
Abstract
Objectives
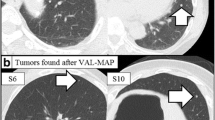
Virtual-assisted lung mapping is a preoperative bronchoscopic multi-spot dye-marking technique used in sublobar lung resection for hardly palpable lung nodules. However, the number of marks required per nodule remains unknown. Therefore, we examined the correlation between the number of intraoperative visible marks and the successful resection rate.
Methods
We retrospectively examined 210 consecutive patients with 256 lesions who underwent virtual-assisted lung mapping during January 2014–December 2020 at our hospital. When a nodule was not resected at the initial attempt, or when a nodule was very close to the cut margin in the resected specimen and required additional resection, we categorized it as unsuccessful resection. We divided 256 lesions into successful and unsuccessful groups and compared the numbers of intraoperative visible marks between the two groups.
Results
Of 797 attempted marks, 738 (92.4%) were visible during the surgery. Fourteen (5.4%) of 256 lesions were determined to be unsuccessful according to the study criteria. There was a remarkable difference in the average numbers of intraoperative visible marks between both groups (3 [interquartile range: 2–4] vs. 2 [interquartile range: 1–2.8]; p < 0.01). Multivariable logistic analysis revealed a significant difference in the number of intraoperative visible marks (odds ratio: 0.28, 95% confidence interval: 0.14–0.57; p < 0.001) between both groups.
Conclusions
Successful sublobar lung resection requires three or more intraoperative visible marks established using virtual-assisted lung mapping per lung nodule.



Similar content being viewed by others


Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
- CT:
-
Computed tomography
- ENB:
-
Electromagnetic navigation bronchoscopy
- VAL-MAP:
-
Virtual-assisted lung mapping
- VATS:
-
Video-assisted thoracic surgery
References
National Lung Screening Trial Research T, Aberle DR, Adams AM, Berg CD, Black WC, Clapp JD et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med 2011;365:395–409.
Bendixen M, Jorgensen OD, Kronborg C, Andersen C, Licht PB. Postoperative pain and quality of life after lobectomy via video-assisted thoracoscopic surgery or anterolateral thoracotomy for early stage lung cancer: a randomised controlled trial. Lancet Oncol. 2016;17:836–44.
Yang HX, Woo KM, Sima CS, Bains MS, Adusumilli PS, Huang J, et al. Long-term survival based on the surgical approach to lobectomy for clinical stage I nonsmall cell lung cancer: comparison of robotic, video-assisted thoracic surgery, and thoracotomy lobectomy. Ann Surg. 2017;265:431–7.
Saji H, Okada M, Tsuboi M, Nakajima R, Suzuki K, Aokage K, et al. Segmentectomy versus lobectomy in small-sized peripheral non-small-cell lung cancer (JCOG0802/WJOG4607L): a multicentre, open-label, phase 3, randomised, controlled, non-inferiority trial. Lancet. 2022;399:1607–17.
Blasberg JD, Pass HI, Donington JS. Sublobar resection: a movement from the lung cancer Study Group. J Thorac Oncol. 2010;5:1583–93.
Sato M, Omasa M, Chen F, Sato T, Sonobe M, Bando T, et al. Use of virtual assisted lung mapping (VAL-MAP), a bronchoscopic multispot dye-marking technique using virtual images, for precise navigation of thoracoscopic sublobar lung resection. J Thorac Cardiovasc Surg. 2014;147:1813–9.
Ichinose J, Kohno T, Fujimori S, Harano T, Suzuki S. Efficacy and complications of computed tomography-guided hook wire localization. Ann Thorac Surg. 2013;96:1203–8.
Yanagiya M, Sato M, Ueda K, Nagayama K, Kawahara T, Kawashima S, et al. Preoperative lung surface localization for pulmonary wedge resection: a single-center experience. J Thorac Dis. 2020;12:2129–36.
Sato M, Kuwata T, Yamanashi K, Kitamura A, Misawa K, Imashimizu K, et al. Safety and reproducibility of virtual-assisted lung mapping: a multicentre study in Japan. Eur J Cardiothorac Surg. 2017;51:861–8.
Sato M, Kobayashi M, Kojima F, Tanaka F, Yanagiya M, Kosaka S, et al. Effect of virtual-assisted lung mapping in acquisition of surgical margins in sublobar lung resection. J Thorac Cardiovasc Surg. 2018;156(1691–701): e5.
Yamanashi K, Sato M, Marumo S, Fukui T, Sumitomo R, Shoji T, et al. Emphysematous lungs do not affect visibility of virtual-assisted lung mapping. Asian Cardiovasc Thorac Ann. 2016;24:152–7.
Sato M, Shinohara Y, Yanagiya M, Karasaki T, Kitano K, Nagayama K, et al. Use of electromagnetic navigation bronchoscopy in virtual-assisted lung mapping: the effect of on-site adjustment. Gen Thorac Cardiovasc Surg. 2019;67:1062–9.
Sato M, Yamada T, Menju T, Aoyama A, Sato T, Chen F, et al. Virtual-assisted lung mapping: outcome of 100 consecutive cases in a single institute. Eur J Cardiothorac Surg. 2015;47:e131–9.
Kanda Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transplant. 2013;48:452–8.
Sato M, Aoyama A, Yamada T, Menjyu T, Chen F, Sato T, et al. Thoracoscopic wedge lung resection using virtual-assisted lung mapping. Asian Cardiovasc Thorac Ann. 2015;23:46–54.
Yoshiyasu N, Sato M, Yamaguchi H, Nakajima J. Risk factors for invisible intraoperative markings after virtual-assisted lung mapping. Ann Thorac Surg. 2021;114:1903.
Yanagiya M, Sato M, Ijiri N, Kobayashi K, Nagano M, Konoeda C, et al. Virtual-assisted lung mapping using dual staining with indocyanine green and indigo carmine enhanced marking detectability. J Thorac Dis. 2022;14:1061–9.
Sato M, Kobayashi M, Sakamoto J, Fukai R, Takizawa H, Shinohara S, et al. The role of virtual-assisted lung mapping 2.0 combining microcoils and dye marks in deep lung resection. J Thorac Cardiovasc Surg. 2022;164:243-51e5.
Yamaguchi H, Sato M, Yamamoto K, Ueda K, Date H, Chen-Yoshikawa T, et al. Virtual-assisted lung mapping in sublobar resection of small pulmonary nodules, long-term results. Eur J Cardiothorac Surg. 2022;61:761–8.
Acknowledgements
The authors would like to thank Enago (https://www.enago.jp) for the English language review.
Funding
This study did not receive any funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None declared.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Nagano, M., Sato, M., Yanagiya, M. et al. Number of dye marks required in virtual-assisted lung mapping. Gen Thorac Cardiovasc Surg 71, 313–320 (2023). https://doi.org/10.1007/s11748-022-01896-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11748-022-01896-2