore be more evening oriented, reflecting a higher proportion of evening types in this group than in the onsite group.
In this study two different measures of chronotype were used (MSFsc: clock time-based measure, MESSi: continuous morningness-eveningness measure). The analysis of the MSFsc and the MESSi showed no significant differences between the groups. Therefore, the expression of chronotype did not differ between the groups.
Regarding the MSFsc variable, Roenneberg and colleagues [33] described a comparable shape and width of the distribution in all age groups, with a varying mean value. Graphical comparison of the group histograms (see Supplement 1) with the expected values ([33], N ≥ 55,000) showed that the distribution in the home-office group had a similar shape. In the onsite group, two equally high peaks existed, one at 3:00 a.m. and one at 4:30 a.m., showing the shape of the distribution to be different from the reference. In the sample of Roenneberg and colleagues [33], the 26-year-old subjects showed peaks at around 4:45 a.m. compared to 4:17 a.m. for the home-office group. For the 30-year-old participants, Roenneberg and colleagues [33] reported an average MSFsc of approximately 4:30 a.m., compared to 3:51 a.m. for the onsite group. Taken together, these two discrepancies led us to consider the MSFsc of the onsite group to be unrepresentative.
In summary, a) the expected distribution of chronotype based on the age groups of the samples and b) the finding that the distribution of chronotype in the onsite group cannot be considered representative suggest that the chronotypes of the groups can generally be expected to differ. The younger group would normally have a higher prevalence of evening types/more pronounced eveningness, although this was not the case in the present samples.
Increased eveningness is associated with a higher risk of SJL. SJL has repeatedly been shown to be particularly detrimental to public health (e.g., cardiovascular outcomes, psychiatric disorders, obesity [34]). However, softer factors such as productivity at work are also significantly affected by SJL. To test whether the measured SJL in the home-office group was within the expected range, the results were compared to an earlier sample of the authors’ research group [13]. In that study, only people who worked in home-office during the COVID-19 pandemic had been surveyed. The mean age of the sample was reported to be ~ 28.6 years (SD: ~ 10.5 years), which was not different compared to the sample of the present study (p = 0.11; Supplement 2). With regard to SJL, the means of the present home-office group (0.80, SD: 0.73 h) and the previous sample (0.82; SD: 0.70 h) were also not significantly different (p = 0.87; Supplement 2). Furthermore, the chronotype within the two groups measured by MSFsc did not differ (p = 0.21; Supplement 2). It can therefore be assumed that the SJL in the present sample is representative for this age group working from home. In another sample of the same age who were not working from home, the SJL was almost 1 h higher (1.78 h) compared to the present sample with 0.8 h [35]. It could be postulated that the implementation of home-office might potentially be beneficial for young people to reduce SJL. The onsite group had an average SJL of 1.03 h, which was also compared to other samples in the current literature. As no age-matching sample could be found in the literature, the present results were compared to slightly younger and older samples. Both showed a meaningful but equal age difference compared to the present sample. Interestingly, the SJL (1.4 ± 1.0, [36]; 1.33 ± 0.88 h, [37]) of the two studies did not significantly differ (p = 0.42, t = 0.78, df = 727, Standard Error of Difference (SED) = 0.09). Therefore, these results were used as representative reference values for SJL in the current sample. Even the value closer to the current study [37] differed significantly from the SJL reported herein (p = 0.04, t = 2.07, df = 637, SED = 0.15; Supplement 2). This led to the conclusion that the SJL of the onsite group cannot be considered representative, as it was significantly below the expected range.
Although the SJL of the present two study groups were not significantly different, there was a tendency towards lower SJL in the home-office group. This tendency was reinforced by an overrepresentation of low SJL in the onsite group, while the home-office group showed more similar values to age-comparable samples. Therefore, the current results suggest that working from home might help to reduce SJL.
The present study differs from the authors’ previous studies which examined only home-office participants and not two samples in different working environments. As spatial flexibility, in addition to temporal flexibility [14], may play a role in the increasing irregularity of students’ sleep schedules, a possible relationship was investigated here.
The sleep timing of the two groups on workdays differed significantly. The home-office group went to bed later and also got up later. However, both groups had similar fluctuations regarding sleep timing variability and no difference in overall nightly sleep duration. Thus, home-office had no negative influence on sleep variability and duration in this sample. There was also no influence of spatial flexibility/working environment on the loss of sleep duration/regularity observed. Instead, data support the hypothesis that the ability to work with unrestricted temporal flexibility is the main influencing factor of the increased sleep timing regularity in students, as discussed in one of the authors’ previous studies [14] by excluding another possible influencing factor.
