
Abstract
Objectives
We investigated the hypothesis that early surgery for infective endocarditis (IE) attenuates the rate of death or embolic events and does not increase the rate of relapse or postoperative valvular dysfunction (PVD) at 6 months.
Methods
21 consecutive patients who underwent surgical treatment of IE were prospectively included. We assessed 6-month postoperative clinical outcomes by comparing early surgery (Group E, surgery within 72 h) and conventional treatment (Group C). Nine patients (43%) were assigned to Group E based on a combination of preoperative evaluation parameters, including the findings of cerebral magnetic resonance imaging (MRI), which was performed in all patients with left-sided IE.
Results
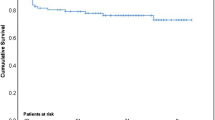
Six surgical plans (5 advancements and 1 postponement) were modified by routine MRI. Although preoperative echocardiography did not confirm all annular invasions, the rate of periannular infection, which was treated by pericardial annular patch plasty (56%) in patients with native-valve IE, was higher in Group E than C (P = 0.006). Early surgery based on MRI findings resulted in no postoperative embolic events or cerebral bleeding. The 6-month mortality rate was 0% in both groups, although the calculated 6-month IE mortality rate was 49.2 ± 25% and 28.8 ± 18%, respectively. No recurrence of IE or PVD occurred in Group E. The 6-month rate of freedom from composite events was 100% in Group E.
Conclusions
Aggressive treatment (periannular resection and disuse of a prosthetic annuloplasty ring) and optimal antibiotic therapy based on intraoperative microorganisms, even in patients who underwent early surgery, reduced the 6-month relapse and PVD rates.


Similar content being viewed by others

References
David TE, Gavra G, Feindel CM, Regesta T, Armstrong S, Maganti MD. Surgical treatment of active infective endocarditis: a continued challenge. J Thorac Cardiovasc Surg. 2007;133:144–9.
Olmos C, Vilacosta I, Habib G, Maroto L, Fernandez C, López J, et al. Risk score for cardiac surgery in active left-sided infective endocarditis. Heart. 2017;103:1435–42. https://doi.org/10.1136/heartjnl-2016-311093.
Park LP, Chu VH, Peterson G, Skoutelis A, Lejko-Zupa T, Bouza E, et al. Validated risk score for predicting 6-month mortality in infective endocarditis. J Am Heart Assoc. 2016;5:e003016. https://doi.org/10.1161/JAHA.115.003016.
Bonow RO, Carabello B, Chatterjee K, de Leon AC, Faxon DP, Freed MD, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 Guidelines for the Management of Patients with Valvular Heart Disease). Circulation. 2006;114:e84–231 (Errata, Circulation 2007;115:e409, 2010;121:e443).
Thuny F, Beurtheret S, Mancini J, Gariboldi V, Casalta JP, Riberi A, et al. The timing of surgery influences mortality and morbidity in adults with severe complicated infective endocarditis: a propensity analysis. Eur Heart J. 2011;32:2027–33.
Habib G, Hoen B, Tornos P, Thuny F, Prendergast B, Vilacosta I, et al. Guidelines on the prevention, diagnosis, and treatment of infective endocarditis (new version 2009): the task force on the prevention, diagnosis, and treatment of infective endocarditis of the European Society of Cardiology (ESC). Endorsed by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and the International Society of Chemotherapy (ISC) for Infection and Cancer. Eur Heart J. 2009;30:2369–413.
Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, et al. ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J. 2015;36:3075–128. https://doi.org/10.1093/eurheartj/ehv319.
Thuny F, Avierinos JF, Tribouilloy C, Giorgi R, Casalta JP, Milandre L, et al. Impact of cerebrovascular complications on mortality and neurologic outcome during infective endocarditis: a prospective multicentre study. Eur Heart J. 2007;28:1155–61.
Kang DH, Kim YJ, Kim SH, Sun BJ, Kim DH, Yun SC, et al. Early surgery versus conventional treatment for infective endocarditis. N Engl J Med. 2012;366:2466–73.
Duval X. Iung B. Klein I. Brochet E. Thabut G. Arnoult F, for the IMAGE (Resonance Magnetic Imaging at the Acute Phase of Endocarditis) Study Group, et al. Effect of early cerebral magnetic resonance imaging on clinical decisions in infective endocarditis: a prospective study. Ann Intern Med. 2010;152:497–504.
Chakraborty T, Scharf E, Rabinstein AA, DeSimone D, El Rafei A, Brinjikji W, et al. Utility of brain magnetic resonance imaging in the surgical management of infective endocarditis. J Stroke Cerebrovasc Dis. 2017;26:2527–35.
Hasbun R, Vikram HR, Barakat LA, Buenconsejo J, Quagliarello VJ. Complicated left-sided native valve endocarditis in adults: risk classification for mortality. JAMA. 2003;289:1933–40.
Ruttmann E, Legit C, Poelzl G, Mueller S, Chevtchik O, Cottogni M, et al. Mitral valve repair provides improved outcome over replacement in active infective endocarditis. J Thorac Cardiovasc Surg. 2005;130:765–71.
Couetil JP, Argyriadis PG, Shafy A, Cohen A, Berrebi AJ, Loulmet DF, et al. Partial replacement of the tricuspid valve by mitral homografts in acute endocarditis. Ann Thorac Surg. 2002;73:1808–12.
Fowler VG Jr, Miro JM, Hoen B, Cabell CH, Abrutyn E, Rubinstein E, et al. Staphylococcus aureus endocarditis: a consequence of medical progress. JAMA. 2005;293:3012–21.
Acknowledgements
We thank Angela Morben, DVM, ELS, from Edanz Group (http://www.edanzediting.com/ac), for editing a draft of this manuscript. We also thank Terae Satoshi, a radiologist in Sapporo City General Hospital, for providing advice regarding the MRI findings.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.
Rights and permissions
About this article

Cite this article
Nakamura, M., Uzuka, T., Sato, H. et al. Early surgery with aggressive surgical approach to improve 6-month outcomes in patients with active infective endocarditis: contribution of cerebral preoperative magnetic resonance imaging. Gen Thorac Cardiovasc Surg 67, 427–435 (2019). https://doi.org/10.1007/s11748-018-1040-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11748-018-1040-9