
Abstract
Objectives
We classified pathological stage I invasive lung adenocarcinomas according to our 3-tier classification, which was based on the proportion of invasive morphological patterns as follows: (1) patients with each predominant subtype, (2) those with a minor histological subtype, even not the predominant subtype and (3) those without each invasive component. We aimed to evaluate the classification's clinical impact in survival, recurrence, malignant grade, and epidermal growth factor receptor (EGFR) mutational status.
Materials and methods
A total of 1,269 patients with p-stage I lung adenocarcinoma underwent curative surgical resection between January 2008 and December 2017. Of these, 620 patients (48.9%) met the inclusion criteria of this study.
Results
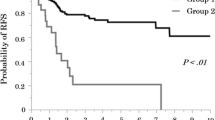
Postoperative recurrence was observed in 81 patients (13.1%). Multivariate analysis showed that vascular invasion (hazard ratio, 2.61; p < 0.001) and p-stage IB (hazard ratio, 2.19; p = 0.001) were significantly associated with an unfavorable RFS, while the presence of acinar component (hazard ratio, 1.64; p = 0.052) or solid component (hazard ratio, 1.60; p = 0.074) were marginally significant. The presence of lepidic or papillary component and the absence of acinar or solid component significantly correlated with an increased proportion of lung adenocarcinomas harboring EGFR mutations.
Conclusion
In patients with p-stage I invasive lung adenocarcinoma, it is beneficial to use not only the predominant subtype but analyzing the extent of each histological component based on our classification to predict patient prognoses and form appropriate postoperative follow-up methods.




Similar content being viewed by others
References
Travis WD, Brambilla E, Noguchi M, et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. J Thorac Oncol Off Publ Int Assoc Study Lung Cancer. 2011;6(2):244–85.
Yoshizawa A, Motoi N, Riely GJ, et al. Impact of proposed IASLC/ATS/ERS classification of lung adenocarcinoma: prognostic subgroups and implications for further revision of staging based on analysis of 514 stage I cases. Mod Pathol Off J US Can Acad Pathol. 2011;24(5):653–64.
Kadota K, Villena-Vargas J, Yoshizawa A, et al. Prognostic significance of adenocarcinoma in situ, minimally invasive adenocarcinoma, and nonmucinous lepidic predominant invasive adenocarcinoma of the lung in patients with stage I disease. Am J Surg Pathol. 2014;38(4):448–60.
Strand TE, Rostad H, Strom EH, Hasleton P. The percentage of lepidic growth is an independent prognostic factor in invasive adenocarcinoma of the lung. Diagn Pathol. 2015;10:94.
Shim HS, Lee DH, Park EJ, Kim SH. Histopathologic characteristics of lung adenocarcinomas with epidermal growth factor receptor mutations in the International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society lung adenocarcinoma classification. Arch Pathol Lab Med. 2011;135(10):1329–34.
Chen Z, Liu X, Zhao J, Yang H, Teng X. Correlation of EGFR mutation and histological subtype according to the IASLC/ATS/ERS classification of lung adenocarcinoma. Int J Clin Exp Pathol. 2014;7(11):8039–45.
Dearden S, Stevens J, Wu YL, Blowers D. Mutation incidence and coincidence in non small-cell lung cancer: meta-analyses by ethnicity and histology (mutMap). Ann Oncol Off J Eur Soc Med Oncol. 2013;24(9):2371–6.
Midha A, Dearden S, McCormack R. EGFR mutation incidence in non-small-cell lung cancer of adenocarcinoma histology: a systematic review and global map by ethnicity (mutMapII). Am J Cancer Res. 2015;5(9):2892–911.
Yanagawa N, Shiono S, Abiko M, Katahira M, Osakabe M, Ogata SY. The clinical impact of solid and micropapillary patterns in resected lung adenocarcinoma. J Thorac Oncol Off Publ Int Assoc Study Lung Cancer. 2016;11(11):1976–83.
Ito M, Miyata Y, Yoshiya T, et al. Second predominant subtype predicts outcomes of intermediate-malignant invasive lung adenocarcinomadagger. Eur J Cardio Thorac Surg Off J Eur Assoc Cardio Thorac Surg. 2017;51(2):218–22.
Zhang Y, Sun Y, Pan Y, et al. Frequency of driver mutations in lung adenocarcinoma from female never-smokers varies with histologic subtypes and age at diagnosis. Clin Cancer Res Off J Am Assoc Cancer Res. 2012;18(7):1947–53.
Dong YJ, Cai YR, Zhou LJ, et al. Association between the histological subtype of lung adenocarcinoma, EGFR/KRAS mutation status and the ALK rearrangement according to the novel IASLC/ATS/ERS classification. Oncol Lett. 2016;11(4):2552–8.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing financial interests associated with this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
About this article

Cite this article
Osawa, J., Shimada, Y., Maehara, S. et al. Clinical usefulness of the 3-tier classification according to the proportion of morphological patterns for patients with pathological stage I invasive lung adenocarcinoma. Gen Thorac Cardiovasc Surg 69, 943–949 (2021). https://doi.org/10.1007/s11748-020-01559-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11748-020-01559-0