Sleep efficiency did not differ between the two groups. However, a difference within the groups could be detected. In the onsite group, sleep efficiency was higher on weekdays than at weekends. The opposite was true for the home-office group, where sleep efficiency was higher at weekends. The reason for this could be explained by the way the sleep efficiency variable is calculated. On weekdays, participants in the onsite group could have either gotten up immediately after waking up (e.g., because of the increased pressure to get up on time in order to commute to work compared to the weekend) or gone straight to sleep after going to bed (e.g., because of the increased exhaustion from onsite work with probably fewer breaks compared to the weekend). This would explain the high ratio of total sleep time to time in bed, which corresponds to a higher sleep efficiency. At the weekend, on the other hand, they may have stayed in bed even longer although they were already awake, or it took longer for them to fall asleep, resulting in lower sleep efficiency. In contrast, the opposite was true for the home-office group, with a higher sleep efficiency at weekends compared to weekdays. Although statistically significant, this effect was small and not clinically meaningful.
Conclusion
In summary, it was found that home-office workers had a delay in sleep timing that did not have a clinically meaningful effect on any other sleep parameter such as sleep efficiency or nightly sleep duration. Compared to values in the current literature, SJL seemed to be reduced in the home-office group. Overall, the work environment had only marginal impact on sleep patterns and thus sleep health in this sample. Sleep timing variability did not differ between groups.
Limitations and strengths
Strengths of the study were the objective data collection via actigraphy and the assessment of different sleep variables covering sleep quantity, quality, and circadian patterns. The results of the study were limited by the fact that the sample was relatively small and there was a significant age difference between the groups. In addition, students were overrepresented in the home-office group. Moreover, although the data were collected during the same seasons, which reduces seasonal effects, they were collected over a long period of time, this may have influenced the data in terms of the evolution of the pandemic (different severity of lockdown regimes, psychological effects due to different familiarity and understanding).
References
Ramar K, Malhotra RK, Carden KA et al (2021) Sleep is essential to health: an American Academy of Sleep Medicine position statement. J Clin Sleep Med 17(10):2115–2119
Sun W, Huang Y, Wang Z, Yu Y, Lau A, Ali G, Shan G (2015) Sleep duration associated with body mass index among Chinese adults. Sleep Med 16(5):612–616
Sabanayagam C, Shankar A (2010) Sleep duration and cardiovascular disease: results from the National Health Interview Survey. Sleep 33(8):1037–1042
Hillman DR, Lack LC (2013) Public health implications of sleep loss: the community burden. Med J Aust 199:S7–S10
Philip P, Chaufton C, Orriols L, Lagarde E, Amoros E, Laumon B, Sagaspe P (2014) Complaints of poor sleep and risk of traffic accidents: a population-based case-control study. Plos One 9(12):e114102
Lin YN, Liu ZR, Li SQ, Li CX, Zhang L, Li N, Li QY (2021) Burden of sleep disturbance during COVID-19 pandemic: a systematic review. NSS 13:933
Conroy DA, Hadler NL, Cho E, Moreira A, MacKenzie C, Swanson LM, Goldstein CA (2021) The effects of COVID-19 stay-at-home order on sleep, health, and working patterns: a survey study of US health care workers. J Clin Sleep Med 17(2):185–191
Hallman DM, Januario LB, Mathiassen SE, Heiden M, Svensson S, Bergström G (2021) Working from home during the COVID-19 outbreak in Sweden: effects on 24‑h time-use in office workers. Bmc Public Health 21(1):1–10
Hirschwald B, Sun Y, Nold A, Bochmann F (2022) Personal factors influencing daytime sleepiness. Zbl Arbeitsmed: 1–7. https://doi.org/10.1007/s40664-022-00459-9
Korman M, Tkachev V, Reis C, Komada Y, Kitamura S, Gubin D, Roenneberg T (2020) COVID-19-mandated social restrictions unveil the impact of social time pressure on sleep and body clock. Sci Rep 10(1):1–10
Leone MJ, Sigman M, Golombek DA (2020) Effects of lockdown on human sleep and chronotype during the COVID-19 pandemic. Curr Biol 30(16):R930–R931
Raman S, Coogan AN (2022) Effects of societal-level COVID-19 mitigation measures on the timing and quality of sleep in Ireland. Sleep Med 91:179–184
Staller N, Randler C (2021) Changes in sleep schedule and chronotype due to COVID-19 restrictions and home office. Somnologie 25:131–137. https://doi.org/10.1007/s11818-020-00277-2
Staller N, Kalbacher L, Randler C (2022) Impact of pandemic lockdown on learning behaviour and sleep quality in German students. Somnologie 26:98–105. https://doi.org/10.1007/s11818-022-00346-8
Vollmer C, Jankowski KS (2022) COVID-19-lockdown delayed sleep timing in Tyrolean teachers. Chronobiol Int 39(12):1601–1610
Khan S, Duan P, Yao L, Hou H (2018) Shiftwork-mediated disruptions of circadian rhythms and sleep homeostasis cause serious health problems. Int J Genomics 2018. https://doi.org/10.1155/2018/8576890
Huang T, Mariani S, Redline S (2020) Sleep irregularity and risk of cardiovascular events: the multi-ethnic study of atherosclerosis. J Am Coll Cardiol 75(9):991–999
Ramírez-Contreras C, Zerón-Rugerio MF, Izquierdo-Pulido M (2022) Life before and after COVID-19: the ‘new normal’benefits the regularity of daily sleep and eating routines among college students. Nutrients 14(2):351
Nestler S, Böckelmann I (2022) Einfluss der Bildschirmzeit auf die Schlafqualität Studierender. Somnologie: 1–8. https://doi.org/10.1007/s11818-022-00357-5
Saxena R, Parmar N, Prabhleen K, Allen T (2021) Effect of screen-time on sleep pattern and dietary habits among college-going students in COVID-19 pandemic. Indian J Community Health 33:1
Korman M, Tkachev V, Reis C, Komada Y, Kitamura S, Gubin D, Roenneberg T (2022) Outdoor daylight exposure and longer sleep promote wellbeing under COVID-19 mandated restrictions. J Sleep Res 31(2):e13471
Randler C, Tryjanowski P, Jokimäki J, Kaisanlahti-Jokimäki ML, Staller N (2020) SARS-CoV2 (COVID-19) Pandemic lockdown influences nature-based recreational activity: The case of birders. IJERPH 17(19):7310
Randler C, Díaz-Morales JF, Rahafar A, Vollmer C (2016) Morningness–eveningness and amplitude–development and validation of an improved composite scale to measure circadian preference and stability (MESSi). Chronobiol Int 33(7):832–848
Mitchell JA, Quante M, Godbole S, James P, Hipp JA, Marinac CR, Kerr J (2017) Variation in actigraphy-estimated rest-activity patterns by demographic factors. Chronobiol Int 34(8):1042–1056
Cole RJ, Kripke DF, Gruen W, Mullaney DJ, Gillin JC (1992) Automatic sleep/wake identification from wrist activity. Sleep 15(5):461–469
Troiano RP, Berrigan D, Dodd KW, Masse LC, Tilert T, McDowell M (2008) Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc 40(1):181
Roenneberg T, Kuehnle T, Pramstaller PP, Ricken J, Havel M, Guth A, Merrow M (2004) A marker for the end of adolescence. Curr Biol 14(24):R1038–R1039
Zavada A, Gordijn MC, Beersma DG, Daan S, Roenneberg T (2005) Comparison of the Munich chronotype questionnaire with the Horne-Östberg’s morningness-eveningness score. Chronobiol Int 22(2):267–278
Wittmann M, Dinich J, Merrow M, Roenneberg T (2006) Social jetlag: misalignment of biological and social time. Chronobiol Int 23(1–2):497–509
pyActigraphy (2022) https://www.researchgate.net/publication/355770176_pyActigraphy_Open-source_python_package_for_actigraphy_data_visualization_and_analysis. Accessed 12 Nov 2022
McKinney W (2012) Python for data analysis: Data wrangling with Pandas, NumPy, and IPython. O’Reilly Media, Inc
Randler C, Faßl C, Kalb N (2017) From Lark to Owl: developmental changes in morningness-eveningness from new-borns to early adulthood. Sci Rep 7(1):1–8
Roenneberg T, Kuehnle T, Juda M, Kantermann T, Allebrandt K, Gordijn M, Merrow M (2007) Epidemiology of the human circadian clock. Sleep Med Rev 11(6):429–438
Caliandro R, Streng AA, van Kerkhof LW, van der Horst GT, Chaves I (2021) Social jetlag and related risks for human health: A timely review. Nutrients 13(12):4543
Randler C, Vollmer C, Kalb N, Itzek-Greulich H (2019) Breakpoints of time in bed, midpoint of sleep, and social jetlag from infancy to early adulthood. Sleep Med 57:80–86
Choi SJ, Joo EY, Hong SB (2016) Sleep–wake pattern, chronotype and seizures in patients with epilepsy. Epilepsy Res 120:19–24
Hayes JF, Schumacher LM, Lanoye A, LaRose JG, Tate DF, Espeland MA, Wing RR (2022) Persistent, high levels of social jetlag predict poor weight outcomes in a weight gain prevention study for young adults. J Behav Med 45(5):794–803
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
N. Staller, M. Quante, H. Deutsch, and C. Randler declare that they have no competing interests.
For this article no studies with animals were performed by any of the authors. All studies mentioned were in accordance with the ethical standards indicated in each case.
Additional information

Supplementary material online – scan QR code
Supplementary Information
11818_2023_408_MOESM1_ESM.docx
Supplement 1 (Fig. 1: Distribution of the corrected midpoint of sleep as a chronotype measure in the onsite group; Fig. 2: Distribution of the corrected midpoint of sleep as a chronotype measure in the home-office group), Supplement 2 (Table: Comparison of age and social jetlag with literature)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Staller, N., Quante, M., Deutsch, H. et al. Onsite versus home-office: differences in sleep patterns according to workplace. Somnologie 27, 272–279 (2023). https://doi.org/10.1007/s11818-023-00408-5
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11818-023-00408-5